

Abstract
Background:
The incidence of anemia rises with age. The consequences of anemia are many and serious, affecting not only individual's health, but also the development of societies and countries. Pandu Roga can be effectively compared with anemia on the ground of its similar signs and symptoms.
Aim:
To evaluate the Panduhara and Rasayana effect of Punarnava Mandura in the management of Pandu Roga in old age (geriatric anemia).
Materials and Methods:
The study was conducted in 50 clinically diagnosed patients of geriatric anemia. Patients were treated with Punarnava Mandura 2 tablets (250 mg each) twice in a day after lunch and dinner with Takra (butter milk) for 90 days. Among 50 registered patients, 40 patients had completed the treatment and 10 patients discontinued the treatment. Results were analyzed using Wilcoxon signed-rank test for subjective parameters and for assessment of objective parameters paired t-test was adopted.
Results:
At the end of study, drug has shown beneficial effect in patients of anemia by providing highly significant result in chief complaints, associated symptoms, Kshaya of Dhatu and Agni Bala, Deha Bala and Sattwa Bala. It has also improved quality-of-life (QOL) of the patients. Moderate and mild improvement was observed in 30 and 70% of the patients respectively.
Conclusion:
Punarnava Mandura may work as Rasayana in geriatric anemia by providing highly significant results on clinical features of Pandu Roga, Dehabala, Agni Bala and Sattwa Bala and by improving QOL. of patients of geriatric anemia.
Keywords: Anemia, geriatric, Pandu, Punarnava Mandura
Introduction
Anemia is common in old age and increases the risk of physical disability, associated with impaired performance and muscle weakness and has been shown to affect older person's physical function.[1] Anemia should not be accepted as an inevitable consequence of aging.[2] The potential negative impact of a low hemoglobin (Hb) level on performance status, physiology, and functional independence appear to be highest in elderly patients.[3]
Acharya Sushruta opines that there is a decline of Sarva Dhatu (tissue), Indriya (sensory-motor system), Bala (strength), Virya (virility) after Sampurnavastha.[4] Acharya Charaka also considered “Bhrishyamana Dhatu Guna” (successive decrease in the qualities of Dhatu). Thus, it is clear from the Charaka's view that both qualitative and quantitative decrease in Dhatu occurs during old age. Bhela Samhita throws further light in this regard. In old age, the capacity for Viveka (discretion of assimilated nutrients into Dhatu) is hampered due to Kshaya of Dhatu. Therefore, the replacement of Dhatu is also reduced as a result of already existing vitiation.[5]
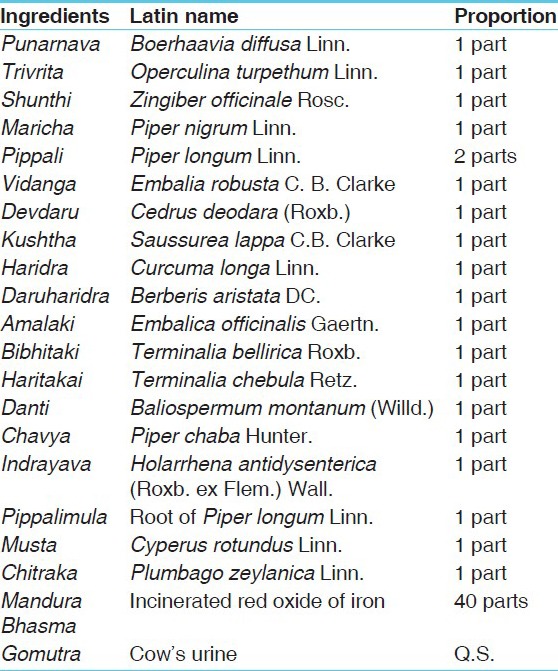
On looking at the ingredients of Punarnava Mandura,[6] [Table 1], it may work in above context by its effect on Srotasa (micro channels) and Agni (digestive fire mechanism) by enhancing digestive capacity as a result of their Deepana (appetizer), Pachana (digestive) properties. Hence, thereby curing the disease (Pandu) and promoting immunity of the body in old age.
Table 1.
Ingredients of Punarnava Mandura
Considering the above facts that is, higher prevalence of anemia, negative impacts in older individuals, it is important to deal with such type of disease. Further Punarnava Mandura, which is considered as an efficacious drug, being successfully prescribed by Ayurvedic physicians for the management of Pandu and lot of work have been done on it, but till date no work has been reported in geriatric anemia.[7,8,9,10]
Aims and objectives
To evaluate Panduhara and Rasayana effect of Punarnava Mandura on the patients of Pandu in old age.
Materials and Methods
Patients fulfilling the criteria for the diagnosis of the disease were registered for the present study between the age group of 50 and 80 years irrespective of sex, religion, occupation, etc., The patients were selected from the outpatient department of Kayachikitsa, Institute for Postgraduate Teaching and Research in Ayurveda, Gujarat Ayurved University, Jamnagar. Out of total 50 selected patients, 40 patients completed, while 10 patients discontinued the treatment due to personal reasons or migration. The study was cleared by the Institutional Ethics Committee vide letter no. PGT/7/Ethics/2009–2010/3494/15 dated 8/2/2010. Informed consent was taken from all the patients before including them in the trial.
