

Abstract
Background:
This study aimed to determine the relationship between the environmental factor, clinical risk factors, and individual variables with mortality due to acute myocardial infarction (MI) in Isfahan.
Materials and Methods:
This cross-sectional study was performed between April 2012 and March 2013. The data on the patients’ mortality due to MI in Isfahan were obtained from the MI National Registry. The international classification system (ICD10: I21-I22) was used to diagnose MI. The air quality indicators and environmental variables were used to measure the air pollution. Multilevel logistic regression in the Stata software was used to determine the factors associated with mortality in patients and odds ratios (ORs) were calculated.
Results:
Six hundred eleven patients with MI were studied during 1-year. 444 (72.2%) patients were male and the rest were female. 4.7% of the patients died due to MI. The mean age at MI incidence was 62.2 ± 13 years. Of the air pollution parameters, PM10 had the maximum mean concentration (49.113 ppm), followed by NOX, NO, NO2, CO, SO2, and O3. The adjusted OR of mortality was derived 2.07 (95% CI: 1.5-2.85) for right bundle branch block, 1.5 (95% CI: 1.3-1.7) for ST-segment elevation MI, 1.84 (95% CI: 1.13-3) for age, 1.06 (95% CI: 1.01-1.20) for CO, 1.1 (95% CI: 1.03-1.30) for O3, and 1.04 (95% CI: 1.01-1.4) for SO2, all of which were considered as the risk factors of mortality. However, OR of mortality was 0.79 for precipitation (95% CI: 0.74-0.84) and 0.52 for angioplasty (95% CI: 0.4-0.68) were considered as protective factors of mortality. The individual characteristics including age, history of MI in the immediate family, hypertension, and diabetes were significantly associated with mortality from MI. The indices of air pollution including SO2, CO, O3, and environmental factors such as the precipitation and temperature were the determinants of mortality in patients with MI.
Conclusion:
With regards to the factors associated with mortality from MI reported in this study, air pollution and environmental factors, in addition to the risk factors and predictive factors, should be particularly addressed to control the mortality from MI.
Keywords: Acute myocardial infarction, air pollution, mortality
INTRODUCTION
Myocardial infarction (MI) is the leading cause of death in Iran and worldwide.[1,2] The factors effective on the outcome of MI and its risk factors have been studied frequently in Iran and other countries. The most important risk factors of MI include age, gender, education, diabetes, hypertension, smoking, obesity, dyslipidemia, physical inactivity, and poor diet.[3,4] The relationship between the air pollution, temperature, relative humidity, precipitation, altitude, and mortality due to the diseases such as respiratory and cardiovascular have been identified and reported in industrialized countries.[5,6,7,8,9,10,11]
There is a significant relationship between the air pollution and human health, rates of hospital admissions and mortality.[12,13,14,15] Air pollution has the serious side effects in some populations such as the elderly, children, the patients with cardiovascular disease, and pregnant women.[16,17] The negative effects of air pollutants on pregnancy interval and miscarriage have been reported in Isfahan, Iran, as well.[18] According to some studies, there is a significant relationship between the air pollutants and MI, while other studies have reported no association.[16,19]
The relationship between the nontraditional risk factors such as air pollution, clinical, and individual risk factors and mortality due to MI in Isfahan as the largest metropolitan area in central Iran has not been yet established clearly. Thus, the necessity of this research relates to the need to provide evidence on the relationship between the air pollution and meteorological parameters, and MI and associated mortality in this metropolitan area.
This study aimed to determine the odds ratio (OR) for mortalities associated with air pollution indicators and environmental factors and to identify the model of mortality risk factors in patients with MI in Isfahan.
