

Abstract
Background:
Educated women are known to take informed reproductive and healthcare decisions. These result in population stabilization and better infant care reflected by lower birth rates and infant mortality rates (IMRs), respectively.
Materials and Methods:
Our objective was to study the relationship of male and female literacy rates with crude birth rates (CBRs) and IMRs of the states and union territories (UTs) of India. The data were analyzed using linear regression. CBR and IMR were taken as the dependent variables; while the overall literacy rates, male, and female literacy rates were the independent variables.
Results:
CBRs were inversely related to literacy rates (slope parameter = −0.402, P < 0.001). On multiple linear regression with male and female literacy rates, a significant inverse relationship emerged between female literacy rate and CBR (slope = −0.363, P < 0.001), while male literacy rate was not significantly related to CBR (P = 0.674). IMR of the states were also inversely related to their literacy rates (slope = −1.254, P < 0.001). Multiple linear regression revealed a significant inverse relationship between IMR and female literacy (slope = −0.816, P = 0.031), whereas male literacy rate was not significantly related (P = 0.630).
Conclusion:
Female literacy is relatively highly important for both population stabilization and better infant health.
Keywords: Birth rate, education, female literacy, India, infant mortality, population growth
Introduction
Social determinants of health such as education and gender equality are strongly related to health seeking behavior and overall health outcomes. It has been known that better education, partly reflected by higher literacy rates is associated with higher incomes and better health indicators such as lower infant mortality rates (IMRs) and lower population growth rate. Education of families, especially of women has a ‘multiplier effect’ on development.[1] Reduction of fertility has been observed in relation to better educational attainment in women.[2,3] Education of women reflected as higher literacy has also been seen to reduce IMRs independent of socioeconomic status or residence in rural or urban area.[4,5,6,7]
Both population stabilization and reduction in infant mortality are key priorities for India, for which better literacy is needed. However, the general relationship between literacy and improved health tends to obscure the specific contribution of female literacy over and above male literacy. Millennium Development Goals have emphasized gender equality with the target of eliminating gender disparity in education of boys and girls.[8] Therefore, we aim to estimate the individual independent associations of male and female literacy with certain key health indicators, that is, crude birth rate (CBR) and IMR of states and union territories (UTs) in India. Knowledge of these individual associations will help us understand how the gender inequality in literacy specifically influences these health indicators.