Criteria for selection of patients
Inclusion criteria
Patients between the age group 50 and 80 years
Patients having cardinal symptoms of Pandu, that is., Panduta (pallor), Shrama (fatigue), Bhrama (vertigo), Pindikodveshtana (calf muscle pain), Daurbalya (general weakness), Ayasaja Shwasa (exertional dyspnoea), etc
Patients having Hb% below the normal range (in men: 7–13 g/dl and in female: 7–12 g/dl).[11]
It is a common perception that Hb level lower than reference values are acceptable in older individuals. However, most experts recommend using the same reference values for Hb in older persons as are used in younger individuals.[12] Hence, in present study same criterion is adopted.
Exclusion criteria
Patients suffering from systemic diseases like diabetes mellitus (DM), renal disorders, heart disease, cancer, acquired immune-deficiency syndrome, tuberculosis., hypertension, and having bleeding disorders
Patients having anemia due to chronic diseases, including inflammatory disease, malignancy and chronic infection or blood loss
Age <50 years and more than 80 years
Hb% level-below 7 g/dl
Anemia in a case of defective absorption due to gastrectomy, sprue syndrome etc.
Patients were diagnosed and assessed thoroughly on the basis of Ayurvedic classical signs and symptoms of Pandu and examined on the basis of specially prepared proforma.
Laboratory investigations
Complete hemogram: Hb%, total leucocyte count (TLC), differential leucocyte count (DLC), erythrocyte sedimentation rate (ESR), and packed cell volume (PCV), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), platelet count and peripheral smear
-
Blood biochemistry: Serum iron, total iron binding capacity (TIBC)
- Serum glutamic pyruvic transaminase (to rule out liver disease), blood sugar (to rule out DM), blood urea and serum creatinine (to assess the functional status of kidney).
Urine and stool: Routine and microscopic examination of urine and stool was done to detect presence of any blood, mucus, ova, cyst etc.
These investigations were done in all the patients before treatment and after completion of treatment.
Criteria for assessment
Assessment was done by considering change in the subjective as well as the objective parameters before the treatment and after the treatment. Patients were assessed clinically every 15 days for evaluation of improvement for a period of 90 days. The changes observed in the signs and symptoms were assessed by adopting suitable scoring method and the objective signs by using appropriate clinical tools.
Criteria for the assessment of overall effect of therapy
The total effect of the therapy was assessed as follows:
Complete remission: 100% relief was considered as complete remission
Marked improvement: 76–99% relief was considered as markedly improvement
Moderate improvement: 51–75% relief was considered as markedly improvement
Mild improvement: 25–50% relief will be considered as markedly improvement
Unchanged: Below 25% relief was considered as unchanged.
Follow-up study
After the completion of 90 days of treatment, all the patients were kept under observation for 1-month. During the follow-up study, further improvement or deterioration or no change in the signs and symptoms was recorded.
Plan of treatment
Patients were given 2 tablets (250 mg each) of Punarnava Mandura twice a day after lunch and dinner with the Anupana of 100 ml of Takra (freshly prepared butter milk) for the duration of 90 days.
Drug detail
All the raw drugs of Punarnava Mandura were procured from Pharmacy, Gujarat Ayurved University, Jamnagar. The correct identity and authenticity of raw materials were confirmed by studying its organoleptic and powder microscopy then comparing them with the characters mentioned in Ayurvedic Pharmacopoiea of India (API). Later, subject experts of Pharmacognosy Department further confirmed identification.
Statistical analysis
The Wilcoxon signed-rank test is a nonparametric statistical hypothesis test for assessment of subjective parameters.[17] To make calculations easy and without manual errors GraphPad Instat 3.06 (Inc, San Diego California, USA) was used. For assessment of objective parameters paired t-test was adopted and software used for paired t-test was SigmaState 3.5 (SSI, 501, Richmond, CA).
Observations
Maximum number of patients, that is, 70% belonged to the age group of 50–60 years. Majority of patients, that is, 90% were female, 86% patients were Hindu, 86% were married, 62% patients were housewives, 50% were from poor socioeconomic group. Maximum numbers of patient had Vata-Pitta Prakriti (46%) followed by Pitta-Kapha Prakriti (34%) and 100% had Rajasika Sattwika, Manasa Prakriti, Avara Sattwa (52%), Avara Sara (46%), Madhyama Samhanana (52%) and 37.62% patients had attained menopause.
Most of the patients (38%) were found to be indulged in intake of excessive Amla (sour) - Lavana (salty) Rasa (taste), 70% patients were doing intake of less nutritive food, 40% patients were taking food at irregular period as well as in excess or in less quantity than required and 84% patients were addicted to Tea. As per Viharatmaka Nidana, Ati Vyayama (heavy physical work) was reported in 60%, Vidagdhe Anne Vyayama (exercise even before food is not properly digested) in 34%, Vidagdhe Anne Divaswapna (sleep even before food is not properly digested) in 32%, Vegavidharana (suppression of natural urges) in 72%, Ratrijagarana (awakening at night) in 51%, disturbed sleep (32%) patients were observed. Manasika Nidana like Chinta (tension) and Krodha (anger) were observed in 70% patients and 16% patients had Shoka (grief).