MATERIAL AND METHODS
This research is a descriptive-analytical study performed between April 2012 and March 2013. Individual data related to mortality in the patients with MI in Isfahan were gathered from the MI National Registry. The study was approved by the Center for Noncommunicable Diseases Control and Department of Cardiovascular Diseases Prevention, Iran Ministry of Health and Medical Education (Approval no: 305/837) and has been obtained from a PhD thesis of Epidemiology by the corresponding author at Shahid Beheshti University of Medical Sciences (Grant no: 1392-1-85-12129). The international classification system (ICD10: I21-I22) was used to diagnose the MI. Individual data of the patients admitted to Isfahan hospitals were collected and recorded on a daily basis. The patients were followed up until they died from a MI or were discharged from the hospital. Definitive diagnosis of acute MI was done by a cardiologist and according to the World Health Organization criteria.[19] Other demographic variables such as age, gender, education, and risk factor variables such as history of diabetes, hypertension, smoking, and clinical variables such as type of MI and its side effects were collected as individual-clinical variables.
The data of air pollution in Isfahan were gathered on a daily basis from Ahmadabad, Azadi, Sepah, Azadegan, Segzi, Vali-e-Asr, Vahid, and Khajoo air quality control stations affiliated with the Environment Protection Organization. Meteorological variables such as air temperature (minimum and maximum), relative humidity, precipitation, and altitude were also gathered from the meteorology stations in Isfahan. The mean of meteorological variables and PM10, NO2, CO, SO2, and O3 were used for air quality assessment.
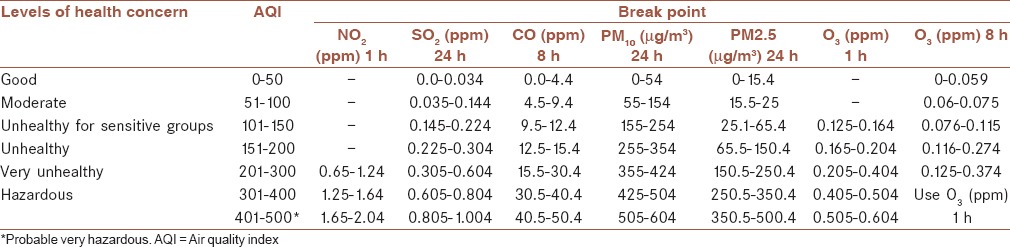
Each pollutant concentration in each station was converted to air quality index (AQI) using the equation below on a daily basis. The air pollutant breakpoints are shown in Table 1.[20]
Table 1.
Classes of pollutants’ concentration for AQI calculation

Where:
IP = The (air quality) index,
CP = The pollutant concentration,
BPHi = The concentration breakpoint that is ≥ Cp,
BPLo = The concentration breakpoint that is ≤ Cp,
IHi = The index breakpoint corresponding to BPHi, and
ILo = The index breakpoint corresponding to BPLo.
The two-level logistic regression modeling was used to determine the relationship among air pollution, meteorological, and individual variables in the patients. OR was used to determine the mortality factors as the dependent variables. Individual variables of patients were considered as the first level, and local variables and hospital admission as the second level. Individual variables for the first level, and air pollution and meteorological variables for the second level were entered into the model. The confidence interval 95% and Stata software (Stata Corp. 2011. Stata statistical software: Release 14. College Station, Stata Corp LP, TX, USA) were used to calculate the OR. The independent t-test and Chi-square were used for data analysis. First, the univariate analysis and then the multiple analyses were performed, and the adjusted ORs were reported.
RESULTS
A total of 611 patients with acute MI were studied during a year. 444 (72.2%) patients were male and the rest were female. 7.4% of the patients incurred on hospital mortality from acute MI. The mean and standard deviation (SD) outbreak age of MI in Isfahan metropolis in men, women, and all patients were 68 ± 12.3, 60 ± 13.9, and 13 ± 2.62 years, respectively. The maximum mortality rate was obtained in spring (2.41%). The demographic and clinical risk factors in the studied patients for mortality from MI are shown in Table 2.
Table 2.
Demographic and clinical characteristics under study

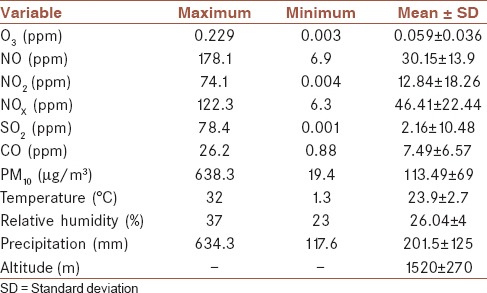
Mean (±SD) daily O3, NO, PM10, and SO2 was derived, respectively, 0.059 ± 0.036, 30.15 ± 13.9, 113.49 ± 69, and 2.16 ± 10.48. The mean of air pollution parameters and meteorological variables in Isfahan are shown in Table 3. Of the air pollution parameters, PM10 had the maximum mean concentration (49.113 ppm), followed by NOX, NO, NO2, CO, SO2, and O3.