Materials and Methods
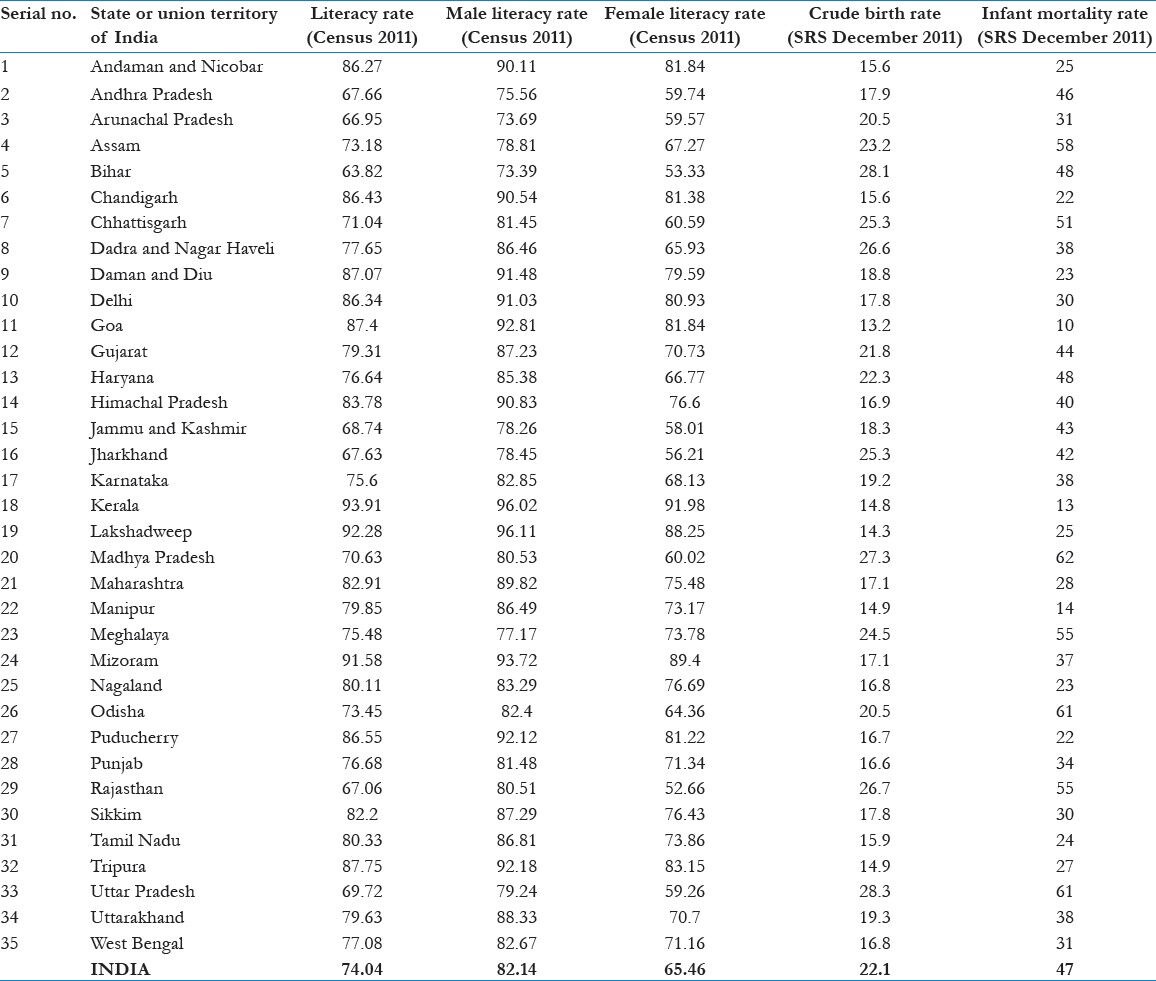
We did an ecological analysis of the data from the national surveys conducted by the Registrar General of India. State-wise literacy rates were taken from the 2011 Census of India.[9] We used literacy rates to reflect educational status to give a simple percentage measure for uniform comparison. CBR and IMR were taken from Sample Registration System (SRS) report pertaining to December 2011.[10] Thus, the census and SRS data corresponded to roughly the same time period. CBR was taken as a surrogate fertility indicator as other indicators such as generalized fertility rates, generalized marital fertility rates, and total fertility rates were available only for large states with more than 10 million population. Each state or UT was taken as the unit for linear regression analysis. CBR and IMR were taken as dependent variables while the overall, male, and female literacy rates were independent variables. The dataset used is given in Table 1.
Table 1.
Literacy rates, crude birth rates, and infant mortality rates of states and union territories of India (Census 2011 and Sample Registration System (SRS) December 2011)
Best fitting lines on scatter plots were drawn and slope parameters and R2 value was calculated. Initially, overall literacy rates and male literacy rates and female literacy rates were all analyzed individually with CBR and IMR, respectively. Next, we combined male and female literacy rates as predictors of CBR and IMR, respectively in multiple regression analysis. We used the slopes of the regression line to quantify the expected reductions in CBR and IMR on each 10% increase in overall literacy rates of states and UTs.
Results
On linear regression, an inverse relationship was found between male literacy rates, female literacy rates [Figure 1], and overall literacy rates with that of the CBR of the respective states and UTs [Table 2]. The slope of -0.325 for female literacy versus CBR suggests that every 1% increase in female literacy is associated with fall in CBR by 0.325/1,000 live births. Fifty-nine percent of the variability in CBR was explained by this relationship, as suggested by the R2 value.
Figure 1.
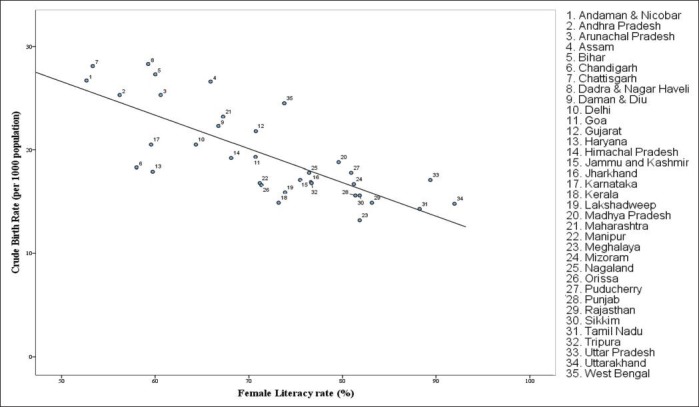
Scatter plot and linear regression of female literacy rates vs crude birth rates of states and union territories (UTs) of India (slope = – 0.325, P < 0.001, R2 = 0.590)
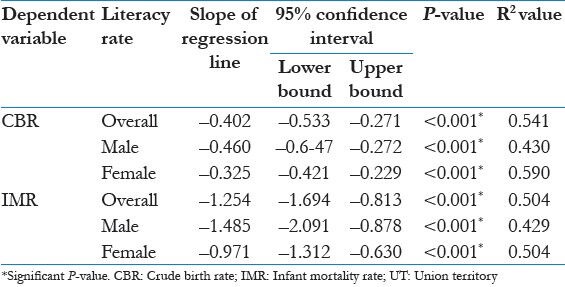
Table 2.
