

Abstract
Context:
Anaemia is a major public health problem in India. Many studies have emphasized on prevalence of anaemia among general population. This study has focussed to address the prevalence of anaemia among the tribal population in Udupi taluk. Anaemia among women in the reproductive age group is one of the causes for maternal morbidity and mortality in India.
Aim:
To estimate the prevalence of anemia among tribal women (aged 15 to 49 years).
Settings and Design:
A Community based cross sectional study was conducted among tribal women aged 14-49 years in Udupi taluk, Udupi district, Karnataka.
Methods and Material:
A cross sectional study during July 2012 to August 2012 was conducted. A sample size of 170 was calculated taking into consideration a relative error of 15% and the prevalence of anemia in Karnataka as 51% (as per the NFHS-3).
Statistical analysis used:
Univariate and multivariate analysis was used to analyse the data using SPSS 15.
Results:
The study sample had a mean hemoglobin value of 11.3 g/dL with 95% CI of (11 – 11.6), with a standard deviation of 2g/dL. The study reveals that in the sample of tribal women in the age group of 15-49 years, the prevalence of anemia was 55.9%. Among the subjects, 6 (3.5%) were severely anemic, 33 (19.4%) were moderately anemic and 56 (32.9%) were mildly anemic.
Conclusions:
This study calls for an appropriate action and intervention in this tribal population to treat and prevent anaemia.
Keywords: Anaemia, Karnataka, population, tribal
Introduction
Anemia is a condition in which the hemoglobin level is below normal and insufficient to meet physiologic needs.[1] The World Health Organization (WHO) estimates anemia as a major public health problem with almost 2 billion people having anemia below normal values.[2] One of the most common causes of anemia is due to inadequate supply of nutrients.[3]
Poor eating habits play a major role in the development of iron deficiency anemia that is an important indicator of poor health status.[3] Children and adolescent are at increased risk of developing iron deficiency anemia because of their increased demand for iron during growth and puberty.[4]
India continues to be one of the countries with very high prevalence. National Family Health Survey (NFHS-3) reveals the prevalence of any anemia to be 55.3%.[5] The NFHS-3 also estimates the prevalence of any type of anemia in Karnataka to be 51.5%, putting half of the population at risk of acquiring anemia.[5]
There are 50 major tribes with 109 subtribes in Karnataka state (as of March 2005), according to the notified schedule under Article 342 of the Constitution of India.[6] Among these tribes, Koraga and Marati Naik tribes dwell in the tribal locales of Udupi Taluk, Udupi district. Previous studies conducted by Jai Prabhakar and Gangadhar[7] in 2009, reports prevalence of anemia in children of Jenukuruba tribe of Karnataka to be 77.1%. De et al.,[8] in 2006 reported incidence of anemia among the tribal people of Assam as 59.82%, in Arunachal Pradesh 53.77% and Tripura 57.45%. The objective of the study is to estimate the prevalence of anemia among tribal women (aged 15-49 years).
Subjects and Methods
The study was a community-based epidemiological survey, employing cross-sectional study design. The study was conducted in association with the Mobile Tribal Health Unit of Peradoor area, located in Udupi Taluk.
The study was conducted among identified Koraga and Marathi Naik tribal hamlets of Udupi Taluk. From the identified tribal blocks, 17 hamlets were visited during this survey. House to house visits were conducted to ensure active participation of the target group. All women aged 15-49 years who belonged to any of the tribal groups and a permanent resident of the selected study setting, who were willing to give their informed consent for the study, were asked to participate in the survey. Considering relative error of 15% and prevalence of anemia in Karnataka (NFHS-3)[5] of 0.51, the sample size was calculated to be 170
Tools
The primary data collection tool was an interview schedule. The schedule had five sections with questions pertaining to the following domains of demographic details, diet history, menstrual history, marital and reproductive history, and general health history. Hemoglobin estimation was done using HemoCue® 201+ hemoglobin photometer; Angelholm, Sweden. The HemoCue® system consists of a portable photometer and a one-step blood collection device (microcuvette) that is covered with dry hemoglobin conversion reagents. The system does not use wet reagents and it allows for measuring hemoglobin levels within a minute. HemoCue® system is accepted as a standard method for hemoglobin measurement by the International Committee for Standardization in Hematology.[9] Sari et al.,[10] recommends the HemoCue method to be used for surveys which are conducted in relatively remote areas. A Medina Lara et al.,[11] concluded recommending HemoCue as the optimal method based on most of the outcome measures. The cost of a single test (US$0.75/test) may be expensive compared with other tests.