Table 3.
Descriptive indices of air pollution and meteorological variables
The number of unhealthy (AQI = 151-200) samples for NO2, SO2, CO, PM10, and O3 was obtained 21, 33, 4, 31, and 142, respectively. PM10 was derived hazardous only 3 times. The sum of calculated AQI for each pollutant in each class in all eight Isfahan stations was calculated according to Table 4. The greatest number of AQI was obtained as a good range for CO and NO2, moderate for PM10 and SO2, and unhealthy for O3.
Table 4.
The number of samples for AQI in each of pollutant in all meteorological stations

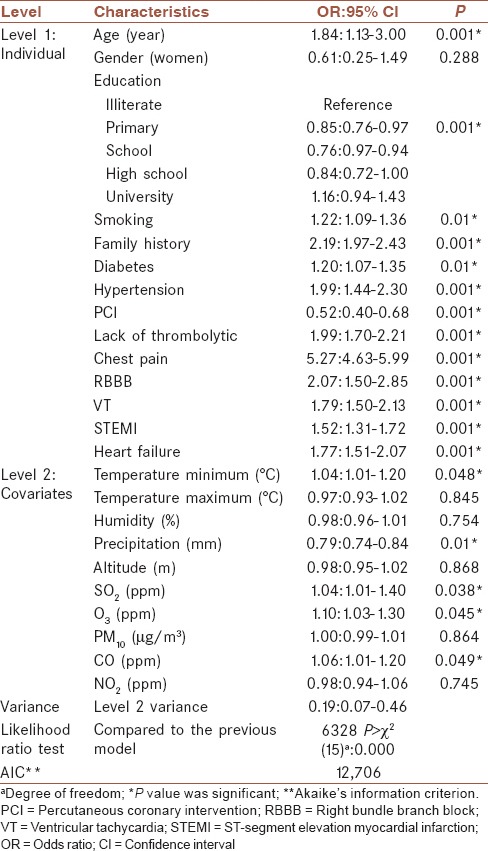
The adjusted OR of mortality was derived 2.07 (95% CI: 1.5-2.85) for right bundle branch block, 1.5 (95% CI: 1.3-1.7) for ST-segment elevation MI, 1.84 (95% CI: 1.13-3) for age, 1.06 (95% CI: 1.01-1.20) for CO, 1.1 (95% CI: 1.03-1.30) for O3, and 1.04 (95% CI: 1.01-1.4) for SO2, all of which were considered as risk factors of mortality. However, OR of mortality was 0.79 for precipitation (95% CI: 0.74-0.84) and 0.52 for angioplasty (95% CI: 0.4-0.68) were considered as protective factors of mortality. The individual characteristics including age, history of MI in the immediate family, hypertension, and diabetes were significantly associated with mortality from MI. The indices of air pollution including SO2, CO, O3, and environmental factors such as the precipitation and temperature were determinants of mortality in patients with MI. Determinant ORs for mortality in patients with MI are shown in Table 5.
Table 5.