Results of individual linear regression between literacy rates as a predictor of CBR and IMR of states and UTs of India
Similarly, an inverse relationship was found between male literacy rates, female literacy rates [Figure 2], and overall literacy rate literacy rates taken individually with the IMR of the states and the UTs [Table 2].
Figure 2.
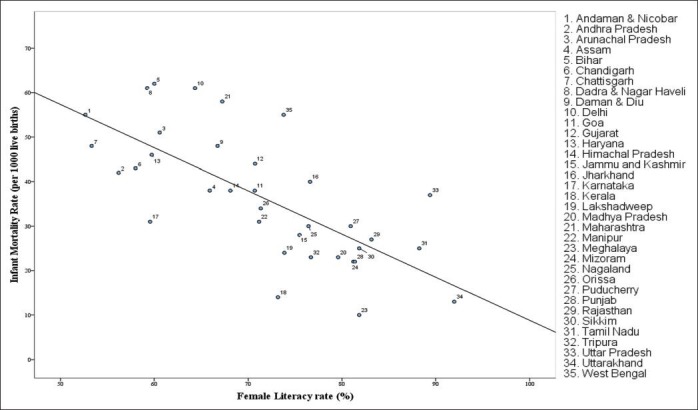
Scatter plot and linear regression of female literacy rates vs infant mortality rates of states and UTs of India (slope = – 0.971, P < 0.001, R2 = 0.504)
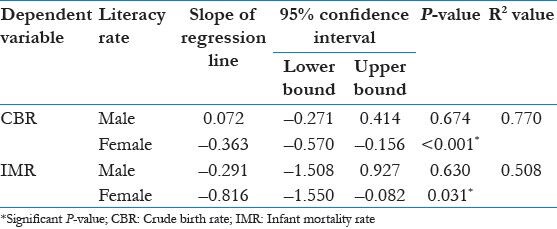
We did multiple linear regression taking male and female literacy rates together as predicting factors of CBR. We found that there was no relationship between male literacy rate and CBR, as the slope of linear regression line was found not significantly different from zero. The slope of female literacy remained significantly negative, implying an inverse relationship [Table 3]. Similarly, while taking male and female literacy rates together as predicting factors of IMR, the relationship of male literacy rate with IMR was found to be nonsignificant, while an inverse relationship was found between female literacy rate and IMR, as suggested by a significantly negative slope [Table 3].
Table 3.
Multiple linear regression between male and female literacy rates together as a predictor of CBR and IMR, respectively
Discussion
States and UTs with higher literacy rates were found to have lower birth rates and IMRs. An association at the state or UT level was found between high female literacy rates and low birth rates and low IMRs. This suggests that literacy in women is related to delayed age of marriage and better access to contraception, thereby contributing to population stabilization.[11,12] The slope of linear regression suggests that a 10% increase in overall literacy rate at the state or UT level will reduce CBR by four live births/1,000 population and IMR by 12/1,000 live births. This potential reduction of IMR with improvement in literacy is substantial. For example in a state with an IMR of 60/ 1,000 live births, a 20% reduction in IMR may be expected with a 10% rise in literacy rate. However, we do not quantify probable improvements in these indicators due to improvement in female and male literacy rates separately, as it is not possible to improve one without the other.
We also found that female literacy rates were inversely related to IMR and CBR independent of the male literacy rates. Although statistically associative in nature, many causal pathways for this relationship may exist. First of all, education brings independent income for women who can spend it on essential child care. Better social standing of women resulting from wider literacy is likely to give them decision making roles with regard to nutrition and immunization, thereby improving child health. Also, education empowers women to apply the right knowledge in the form of home based care and prompt referral of a child in an illness.[13] This, in addition to the gains made over time in ensuring adequate nutrition, is one of the plausible mechanisms of women's education saving infant lives.