In cardinal symptom Daurbalya (general weakness), Panduta (pallor) and Hridspandana (palpitation) were observed in all the patients, that is, 100%, followed by Shrama (fatigue) in 98% of patients. Ayasaja Shwasa (exertional dyspnoea), Bhrama (vertigo), Aruchi (loss of appetite) and Jwara (fever) were found in 96%, 88%, 70% and 56% respectively. Among associated symptoms all the patients, that is, 100% were Hataprabha (lusterlessness). While, Kati-Pada-Ururuk (pain in lower limb), Gaurava (heaviness) and Alasya (lethargy) were noticed in 94%, 82% and 78% of the patients respectively. Kopanatwa (irritability) was found in 76% patients. The 54% patients had Atinidra (excessive sleep), while 52% patients had complaint of Karnakshweda (ringing in the ear). Sthivana (excessive salivation) and Shirnaloma (hair falling) were noticed in 66% and 40% patients respectively.
Constipation was found in 58% of the patients in present study. 52% of the patients had diminished capacity to ingest the food followed by less appetite (48%). Rasa Kshaya and Majja Kshaya were found in all the patients. While Mamsa Kshaya and Meda Kshaya were noticed in 98% and 88% patients respectively. Whereas, Asthi Kshaya was found in 84% patients.
Most of the patients, that is, 54% patients had dimorphic anemia and 42% patients had microcytic hypochromic anemia and only 4% had maculo ovulocytic anemia. Moderate pallor of conjunctiva was observed in 40% patients. Whereas moderate pallor of tongue and nail was found in 46% patients. Mild clubbing of nail was noticed in 62% patients of anemia. None of the patients had jaundice.
Results
Punarnava Mandura was found statistically highly significant (P < 0.0001) in all chief complaints, that is, Aruchi (95.38%), Daurbalya (94.59%), Pindikodwestana (93.46%), Jwara (80%) and Bhrama (82.43%) except in Akshikuta Shotha (29.63%) in which significant result was noticed [Table 2].
Table 2.
Effect of therapy on chief complaints on the patients of geriatric anemia

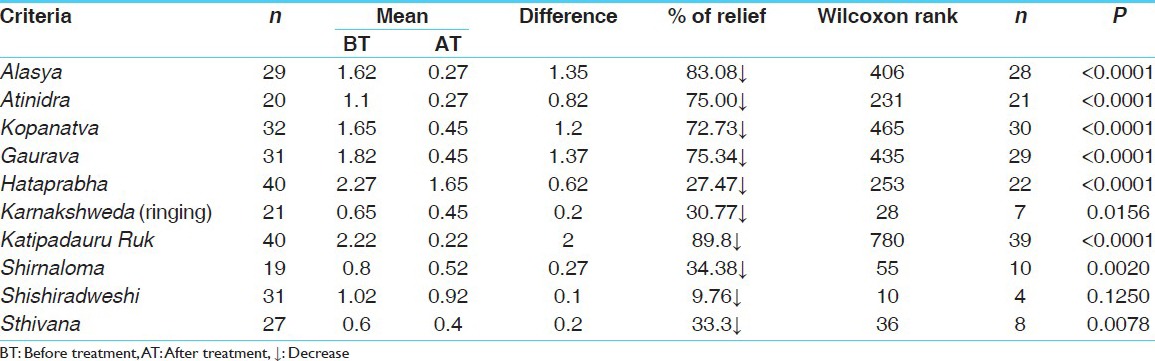
In associate symptoms, therapy showed highly significant decrease in Alasya (83.08%), Atinidra (75%), Kopanatwa (72.73%), Hataprabha (27.47%), Kati-pada-uru ruk (89.89%), Shirnaloma (34.38%) and Sthivana (33.33%). While in Shishiradweshi nonsignificant (P = 0.1250) result and in Karnakshweda significant relief were observed [Table 3].
Table 3.
Effect of therapy on associated symptoms on the patients of geriatric anemia
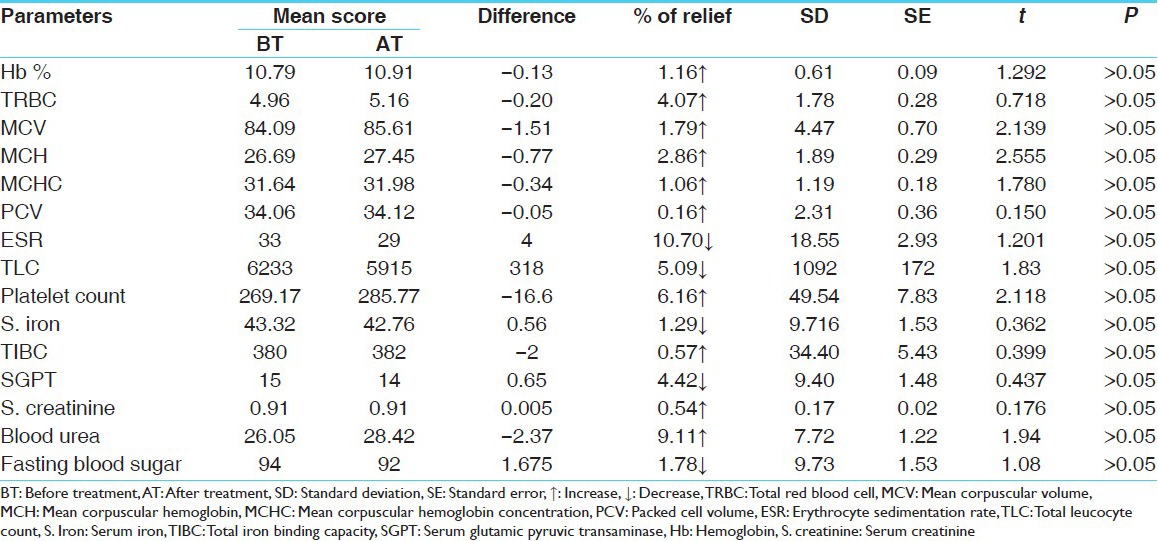
Statistically insignificant results were found in hematological parameters that is, Hb%, Total red blood cell (RBC), MCV, MCH, MCHC, PCV, ESR, platelet count and in biochemical parameters that is, serum iron, TIBC, Fasting blood sugar, serum creatinine and blood urea. ESR was decreased by 11.70%. ESR is increased in anemia and decrease in ESR is indicative of improvement in condition of the disease [Table 4].