OR for in-hospital mortality associated factors in patients by multi-level analysis model
DISCUSSION
MI mortality determinants’ ORs due to the personal, environmental factors, and air pollution indicators were simultaneously calculated and reported in this study. This study showed that the demographic and clinical risk factors in patients with MI, was the most important predictor of mortality in patients. Also, although SO2, O3, CO, and precipitation had an approximately significant role in the model of factors associated with mortality alongside other variables, other air pollution indices had no decisive and effective role in the mortality of the patients with heart attack. In a meta-analysis, it was reported that the gaseous pollutants had an important role in the increased risk of diabetes as compared to the particles.[4]
The result of our study appears to be in line with the above study. In a study in Gothenburg, Sweden, the reverse effect of temperature and hospital MI admission were obtained,[11] which is consistent with the present study. The results of our study are also consistent with a study in Tehran, Iran, reporting a direct correlation between the air pollution and incidence of MI.[12] A study reported that PM2.5 had a direct relationship with arrhythmias, atrial fibrillation, and pulmonary embolism. NO2 also led to an increase in the risk of MI. However, air pollution, with the increase of segment, generally had no significant effect on MI and stroke.[18] The results of our study are consistent with these studies. A study reported that there was an inverse relationship between the O3 and out-of-hospital mortality from coronary heart disease. However, there is a direct relationship with acute hospital MI, especially for women, the elderly and patients with chronic diseases.[21] In our study, O3 was found to be an important risk factor for hospital mortality from acute MI, which corresponded with the reference study.
A study in Tehran, Iran reported that air pollutants, especially PM10, SO2, NO2, and NOX, played an important role in the development of multiple sclerosis.[22] Therefore, these pollutants were determinant in our study. Early diagnosis and predisposing factors play an important role in the prevention and control of cardiovascular diseases.[23] Therefore, it seems necessary to avoid the cardiovascular disease through monitoring and evaluation of air pollution and programming to prevent and control. A study in Tabriz, Iran showed that with the increase by 10 mg/m3 in concentration of O3, NO2, and SO2, the risk of heart attack increased by about 0.58, 0.38, and 0.44%, respectively. Moreover, these emissions led to increased hospital admissions due to a heart attack.[24] Our study is in agreement with the study of Tabriz.
In a study in Kerman, Iran the relationship between the mortality from cardiovascular diseases and air pollution was investigated by Poisson regression (crude and adjusted). Statistical analysis in the initial regression only showed an association between ozone and mortality due to the cardiovascular disease in women. Mortality was higher in women with cardiovascular disease with an increase in ozone. However, in both crude and adjusted regression models, there was no relationship between the increased pollution and mortality from cardiovascular patients and no significant association between the air pollution and cardiovascular mortality.[25] In Tehran, the effects of air pollution on the emergency admissions for the cardiovascular and respiratory disease have been studied. Results have shown that increased levels of CO and O3 during two consecutive days resulted in a significant increase in the emergency admissions of cardiovascular patients on the 3rd day. In addition, the increased levels of O3, PM2.5, NO2, and CO contributed to increased admissions due to respiratory disease in the emergency centers.[26] In an important study, the exposure to the particle and ozone could contribute to the decrease in vagal tone, and resulted in reduced heart rate variability (HRV).[27]