Results
The prevalence of anemia was 55.9% (95) with hemoglobin values below 12 g/dL. Among the subjects, 6 (3.5%) were severely anemic, 33 (19.4%) were moderately anemic, and 56 (32.9%) were mildly anemic. The study sample had a mean hemoglobin value of 11.3 g/dL with 95% confidence interval (CI) of (11-11.6), with a standard deviation of 2 g/dL. The demographic details are mentioned in Table 1.
Table 1.
Demographic characteristics N=170
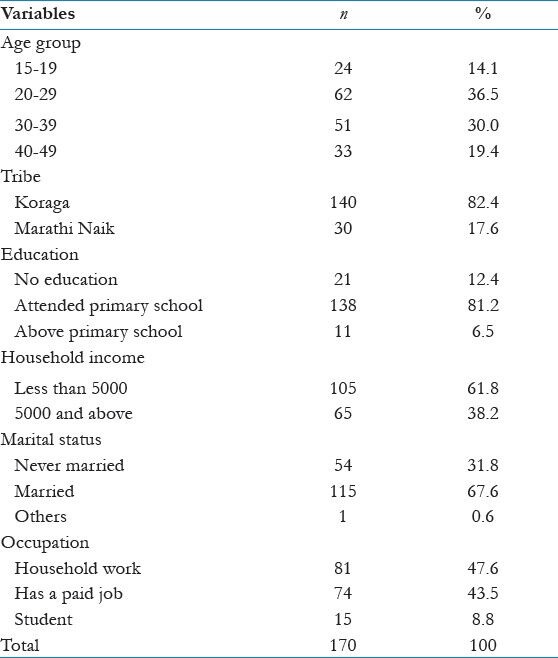
All the participants, 170 (100%), followed a mixed diet pattern. Rice was the staple food in the study, and all of them had consumed at least three servings in the last week before the interview. Majority of the subjects 156 (91.8%) had consumed at least one serving of green leafy vegetables, 144 (84.7%) had consumed at least one serving of fruits along with the meals.
The participants of the study had a mean age at menarche of 13.69 [standard deviation (SD = 6.7)], whereas 100 (58.8%) recall that they had attained menarche at 13 years of age or before, while the rest had attained menarche after 13 years of age. A majority 94 (81%) got married after the age of 18 years. Among the participants, 7 (6%) were pregnant and 14 (12.1) were lactating mothers. Among lactating mothers, eight were found to be anemic.
The mean age of mothers at their first birth was19.9 years (SD = 3.9). A majority of mothers 37 (50.7%) gave their second birth after an interval of 3 or more years. A majority of the mothers 85 (78.7%) said that they had not taken Iron folic acid tablets during their last pregnancy. Food intake during the last pregnancy was same as the nonpregnant state for 45 (26.5%), while 43 (25.3%) said that they consumed more. Out of the subjects who successfully completed a pregnancy, 78 (69.6%) had gone for at least three antenatal visits during the last pregnancy, while 26 (23.2%) had gone for six or more antenatal visits.
In the study, 86 (50.6%) of having ever consumed iron tablets or syrup, but all of them stopped after their pregnancies. Only 19 (11.2%) were currently consuming iron tablets/syrup. The iron tablets/syrup was sourced by 80 (47.1%) from hospital/Primary Health Centre. All of the participants said that they neither had reason to suspect worm infestations, nor did they have any history of malaria in last 3 months.