Table 4.
Effect of therapy on laboratory investigations (n=40)
Study showed highly significant result in Agni Bala, Deha Bala and Sattwa Bala in the patients of Pandu Roga in old age [Table 5]. Further Punarnava Mandura showed statistically highly significant result in Kshaya (decrement) of all Dhatu except Rakta Dhatu in which nonsignificant result was observed [Table 6].
Table 5.
Effect of therapy on Agni Bala, Deha Bala and Sattwa Bala (n=40)
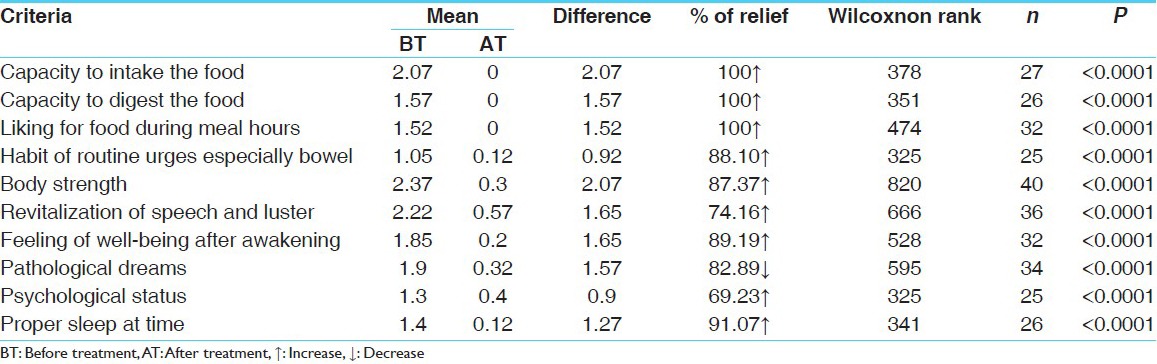
Table 6.
Effect of therapy on Sharira Upachaya (growth of body assessed by weight)

Observing the result of health, wellness and QOL questionnaire, it was found that physical stress and mental stress were relieved by 27.68–32.50% respectively. Whereas, life enjoyment and overall QOL were improved in 45.45–37.40% of the patients [Table 7].
Table 7.
Effect of therapy on health, wellness and QOL

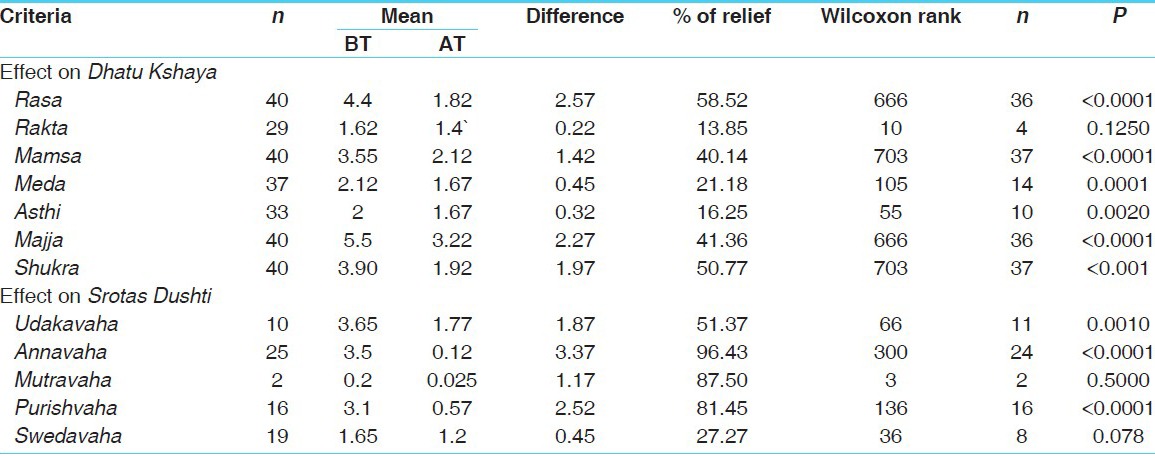
Study showed highly significant result in all the three types of Pandu i.e. Vatanubandha, Pittanubandha and Kaphanubandha Pandu [Table 8]. Punarnava Mandura provided highly significant result in Kshaya (decrement) of Dhatu except Rakta Dhatu [Table 9].
Table 8.
Effect of therapy on Doshanubandha Pandu

Table 9.
Effect of therapy on Dhatu Kshaya and Srotas Dushti
The overall effect of therapy shows that, maximum numbers of the patients that is, 70% got mild improvement and 30% patients showed moderate improvement. None of the patients remain unchanged. While marked improvement and complete remission was not found in any patient [Figure 1].
Figure 1.