In a study in Boston, the USA, the association between the ambient air pollution and HRV was investigated and a reduction of HRV was seen. Our results correspond with the Boston study and ozone contributed to the modeling of the determinants of mortality. In five cities in Europe, the relationship between the air pollution and MI survivors was studied. The results showed that there was a relationship between the air pollution and readmissions in MI survivors.[28] In another study in Tehran, Iran the relationship between air pollution and admissions for cardiac and respiratory disease was examined. It was observed that carbon monoxide and particulate matter with higher than standard levels are the main components of air pollutants. The results show that the number of patients hospitalized for heart and respiratory diseases is positively associated with the concentration of CO, NO2, SO2, and PM10.[29] In Kaohsiung, Taiwan, the relationship between air pollution and heart attacks in the single- and two-pollutant models were investigated. The results showed a significant correlation between the levels of PM10, NO2, SO2, CO, and O3, and cerebral hemorrhagic strokes and ischemic strokes in the single-pollutant models on hot days (more than 20°C). Also, in the single-pollutant models on cold days (below 20°C), a significant relationship was observed only between the CO and ischemic strokes. In the two-pollutant models, PM10 and NO2 simultaneously had a relationship with MI and stroke. The effects of CO, SO2, and O3 in most cases were not significant when NO2 or PM10 was controlled.[30]
A study in Canada has analyzed the relationship between the air pollution and the number of cardiac and respiratory visits in the emergency department. The analysis has shown a consistent relationship between the average daily concentrations of CO and NO2, and cardiac visits, and ozone concentration and respiratory visits. Also during warm seasons, there was a high correlation between PM10 and PM2.5, and visits to patients with asthma.[31] The knowledge of the role of environmental and biological factors could be used to improve the prevention measures and educational strategies, especially in people at risk of diseases. A limitation of the present study was a failure to gather the data on ejection fraction as it is one of the predictive factors of mortality, needing to be addressed in future studies. Prospective cohort study and follow-up of the patients for the event of interest at frequent intervals are recommended in future investigations. Implementing educational strategies, motivating people to visit doctors early, and increasing access to treatment, especially in the individuals at MI risk could reduce the mortality due to MI.[32,33]
CONCLUSIONS
In the present study, the association of individual and clinical risk factors, as well as, air pollution indices with mortality in MI patients was investigated. The risk factors and predictive factors significantly associated with mortality from MI were reported, as well. Together, the air pollution indices, in addition to the risk factors, and predictive factors, should be particularly addressed to control the mortality from MI. This study and clinical studies of patients with acute MI show that the individual risk factors are significant predictors of mortality in patients. The present study showed that although SO2, O3, CO, and precipitation contributed nearly significantly to the model of mortality-associated factors alongside other variables. Other air pollution indices had no decisive and effective role in MI mortality.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
AUTHOR'S CONTRIBUTION
AA, MS, and AB designed the research protocol and supervised its implementation. AA, NM, and SF designed analysis. AB, SF, and NM drafted the article. All of the authors reviewed drafts of the article and contributed to the conceptual framework.
Acknowledgments
The authors gratefully thank Mrs. Izadpanah, Dr. Motasadi, and Dr. Rashidi in the Environment Protection Organization and also Cardiovascular Disease Prevention Department at the Iran Ministry of Health and Medical Education for offering the data as well as Research and Technology Deputy of Shahrekord University of Medical Sciences, Shahrekord, Iran. Data collection for this research was supported by the Department of Cardiology of Ministry of Health and Medical Education, respectful personnel in the treatment deputies of universities of medical sciences and the nurses in cardiology wards of hospitals across Iran as well as cardiologists, officials, and advisors of Iran's Myocardial Infarction Registry Program. The funding sources played no role in the study design, data analysis, and manuscript writing, or in the decision to submit this manuscript for publication.