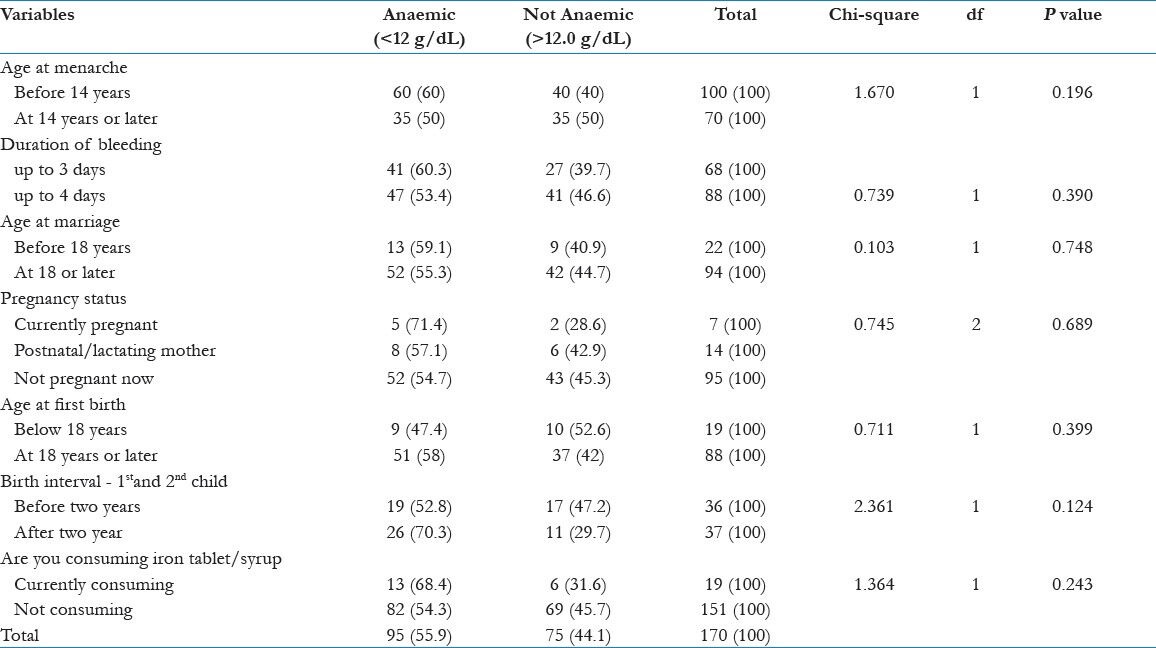
Table 2 shows univariate analysis was using chi-square test to compare proportions. The sample did not show significant difference between anemic and nonanemic groups when analyzed with these variables, except for the occupation of the individual.
Table 2.
Univariate analysis
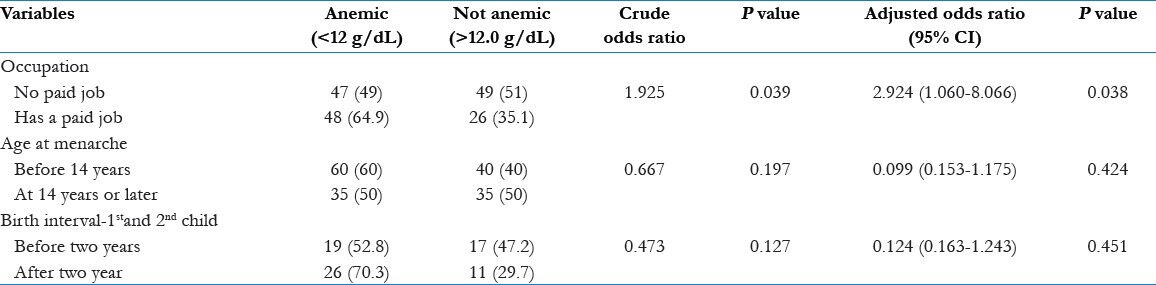
Only occupation of the individual showed any significant differences in the anemic and nonanemic groups. In Table 3, multivariate logistic regression showed statistically significant difference for the occupation of the individual. The participants who did not have a paid job were at higher odds of being anemic [odds ratio of 2.924 (95% CI: 1.060–8.066), P value = 0.038].
Table 3.
Multivariate analysis
Discussion
This study confirms that anemia is widely prevalent among tribal women of reproductive age group (15-49 years). This is similar to what has been reported for elsewhere in India and other developing countries across different populations. These figures for anemia are in close agreement with those reported for women of same age group (55%) in the NFHS-3, reported in 2005-2006.[5] It is also comparable to the prevalence rates reported in the state of Karnataka (51.5%) in the same NFHS survey.[5] De et al.,[8] in 2006 had conducted a study in the tribal regions of Northeast India. The prevalence of anemia among the tribal people of Assam was 59.82%, in Arunachal Pradesh 53.77% and Tripura 57.45%.[8] These findings are comparable to the finding of this study.