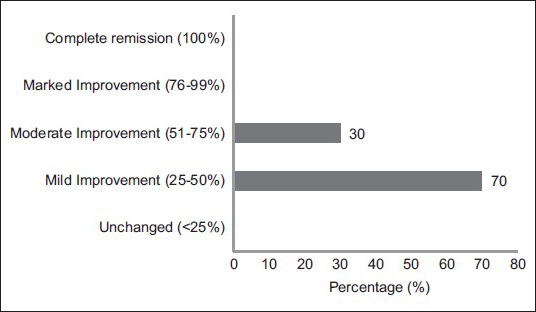
Overall effect of therapy on 40 patients of Pandu Roga in old age (geriatric anemia)
Discussion
There is no direct reference of incidence of Pandu Roga during old age. However, Ayurvedic texts have given comprehensive expression of age related Dhatu Kshaya which establish the prevalence of Pandu Roga in old age. Vata Vriddhi and Dhatu Kshaya in old age, starts a vicious cycle of Pandu, which makes it Kricchasadhya.
Nidana which were observed in maximum patients like awakening at night (51%), heavy physical work (60%), exercise even before food is not properly digested (34%), day sleep even before food is not properly digested (32%), suppression of natural urges (72%), uncompatible food (40%), excessive intake of sour-salt dominant diet (38%), low nutritive diet (70%) and addiction to tea (84%), tension (70%), anger (70%) play a major role in etiopathogenesis of Pandu during old age.
In the present study, majority of the patients that is 90% were female. A study also reveals the same fact that under age 75 years, anemia is more common in females.[18] Most of the patients were having Pitta-Vata and Pitta-Kapha Prakriti, so it may be inferred that persons with Pitta dominance may suffer from Pandu Roga more frequently than that of Vata or Kapha dominance and it may be recommended for the persons of Pitta dominance that to avoid disease like Pandu Roga they should have to keep away from Pitta vitiating factors.
It was observed that constipation was found in 58%, it may be due to reduced peristalsis of the colon in old age.[19] Microcytic hypochromic anemia that is iron deficiency anemia was found in 42% of the patients, which is supported by the fact that iron deficiency occurs in approximately 15-30% of elderly anemic patients.[20]
Maximum patients had diminished intake of food and impaired digestion, this signifies the disturbance of Agni that is Mandagni, it results into improper formation of Rasa Dhatu and subsequently Rakta Dhatu etc., also. Rajasika Sattwika Prakriti and Avara Sattwa were found in 100 and 52% patients respectively. These patients are more prone to tension, anger and disturbed sleep. Disturbance in Manasika Bhavas that is tension and anger etc., lead to improper digestion of food even after the taken diet is in proper quality and easily digestible.[21] Subsequently it results into improper formation of further Dhatus and produce disease.
Daurbalya and Ayasaja Shwasa (exertional dyspnoea) were found in 100% and 96% respectively. In anemia oxygen carrying capacity of RBC is diminished due to reduction in MCH and MCV. Hence, to supply the required amount of oxygen according to the tissue demand, heart has to do more work, so heart rate increases, tachycardia and palpitation occurs and respiratory rate also increases accordingly, and patients feel exertional dyspnoea.[22]
Improvement in Aruchi was 95%, may be due to appetizer, digestive, hepatoprotective properties of Trikatu,[23] Chitraka, Vidanga etc.[24]
Therapy showed highly significant result in all the parameters that is physical stress, mental stress, life enjoyment and overall QOL of health, Wellness and QOL questionnaire. It may be achieved due to antioxidant and immune modulator ingredients of Punarnava Mandura.
Statistically highly significant result was observed in Kshaya (decrement) of Dhatu except Rakta Dhatu. Rasayana drugs bear the property of antioxidant and work as free radical scavengers and thus beneficial in decrement of Dhatu found in geriatric anemia. Therapy showed highly significant result in Udakavaha, Annavaha, Purishavaha and Swedavaha Srotas Dushti [Table 9].
In assessment of Agni Bala, 100% improvement was noted in capacity to digest the food, capacity to intake the food and liking for food during meal hours, which may be due to appetizer, digestive and carminative properties of the drug. While 88.10% improvement was noted in habit of routine urges especially bowel [Table 5].
Vata Dosha plays crucial role in manifestation of Pandu Roga mainly Vyana Vayu has a relation with pathogenesis of Pandu Roga.[25] During old age the diminution of the Dhatu occurs with dominance of Vata Dosha.[26] It results in diminished function of the digestion and metabolism in old age. Further it results in improper production of consequent Rasa, Rakta etc., These can be counteracted by Punarnava Mandura which contains appetizer, digestive and immunomodulator drugs.
In assessment of Sattwa Bala, statistically highly significant improvement was found in feeling of wellbeing after awakening, pathological dreams and psychological status of patient and proper sleep at time in 89.19%, 82.89%, 69.23%, 91.07% respectively. While assessing Deha Bala, physical strength, revitalization of speech and luster and growth of body assessed by weight were improved in 87.37%, 74.16% and 0.23% of the patients respectively [Tables 5 and 6].