REFERENCES
- 1.Ahmadi A, Soori H, Mehrabi Y, Etemad K, Samavat T, Khaledifar A. Incidence of acute myocardial infarction in Islamic Republic of Iran: A study using national registry data in 2012. East Mediterr Health J. 2015;21:5–12. doi: 10.26719/2015.21.1.5. [DOI] [PubMed] [Google Scholar]
- 2.Ahmadi A, Soori H, Sajjadi H. Modeling of in hospital mortality determinants in myocardial infarction patients, with and without type 2 diabetes, undergoing pharmaco-invasive strategy: The first national report using two approaches in Iran. Diabetes Res Clin Pract. 2015;108:216–22. doi: 10.1016/j.diabres.2015.02.018. [DOI] [PubMed] [Google Scholar]
- 3.Ahmadi A, Soori H, Mobasheri M, Etemad K, Khaledifar A. Heart failure, the outcomes, predictive and related factors in Iran. J Mazandaran Univ Med Sci. 2014;24:180–8. [Google Scholar]
- 4.Janghorbani M, Momeni F, Mansourian M. Systematic review and metaanalysis of air pollution exposure and risk of diabetes. Eur J Epidemiol. 2014;29:231–42. doi: 10.1007/s10654-014-9907-2. [DOI] [PubMed] [Google Scholar]
- 5.Nasri H, Ahmadi A, Baradaran A, Momeni A, Nasri P, Mardani S, et al. Clinicopathological correlations in lupus nephritis; a single center experience. J Nephropathol. 2014;3:115–20. doi: 10.12860/jnp.2014.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ahmadi A, Mobasheri M, Hashemi-Nazari SS, Baradaran A, Choobini ZM. Prevalence of hypertension and type 2 diabetes mellitus in patients with colorectal cancer and their median survival time: A cohort study. J Res Med Sci. 2014;19:850–4. [PMC free article] [PubMed] [Google Scholar]
- 7.Nasri H, Behradmanesh S, Ahmadi A, Rafieian-Kopaei M. Impact of oral vitamin D (cholecalciferol) replacement therapy on blood pressure in type 2 diabetes patients; A randomized, double-blind, placebo controlled clinical trial. J Nephropathol. 2014;3:29–33. doi: 10.12860/jnp.2014.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ahmadi A, Hasanzadeh J, Rajaeifard A. Metabolic control and care assessment in patients with type 2 diabetes in chaharmahal & bakhtiyari province 2008. Iran J Endocrinol Metab. 2009;11:33–9. [Google Scholar]
- 9.Ahmadi A, Soori H, Khaledifar A. In-hospitalcase fatality rate and cox proportional-hazards model for risk factors of mortality due to myocardial infarction in Iran's hospitals: A national study. Int Cardiovasc Res J. 2015;9:45–51. [Google Scholar]
- 10.Ahmadi A, Soori H, Sajjadi H, Nasri H, Mehrabi Y, Etemad K. Current status of the clinical epidemiology of myocardial infarction in men and women: A national cross-sectional study in iran. Int J Prev Med. 2015;6:14. doi: 10.4103/2008-7802.151822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wichmann J, Rosengren A, Sjöberg K, Barregard L, Sallsten G. Association between ambient temperature and acute myocardial infarction hospitalisations in Gothenburg, Sweden: 1985-2010. PLoS One. 2013;8:e62059. doi: 10.1371/journal.pone.0062059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nabavi SM, Jafari B, Jalali MS, Nedjat S, Ashrafi K, Salahesh A. Environmental air pollution and acute cerebrovascular complications: An ecologic study in tehran, iran. Int J Prev Med. 2012;3:723–9. [PMC free article] [PubMed] [Google Scholar]
- 13.Ahmadi A, Soori H, Mehrabi Y, Etemad K, Khaledifar A. Epidemiologic pattern of myocardial infarction and modeling risk factors relevant to in-hospital mortality: The first results from Iranian myocardial infarction registry. Kardiol Pol. 2015;73:451–7. doi: 10.5603/KP.a2014.0230. [DOI] [PubMed] [Google Scholar]
- 14.Ahmadi A, Golshahi J, Khaledi-Far A, Soori H, Mehrabi Y, Etemed K. The pattern of in-hospital mortality of myocardial infarction and associated factors in Iran: A national study. J Isfahan Med Sch. 2015;32:2174–83. [Google Scholar]
- 15.Ahmadi A, Sajjadi H, Etemad K, Khaledifar A, Mobasherii M. Epidemiological characteristics and determinants of mortality in acute coronary syndrome in Iran. J Mazandaran Univ Med Sci. 2015;24:1–9. [Google Scholar]
