

Abstract
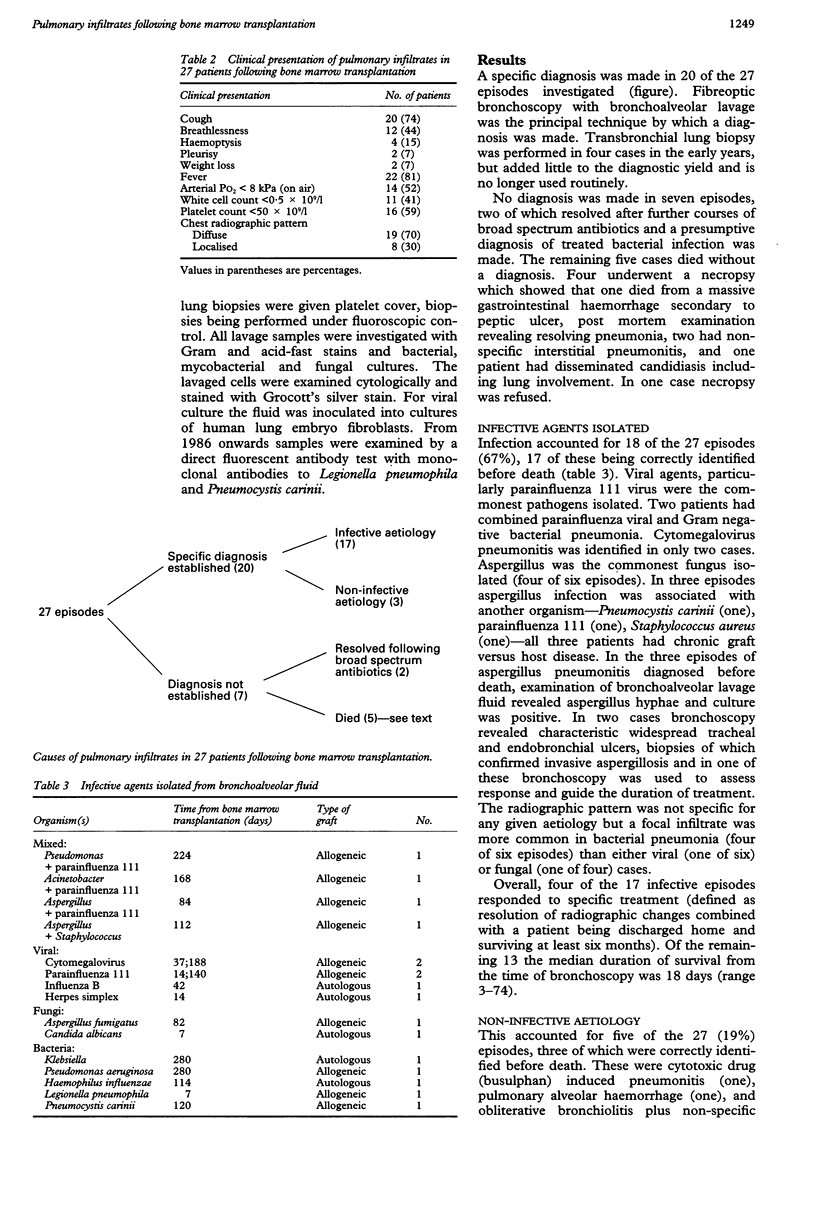
BACKGROUND--Although pulmonary infiltrates are common in bone marrow transplant recipients and add significantly to the morbidity and mortality of this group of patients, there is uncertainty as to the most appropriate investigation and a lack of information on the effects of investigations on management and outcome. METHODS--All bone marrow transplant recipients from one institution referred for respiratory investigation between 1982 and 1990 were reviewed. RESULTS--Of 204 bone marrow transplant recipients 27 developed pulmonary infiltrates which failed to respond to broad spectrum antibiotics. All were examined by bronchoscopy and bronchoalveolar lavage. A specific diagnosis was made in 20 cases, 17 with an infective cause and three with a non-infective aetiology. In 17 of the 27 episodes these investigations led to a positive change in treatment, but in only five did these changes result in patient survival beyond one month. Eighteen of the 20 deaths were due to progressive respiratory failure of an infective aetiology in 14 and non-infective in four. CONCLUSIONS--Bronchoscopy and bronchoalveolar lavage are effective in establishing a diagnosis, but the impact on overall survival is disappointingly poor.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Campbell J. H., Raina V., Banham S. W., Cunningham D., Soukop M. Pulmonary infiltrates--diagnostic problems in lymphoma. Postgrad Med J. 1989 Dec;65(770):881–884. doi: 10.1136/pgmj.65.770.881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark J. G., Crawford S. W. Diagnostic approaches to pulmonary complications of marrow transplantation. Chest. 1987 Apr;91(4):477–479. doi: 10.1378/chest.91.4.477. [DOI] [PubMed] [Google Scholar]
- Krowka M. J., Rosenow E. C., 3rd, Hoagland H. C. Pulmonary complications of bone marrow transplantation. Chest. 1985 Feb;87(2):237–246. doi: 10.1378/chest.87.2.237. [DOI] [PubMed] [Google Scholar]
- Lum L. G. The kinetics of immune reconstitution after human marrow transplantation. Blood. 1987 Feb;69(2):369–380. [PubMed] [Google Scholar]
- Meyers J. D., Flournoy N., Thomas E. D. Nonbacterial pneumonia after allogeneic marrow transplantation: a review of ten years' experience. Rev Infect Dis. 1982 Nov-Dec;4(6):1119–1132. doi: 10.1093/clinids/4.6.1119. [DOI] [PubMed] [Google Scholar]
- Milburn H. J., Prentice H. G., du Bois R. M. Role of bronchoalveolar lavage in the evaluation of interstitial pneumonitis in recipients of bone marrow transplants. Thorax. 1987 Oct;42(10):766–772. doi: 10.1136/thx.42.10.766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neiman P. E., Reeves W., Ray G., Flournoy N., Lerner K. G., Sale G. E., Thomas E. D. A prospective analysis interstitial pneumonia and opportunistic viral infection among recipients of allogeneic bone marrow grafts. J Infect Dis. 1977 Dec;136(6):754–767. doi: 10.1093/infdis/136.6.754. [DOI] [PubMed] [Google Scholar]
- Robin E. D., Burke C. M. Lung biopsy in immunosuppressed patients. Chest. 1986 Feb;89(2):276–278. doi: 10.1378/chest.89.2.276. [DOI] [PubMed] [Google Scholar]
- Weiner R. S., Bortin M. M., Gale R. P., Gluckman E., Kay H. E., Kolb H. J., Hartz A. J., Rimm A. A. Interstitial pneumonitis after bone marrow transplantation. Assessment of risk factors. Ann Intern Med. 1986 Feb;104(2):168–175. doi: 10.7326/0003-4819-104-2-168. [DOI] [PubMed] [Google Scholar]
- Wingard J. R., Mellits E. D., Sostrin M. B., Chen D. Y., Burns W. H., Santos G. W., Vriesendorp H. M., Beschorner W. E., Saral R. Interstitial pneumonitis after allogeneic bone marrow transplantation. Nine-year experience at a single institution. Medicine (Baltimore) 1988 May;67(3):175–186. doi: 10.1097/00005792-198805000-00004. [DOI] [PubMed] [Google Scholar]
- Winston D. J., Gale R. P., Meyer D. V., Young L. S. Infectious complications of human bone marrow transplantation. Medicine (Baltimore) 1979 Jan;58(1):1–31. doi: 10.1097/00005792-197901000-00001. [DOI] [PubMed] [Google Scholar]