Probable mode of action
According to Ayurvedic literature, most of the drugs in Punarnava Mandura that is Triphala,[27] Trikatu,[28] Chitraka,[29] Vidanga[30] and Pippalimula[31] are having appetizer, digestive and carminative properties. Hence it improves digestive power and ultimately absorption of nutrition and drug also. The components like Trivrita,[32] Haritaki[33] and Danti[34] act as purgative/laxative which help in relieving constipation mainly found in old age. Haridra,[35] Amalaki,[36] Pippali,[37] Punarnava[38] and Trivrita[39] are thought to be Panduhara by various Acharyas. Other drugs that is Amalaki,[40] Danti,[41] Pippali,[42] Punarnava,[43] Kushtha[44] and Daruharidra[45] are documented as drugs which are having immunomodulator and antioxidant properties. Hence, they may have the potential to confer beneficial health effects due to their antioxidant activity and thus useful in geriatric anemia.
Amalaki possess antioxidant activity and could be an important dietary source of Vitamin C, which is a powerful water-soluble antioxidant[46] and helps in increasing iron absorption from the gut.[47] One study on Pippali suggests that, piperine gets absorbed very quickly across the intestinal barrier through the intracellular pathway. It may modulate membrane dynamics due to its easy partitioning thus helping in efficient permeability across the barriers.[48] In addition Pippali is said to be bio-availability enhancer of the drug,[49] which further helps in easy assimilation of the drug components. Hence, it counteracts poor digestion and absorption usually reported in patients of geriatric anemia. It has also immunomodulator activity.[50] Therefore it improves general health and immunity vigor, luster of the skin etc., in patients having anemia.
Mandura Bhasma (incinerate form of iron-Fe2O3), the main component is the activator of the formulation and is the chief responsible component for the pharmacodynamics of Punarnava Mandura. By virtue of Rasa and Guna it pacifies aggravated Pitta and maintains the normalcy, improves the digestion and metabolism. Looking in to the diversified actions, Acharya Charaka says that, Mandura and its preparations are vital in treating cases of Pandu. The ferric and ferrous fractions of Mandura provide sufficient amount of iron to the living matter, which is needed for normal erythropoiesis.[51]
As Gomutra (Cow's urine) is one ingredient of Punarnava Mandura, it works as Rasayana by its antioxidant property. It has been found to be a very good immune enhancer.[52] Presence of erythropoietin hormone in Cow's urine may be one of the reasons why Gomutra is useful in anemia. Iron present in Cow's urine maintains balance and helps in production of red blood cells and Hb.[53]
Further, the activity of Punarnava Mandura gets potentiated as it is to be administered with Takra (butter milk) as an adjuvant of which have therapeutic attributes Agnideepana (appetizer) and Panduhara (anti anemic) properties.[54]
Conclusion
Punarnava Mandura is a unique poly herbo mineral formulation which may work as a Panduhara and Rasayana in the patients of geriatric anemia and can counteract most of the pathological manifestations related to Pandu Roga in old age (geriatric anemia).
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Penninx BW, Pahor M, Woodman RC, Guralnik JM. Anemia in old age is associated with increased mortality and hospitalization. J Gerontol A Biol Sci Med Sci. 2006;61:474–9. doi: 10.1093/gerona/61.5.474. [DOI] [PubMed] [Google Scholar]
- 2.Smith DL. Anemia in the elderly American Family Physician Web archive, Published by American Academy of Family Physicians (AAFP), on October 1, 2000. [Last accessed on 2011, Jan 20]. Available from: http://www.aafp.org/afp/20001001/1565.html .
- 3.Gaskell H, Derry S, Andrew Moore R, McQuay HJ. Prevalence of anaemia in older persons: Systematic review. BMC Geriatric. 2008;8:1. doi: 10.1186/1471-2318-8-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kaviraj Ambikadatta Shastri., editor. Varanasi: Chaukhambha Sanskrit Sansthan; 2005. Sushruta, Sushruta Samhita, Sutra Sthana, Aturopakramaniya Adhyaya, 35/36. Reprint ed. 135. [Google Scholar]
- 5.Shukla D, Chandola HM. Thesis. Jamnagar: Manas Roga and Manovijnana Dept, IPGT and RA, Gujarat Ayurved University; 2007. Role of Manasika bhavas in Akalaja jara (ageing) and comparative study of its management with Guduchyadi and Bhrungaraja Rasayana", M.D. [Google Scholar]
- 6.Vaidya Jadavji Tirkamji Acharya., editor. 2nd ed. Varanasi: Chaukhamba Surbharati Prakashana; 2005. Agnivesha, Charaka, Dridhabala, Charaka Samhita, Chikitsa Sthana, Pandurogachikitsa Adhyaya, 16/93-96. 530. [Google Scholar]
- 7.Shantharam KS, Gopinath BG, Mangalgi SG. Thesis. Mysore: Kayachikitsa Department, Gov Ayurvedic Medical College, RUGHS; 1986. Management of Pandu roga associated with Shotha, M.D. [Google Scholar]
- 8.Sengupta S, Panda N, Mahapatra SK. Thesis. Puri: Dept of Kayachikitsa, Gopalbandhu Ayurveda Mahavidhalaya; 1996. A clinical study on Pandu associated with Ankushmukhi krimi-Ankylostoma duodenale and its management by punarnavadi manduram, M.D. [Google Scholar]
- 9.Bombarde DT. Thesis. Bombay: Dept. of Kayachikitsa, R.A Podar Medical College (Ayu); 1987. Effect of Punarnavadi Mandura in Pandu Roga, M.D. [Google Scholar]
- 10.Vasundhara S, Tiwari PV. Thesis. Varanasi: Dept. of Prasuti – Balaroga, Faculty of Ayurveda, Institute of Medical Science, B.H.U; 1980. Treatment of garbhini pandu with punarnava mandoora. M. D. [Google Scholar]
- 11. Geneva, Switzerland: WHO; 1968. [Last accessed on 2011, 21 July]. World Health Organization. Nutritional Anaemias. Report of a WHO Scientific Group. Technical Report Series No. 405. Available from: http://www.whqlibdoc.who.int/trs/WHO_TRS_405.pdf . [PubMed] [Google Scholar]
- 12.Izaks GJ, Westendorp RG, Knook DL. The definition of anemia in older persons. JAMA. 1999;281:1714–7. doi: 10.1001/jama.281.18.1714. [DOI] [PubMed] [Google Scholar]
- 13.Acharya VJ, editor. Varanasi: Chaukhamba Surbharati Prakashana; 2005. Agnivesha, Charaka, Dridhabala, Charaka Samhita, Chikitsa, Sthana Pandurogachikitsa Adhyaya, 16/13-16; 2 nd ed; p. 527. [Google Scholar]
- 14.Ibidem, Charaka Samhita, Sutra Sthana, Kiyanta Shirshiya Adhyaya, 17/64-69. :103. [Google Scholar]
- 15.QOL questionnaire. [Last accessed on 2010 Dec. 20]. Available from: http://www.donaldepstein.com/pdf/newlongitudinal.pdf .