Overall, it is highlighted that literacy of women is relatively more important for both population stabilization and lower infant mortality than male literacy rates. Our findings suggest that gender equality in literacy must be considered important. In settings where there is a high gap in male and female literacy, health indicators are expected to remain poor despite high overall literacy rates. This phenomenon is seen in some states like Chhattisgarh, Madhya Pradesh, Haryana, and Orissa.[9]
We have a limitation that this ecological association might not be generalizable to the family unit. But we feel that even this broad relationship should spur the individual state governments of India to prioritize education of girls as a highly productive strategy for improving health.
The latest report on Millennium Development Goals states that one of the targets of achieving gender parity in school enrolment of girls and boys has been achieved.[14] It remains to be seen how far this encouraging trend is replicated in the social and economic arena of gender parity. In the years to come, we must not lose sight of the fact that empowerment of women is vital to the achievement of a healthy community.
Conclusion
Female literacy is an important determinant of infant health and population stabilization. The effect of female literacy exists independently of male literacy.
Footnotes
Source of Support: None
Conflict of Interest: None declared
References
- 1.New York: United Nations; 2012. [Last accessed on 2012 Dec 1]. UN Economic and Social Council. Commission on the Status of Women: Fifty-fifth Session. Available from: http://www.un.org/News/Press/docs//2011/wom1843.doc.htm . [Google Scholar]
- 2.Graff M, Yount KM, Ramakrishnan U, Martorell R, Stein AD. Childhood nutrition and later fertility: Pathways through education and pre-pregnant nutritional status. Demography. 2010;47:125–44. doi: 10.1353/dem.0.0090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kravdal Ø. Education and fertility in sub-Saharan Africa: Individual and community effects. Demography. 2002;39:233–50. doi: 10.1353/dem.2002.0017. [DOI] [PubMed] [Google Scholar]
- 4.Ramakrishnan U, Barnhart H, Schroeder DG, Stein AD, Martorell R. Early childhood nutrition, education and fertility milestones in Guatemala. J Nutr. 1999;129:2196–202. doi: 10.1093/jn/129.12.2196. [DOI] [PubMed] [Google Scholar]
- 5.Peña R, Liljestrand J, Zelaya E, Persson LA. Fertility and infant mortality trends in Nicaragua 1964-1993. The role of women's education. J Epidemiol Community Health. 1999;53:132–7. doi: 10.1136/jech.53.3.132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rao RS, Chakladar BK, Nair NS, Kutty PR, Acharya D, Bhat V, et al. Influence of parental literacy and socio-economic status on infant mortality. Indian J Pediatr. 1996;63:795–800. doi: 10.1007/BF02730932. [DOI] [PubMed] [Google Scholar]
- 7.Gokhale MK, Rao SS, Garole VR. Infant mortality in India: Use of maternal and child health services in relation to literacy status. J Health Popul Nutr. 2002;20:138–47. [PubMed] [Google Scholar]
- 8.New York: United Nations; 2000. United Nations General Assembly. United Nations Millennium Declaration. [Google Scholar]
- 9.New Delhi: 2011. [Last accessed on 2012 Dec 1]. Registrar General of India. Statement 5, Provisional Population Totals Paper 2. Census of India, 2011. Available from: http://www.censusindia.gov.in/2011-prov-results/paper2/prov_results_paper2_india.html . [Google Scholar]
- 10.New Delhi: 2012. [Last accessed on 2012 Dec 1]. Registrar General of India. SRS Bulletin Volume 46 No 1. Sample Registration System. Available from: http://censusindia.gov.in/vital_statistics/SRS_Bulletins/Bulletins.aspx . [Google Scholar]
- 11.Panopoulou G, Tsakloglou P. Fertility and economic development: Theoretical considerations and cross-country evidence. Appl Econ. 1999;31:1337–51. doi: 10.1080/000368499323229. [DOI] [PubMed] [Google Scholar]
- 12.Maitra P. Effect of socioeconomic characteristics on age at marriage and total fertility in Nepal. J Health Popul Nutr. 2004;22:84–96. [PubMed] [Google Scholar]
- 13.Shieh C, Halstead JA. Understanding the impact of health literacy on women's health. J Obstet Gynecol Neonatal Nurs. 2009;38:601–10. doi: 10.1111/j.1552-6909.2009.01059.x. [DOI] [PubMed] [Google Scholar]
- 14.New York: United Nations; 2012. United Nations. The millennium development goals report 2012. [Google Scholar]