A study conducted in 2011 by Joshi[12] had found 95.3% prevalence of anemia in a group of tribal women. Even the study conducted by Jai Prabhakar and Gangadhar,[7] in 2009 showed a prevalence of 77.1% among the study sample. Balgir et al.,[13] had assessed the prevalence of anaemia in Bhuyan and Kharia tribes of Odisha state. Anemia was prevalent among both the tribes; Bhuyan tribe (89.9%) than in Kharia tribe (73.8%).[13] The WHO suggests that if the prevalence of anemia in a population is detected to be 40% or higher, it is considered to be severely anemic.[14] This study provides evidence that the prevalence of anemia among women in reproductive age group of the study population is 55.9%, which is much higher than the WHO criterion for severe anemia; thereby placing the tribal population of Udupi Taluk in the category of severely anemic.
The study was conducted among a population among whom a similar survey was never done. The data from this survey provide baseline information of the tribal women of reproductive age group. The information could be used by policy makers and health administrators in implementing new strategies and strengthening existing services.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Almaz S. Calverton, Maryland USA: ORC Macro; 2000. Anemia testing in population-based surveys: General information and guidelines for country monitors and program managers. [Google Scholar]
- 2.WHO Publications; 2005. Assessing Iron Status of Populations. Report of a Joint World Health Organization/Centers for Disease Control and Prevention Technical Consultation on the Assessment of Iron Status at the Population Level. [Google Scholar]
- 3.Agarwal KN, Agarwal DK, Sharma A, Sharma K, Prasad K, Kalita MC, et al. Prevalence of anemia in pregnant and lactating women in India. Indian J Med Res. 2006;124:173–84. [PubMed] [Google Scholar]
- 4.Park K. 20th ed. Jabalpur: Banarsidas Bhanot; 2009. A text book of Preventive and Social Medicine. [Google Scholar]
- 5.International Institute for Population Sciences (IIPS), NFHS 3 report- Chapter Nutrition and Anemia. 2006 [Google Scholar]
- 6.Indigenous Peoples Development Planning Document; 2006. Karnataka Urban Infrastructure Development and Finance Corporation (KUIDFC) [Google Scholar]
- 7.Jai Prabhakar SC, Gangadhar MR. Prevalence of anemia in jenukuruba primitive tribal children of Mysore District, Karnataka. Anthropologist. 2009;11:49–51. [Google Scholar]
- 8.De M, Halder A, Podder S, Sen R, Chakrabarty S, Sengupta B, et al. Anemia and hemoglobinopathies in tribal population of Eastern and North-eastern India. Hematology. 2006;11:371–3. doi: 10.1080/10245330600840180. [DOI] [PubMed] [Google Scholar]
- 9.Maryland: Hemocue Malaria Indicator Survey Anemia Testing Manual; 2005. Feb, ORC Macro. [Google Scholar]
- 10.Sari M, de Pee S, Martini E, Herman S, Sugiatmi, Bloem MW, et al. Estimating the prevalence of anemia: A comparison of three methods. Bull World Health Organ. 2001;79:506–11. [PMC free article] [PubMed] [Google Scholar]
- 11.Medina Lara A, Mundy C, Kandulu J, Chisuwo L, Bates I. Evaluation and costs of different hemoglobin methods for use in district hospitals in Malawi. J Clin Pathol. 2005;58:56–60. doi: 10.1136/jcp.2004.018366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Joshi A. Community based screening and management of adolescent anemia in tribal areas of India key to reduction in maternal mortality. J Adoles Health. 2011;48(2) Supplement 1:S23. [Google Scholar]
- 13.Balgir RS, Mishra RK, Murmu B. Clinical and hematological profile of hemoglobinopathies in two tribal communities of Sundargarh District in Orissa, India. Int J Hum Genet. 2003;3:209–16. [Google Scholar]
- 14.Geneva: World Health Organization; 2011. WHO. Hemoglobin concentrations for the diagnosis of anemia and assessment of severity. Vitamin and Mineral Nutrition Information System. [Google Scholar]