- 16.Vaidya Jadavji Tirkamji Acharya., editor. 2nd ed. Varanasi: Chaukhamba Surbharati Prakashana; 2005. Agnivesha, Charaka, Dridhabala, Charaka Samhita, Vimana Sthana, Rogabhishagjitiya Adhyaya, 8/89. 275. [Google Scholar]
- 17.Ying Yuan, Valen E. Johson, Bayesian Hypothesis tests using nonparametric statistics, Statistica Sinica, 18, 2008, 1185-1200 [Google Scholar]
- 18.Guralnik JM, Ershler WB, Schrier SL, Picozzi VJ. Anemia in the elderly: A public health crisis in hematology. Hematology American Society of Hematology Education Programmee. 2005. [Last accessed on 2011 Jul 02]. pp. 528–32. Available from: http://www.clinicalgeriatrics.com/articles/Anemia-Elderly . [DOI] [PubMed]
- 19.Mohan H. 5th ed. New Delhi: Published by Jaypee Brothers, Medical Publishers; 2005. Text Book of Pathology; p. 940. [Google Scholar]
- 20.Joosten E, pelemans W, Hiele M, Noyen J, Verghaeghe R, Boogaerts MA. Prevalence and causes of anaemia in a geriatric hospitalized population, Gerontol. 1992;38:111–7. doi: 10.1159/000213315. [DOI] [PubMed] [Google Scholar]
- 21.Vaidya Jadavji Trikamji Acharya., editor. 2nd ed. Varanasi: Chaukhamba Surbharati Prakashana; 2005. Agnivesha, Charaka, Dridhabala, Charaka Samhita, Vimana Sthana, Trividhakukshiya Vimana Adhyaya, 2/9. 238. [Google Scholar]
- 22.Sarkar PK, Prajapati PK, Chaudhary AK, Ravishankar B, De S. Thesis. Jamnagar: Rasa Shastra Department, IPGT and RA, Gujarat Ayurved University; 2005. A Comparative Pharmaceutico-Pharmaco-Clinical Study of Lauha Bhasma and Mandura Bhasma W.S.R to its Panduhara Effect. M. D; p. 255. [Google Scholar]
- 23.Sharma PC, Yelne MB, Dennis TJ. Vol. 1. Delhi: CCRAS, Dept of ISM and H, Ministry of H and FW, Government of India; 2002. Database on Medicinal Plants Used in Ayurveda; p. 104. Reprint. ed. [Google Scholar]
- 24.Sharma PC, Yelne MB, Dennis TJ. Vol. 3. Delhi: CCRAS, Dept of ISM and H, Ministry of H and FW, Government of India; 2005. Database on Medicinal Plants Used in Ayurveda; p. 473. Reprint ed. 480. [Google Scholar]
- 25.Vaidya Jadavji Trikamji Acharya., editor. 2nd ed. Varanasi: Chaukhamba Surbharati Prakashana; 2005. Agnivesha, Charaka, Dridhabala, Charaka Samhita, Chikitsa Sthana, Pandurogachikitsa Adhyaya, 16/10. 527. [Google Scholar]
- 26.Ibidem, Charaka Samhita, Vimana Sthana, Rogabhishagjitiya Adhyaya, 8/122. 280. [Google Scholar]
- 27.Mishra BS, editor. 7th ed. Varanasi: Chaukhambha Sanskrita Bhavan; 1990. Bhavamishra, Bhavaprakash Nighantu, Purvardha, Haritakyadi Varga, 1/42-32. 12. [Google Scholar]
- 28.Ibidem. Bhavprakasha Nighantu, Haritakyadi Varga, 1/63. 19. [Google Scholar]
- 29.Ibidem. Bhavprakasha Nighantu, Haritakyadi Varga, 1/70. 19. [Google Scholar]
- 30.Ibidem. Bhavprakasha Nighantu, Haritakyadi Varga, 1/12. 52. [Google Scholar]
- 31.Ibidem. Bhavprakasha Nighantu, Haritakyadi Varga, 1/64. 19. [Google Scholar]
- 32.Kohli KR, Nipanikar SU, Kadbhane KP. A comprehensive review on Trivrit [Operculina turpethum Syn. Ipomoea turpethum] Int J Pharma Bio Sci. 2010;1:443–52. [Google Scholar]
- 33.Malhotra S, Pal Singh A. A review of pharmacology of phytochemicals from Indian medicinal plants. Internet J Altern Med. 2007;5(1):4. [Google Scholar]
- 34.Joy PP, Thomas J, Samuel M, Skaria BP. Vol. 1. Thrissur: Kerala Agricultural University, Aromatic and Medicinal Plants Research Station; 1998. Medicinal Plants; p. 114. [Google Scholar]
- 35.Mishra B S, editor. 7th ed. Varanasi: Chaukhambha Sanskrita Bhavan; 1990. Bhavamishra, Bhavaprakash Nighantu, Purvardha, Haritakyadi Varga, 1/197. 114. [Google Scholar]