- 16.Poursafa P, Mansourian M, Motlagh ME, Ardalan G, Kelishadi R. Is air quality index associated with cardiometabolic risk factors in adolescents? The CASPIAN-III study. Environ Res. 2014;134:105–9. doi: 10.1016/j.envres.2014.07.010. [DOI] [PubMed] [Google Scholar]
- 17.Qorbani M, Yunesian M, Fotouhi A, Zeraati H, Sadeghian S. Effect of air pollution on onset of acute coronary syndrome in susceptible subgroups. East Mediterr Health J. 2012;18:550–5. doi: 10.26719/2012.18.6.550. [DOI] [PubMed] [Google Scholar]
- 18.Janghorbani M, Piraei E. Association between air pollution and preterm birth among neonates born in Isfahan, Iran. J Res Med Sci. 2013;18:875–81. [PMC free article] [PubMed] [Google Scholar]
- 19.Ahmadi A, Soori H, Etemad K, Mehrabi Y, Hojabri S. Geographical pattern of in-hospital mortality due to myocardial infarction in Iran. J Mazandaran Univ Med Sci. 2015;25:1–9. [Google Scholar]
- 20.Ministry of Health and Medical Education. A Guide to Calculation, Determination and Announcement of Air Quality Index. Environmental and Occupational Center, Institute for Environmental Research. 2013 (In Persian) [Google Scholar]
- 21.Nuvolone D, Balzi D, Pepe P, Chini M, Scala D, Giovannini F, et al. Ozone short-term exposure and acute coronary events: A multicities study in Tuscany (Italy) Environ Res. 2013;126:17–23. doi: 10.1016/j.envres.2013.08.002. [DOI] [PubMed] [Google Scholar]
- 22.Heydarpour P, Amini H, Khoshkish S, Seidkhani H, Sahraian MA, Yunesian M. Potential impact of air pollution on multiple sclerosis in Tehran, Iran. Neuroepidemiology. 2014;43:233–8. doi: 10.1159/000368553. [DOI] [PubMed] [Google Scholar]
- 23.Kelishadi R, Poursafa P. A review on the genetic, environmental, and lifestyle aspects of the early-life origins of cardiovascular disease. Curr Probl Pediatr Adolesc Health Care. 2014;44:54–72. doi: 10.1016/j.cppeds.2013.12.005. [DOI] [PubMed] [Google Scholar]
- 24.Ghozikali MG, Mosaferi M, Safari GH, Jaafari J. Effect of exposure to O3, NO2, and SO2 on chronic obstructive pulmonary disease hospitalizations in Tabriz, Iran. Environ Sci Pollut Res Int. 2015;22:2817–23. doi: 10.1007/s11356-014-3512-5. [DOI] [PubMed] [Google Scholar]
- 25.Khanjani N, Bahrampour A. Temperature and cardiovascular and respiratory mortality in desert climate. A case study of Kerman, Iran. Iranian J Environ Health Sci Eng. 2013;10:11. doi: 10.1186/1735-2746-10-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Shahi AM, Omraninava A, Goli M, Soheilarezoomand HR, Mirzaei N. The effects of air pollution on cardiovascular and respiratory causes of emergency admission. Emerg. 2014;2:107–14. [PMC free article] [PubMed] [Google Scholar]
- 27.Gold DR, Litonjua A, Schwartz J, Lovett E, Larson A, Nearing B, et al. Ambient pollution and heart rate variability. Circulation. 2000;101:1267–73. doi: 10.1161/01.cir.101.11.1267. [DOI] [PubMed] [Google Scholar]
- 28.von Klot S, Peters A, Aalto P, Bellander T, Berglind N, D’Ippoliti D, et al. Ambient air pollution is associated with increased risk of hospital cardiac readmissions of myocardial infarction survivors in five European cities. Circulation. 2005;112:3073–9. doi: 10.1161/CIRCULATIONAHA.105.548743. [DOI] [PubMed] [Google Scholar]
- 29.Khalilzadeh S, Khalilzadeh Z, Emami H, Masjedi MR. The relation between air pollution and cardiorespiratory admissions in Tehran. Tanaffos. 2009;8:35–40. [Google Scholar]
- 30.Tsai SS, Goggins WB, Chiu HF, Yang CY. Evidence for an association between air pollution and daily stroke admissions in Kaohsiung, Taiwan. Stroke. 2003;34:2612–6. doi: 10.1161/01.STR.0000095564.33543.64. [DOI] [PubMed] [Google Scholar]
- 31.Stieb DM, Szyszkowicz M, Rowe BH, Leech JA. Air pollution and emergency department visits for cardiac and respiratory conditions: A multi-city time-series analysis. Environ Health. 2009;8:25. doi: 10.1186/1476-069X-8-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ahmadi A, Soori H, Mehrabi M, Etemad K, Sajjadi H, Sadeghi M. Predictive factors of hospital mortality due to myocardial infarction: A multilevel analysis of Iran's national data. Int J Prev Med. 2015;6:15. doi: 10.4103/2008-7802.170026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ahmadi A, Soori H, Mehrabi M, Etemad K. Spatial analysis of myocardial infarction in iran: National report from the Iranian myocardial infarction registry. J Res Med Sci. 2015;20:434–9. doi: 10.4103/1735-1995.163955. [DOI] [PMC free article] [PubMed] [Google Scholar]