- 36.Ibidem. Bhavaprakasha, Haritakyadi Varga, 1/39. 10. [Google Scholar]
- 37.Ibidem. Bhavaprakasha, Haritakyadi Varga, 1/58. 15. [Google Scholar]
- 38.Ibidem. Bhavaprakasha, Guduchyadi Varga, 1/231. 422. [Google Scholar]
- 39.Kaiyadeva Nighantu. Aaushadhi Varga/1016. In: Sharma P, Sharma GP, editors. 1st ed. Varanasi: Chaukhmbha Orientalia; 2006. 188. [Google Scholar]
- 40.Sai Ram M, Neetu D, Yogesh B, Anju B, Dipti P, Pauline T, et al. Cyto-protective and immunomodulating properties of amla (Emblica officinalis) on lymphocytes: An in-vitro study. J Ethnopharmacol. 2002;81:5–10. doi: 10.1016/s0378-8741(01)00421-4. [DOI] [PubMed] [Google Scholar]
- 41.Patil KS, Jalalpure SS, Wadekar RR. Effect of Baliospermum montanum root extract on phagocytosis by human neutrophils. Indian J Pharm Sci. 2009;71:68–71. doi: 10.4103/0250-474X.51966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Sunila ES, Kuttan G. Immunomodulatory and antitumor activity of Piper longum Linn. and piperine, J Ethnopharmacol. 2004;90:339–46. doi: 10.1016/j.jep.2003.10.016. [DOI] [PubMed] [Google Scholar]
- 43.Sumanth M, Mustafa SS. Antistress, adoptogenic and immunopotentiating activity roots of Boerhaavia diffusa in mice. Int J Pharmacol. 2007;3:416–20. [Google Scholar]
- 44.Kulakarni S, Desai S. Immunostimulant activity of inulin from Saussurea lappa roots. Indian J Pharm Sci. 2001;63:292–4. [Google Scholar]
- 45.Singh J, Kakkar P. Antihyperglycemic and antioxidant effect of Berberis aristata root extract and its role in regulating carbohydrate metabolism in diabetic rats. J Ethnopharmacol. 2009;123:22–6. doi: 10.1016/j.jep.2009.02.038. [DOI] [PubMed] [Google Scholar]
- 46.Bhattacharya A, Chatterjee A, Ghosal S. Antioxidant activity of active tannoid principles of Emblica officinalis (Amla) Indian J. Exp. Biol. 1999;37(7):676–80. [PubMed] [Google Scholar]
- 47.Mohan H. 5th ed. New Delhi: Jaypee Brothers, Medical Publishers; 2005. Text Book of Pathology; p. 369. [Google Scholar]
- 48.Khajuria A, Zutshi U, Bedi KL. Permeability characteristics of piperine on oral absorption – An active alkaloid from peppers and a bioavailability enhancer. Indian J Exp Biol. 1998;36:46–50. [PubMed] [Google Scholar]
- 49.Shoba G, Joy D, Joseph T, Majeed M, Rajendran R, Srinivas PS. Influence of piperine on the pharmacokinetics of curcumin in animals and human volunteers. Planta Med. 1998;64:353–6. doi: 10.1055/s-2006-957450. [DOI] [PubMed] [Google Scholar]
- 50.Agarwal AK, Singh M, Gupta N, Saxena R, Puri A, Verma AK, et al. Management of giardiasis by an immuno-modulatory herbal drug Pippali rasayana. J Ethnopharmacology. 1994;44:143–46. doi: 10.1016/0378-8741(94)01181-8. [DOI] [PubMed] [Google Scholar]
- 51.Baghel MS, Prajapati PK, Ravishankar B, Patgiri BJ, Shukla VJ. Jamnagar: India, Institute for Post Graduate Teaching and Research in Ayurveda, Gujarat Ayurved University; 2009. Galib, Monograph on Punarnava Mandura (SMP and Safety Profile) p. 7. [Google Scholar]
- 52.Banga RK, Singhal LK, Chauhan RS. Cow urine and immunomodulation: An update on cowpathy. Int J Cow Sci. 2005;1(2):26–9. [Google Scholar]
- 53. [Last accessed on 2011 Jul 02]. Available from: http://www.goshala.com/Articles/2011/Jun/Urinebenefits.html .
- 54.Kaviraj Ambikadatta Shastri., editor. Varanasi: Chaukhambha Sanskrit Sansthan; 2005. Sushruta, Sushruta Samhita, Sutrasthana, Dravadravya Vidhi Adhyaya, 45/54. reprint ed. 176. [Google Scholar]