

Objectives
The use of electroconvulsive therapy (ECT) varies across countries. The aim of this study was to describe and explore the use of ECT in Sweden in 2013.
Methods
The Swedish mandatory patient register of the National Board of Health and Welfare includes information on diagnoses and treatments, including ECT. All 56 hospitals that provide ECT in Sweden also report to the nonmandatory national quality register for ECT, which contains information on patient and treatment characteristics. In this study, we combined data from both registers. In addition, all hospitals responded to a survey concerning equipment and organization of ECT.
Results
We identified 3972 unique patients who received ECT in Sweden in 2013. This translates into 41 ECT-treated individuals per 100,000 inhabitants. Of these patients, 85% opted to participate in the quality register. The median age was 55 years (range, 15–94 years), and 63% were women. The indication was depression in 78% of the treatment series. Of 4 711 hospitalized patients with severe depression, 38% received ECT. The median number of treatments per index series was 7. Unilateral treatment was used in 86% of the series.
Conclusions
In Sweden, ECT is used at a relatively high rate as compared with other western countries, and the rate was unchanged from the last survey in 1975. However, there is room for improvement in the specificity of use and availability of ECT for disorders where ECT is considered a first-line treatment.
Key Words: electroconvulsive therapy, depression, epidemiology
Electroconvulsive therapy (ECT) is an established and effective treatment for severe affective disorders and is used worldwide.1 Mandatory reporting and ECT registers covering entire countries are sparse, and data on the use and practice of ECT are mostly based on occasional national surveys. In a recent systematic overview of ECT worldwide, Leiknes et al2 showed a large global variation in the indications, treatment techniques, and availability of ECT. In western countries, the patients tended to be older women with depression, in contrast to Asian countries where the patients tended to be younger men with schizophrenia. Bilateral electrode placement was more common than unilateral electrode placement, but in Europe and Australia/New Zealand, unilateral electrode placement was preferred. Brief-pulse modified ECT was most common, but sine-wave and unmodified ECT were still in use. General trends were that within countries there were only a few institutions providing ECT, training was inadequate, and guidelines were not followed. The availability in terms of treated person rate varied from 1.1 to 54 per 100,000. Legal requirements and consent procedures also varied across countries.2,3 In European countries except Sweden, Finland, Denmark, and Slovakia, written consent is necessary.3
The Swedish National Board of Health and Welfare estimated the use of ECT in Sweden in 2010 to be 36.7 per 100 000,4 but the use and practice of ECT in Sweden has not been systematically investigated since 1975, when 3482 patients (42 per 100,000) received ECT.5
The aim of this study was to explore and describe the use of ECT in Sweden in 2013, using data from a national mandatory reporting register, a national quality register for ECT, and a survey.
MATERIALS AND METHODS
All Swedish hospitals report to the mandatory patient register of the National Board of Health and Welfare. The register includes information on diagnosis and treatment (including treatment with ECT) and is organized according to personal identification number.
In 2008, a regional ECT register was started in 3 counties in Sweden. The National Board of Health and Welfare and the Swedish Psychiatric Association considered it important to document the use of ECT in Sweden in more detail, and in 2011, the regional register was expanded to a national quality register with support from the Swedish Association of Local Authorities and Regions. One of the aims of the national quality register for ECT is to enable monitoring of the Swedish clinical guidelines for ECT issued in 2014.6 The register holds detailed information on the patient characteristics, severity of symptoms, indications for therapy, electrical stimulus and seizures, course of treatment, pharmacotherapy (including the post-ECT medication used to reduce the risk of relapse), and side effects. The register is used for both quality assurance and for research. It is a nonmandatory register, and every patient has the option of declining participation. All 56 hospitals that provided ECT in Sweden reported to the nonmandatory national quality register for ECT in 2013. In addition, a questionnaire was sent out to all hospitals providing ECT to survey the apparatus used and the organization.
Information from the mandatory patient register and the national quality register for ECT was combined to identify all patients treated with ECT in Sweden in 2013. SPSS version 21 (SPSS Inc., Chicago, IL) was used for the statistical analyses. The Regional Ethical Vetting Board in Uppsala approved this study. The patients were informed about the quality register and had the option to decline participation.
RESULTS
Treatment Rate and Demographics of the ECT Population
In total, 3972 patients were identified that had received ECT in Sweden in 2013. The population of Sweden was 9,644,864 inhabitants in December 2013, according to Statistics Sweden. This means that 41 inhabitants per 100,000 were treated with ECT. The proportion ranged from 26 per 100,000 to 62 per 100,000 across the different counties in Sweden (Fig. 1). The proportion varied from 0 per 100,000 in persons aged younger than 14 years to 77 per 100,000 in persons aged 75 to 84 years (Fig. 2).
FIGURE 1.
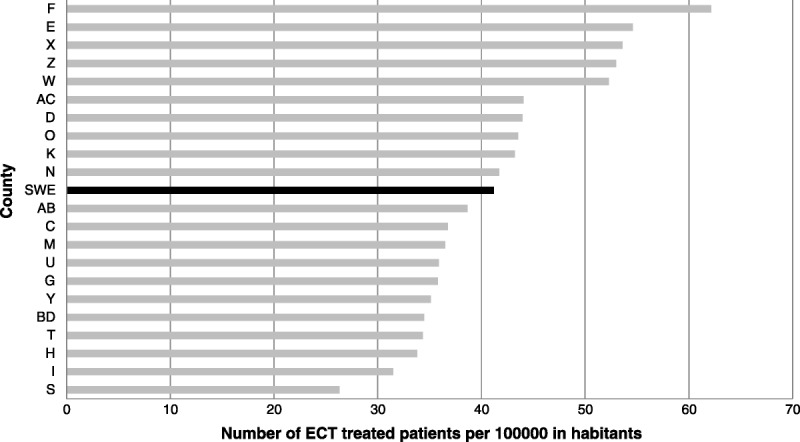
The number of ECT-treated patients per 100 000 inhabitants in different counties in Sweden. Sweden as a whole is shown in black. The counties are represented by their official county letter. Key: AB: Stockholm County Council, AC: Västerbotten County Council, BD: Norrbotten County Council, C: Uppsala County Council, D: Sörmland County Council, E: Region Östergötland, F: Region Jönköping County, G: Region Kronoberg, H: Kalmar County Council, I: Region Gotland, K: Blekinge County Council, M: Region Skåne, N: Region Halland, O: Region Västra Götaland, S: Värmland County Council, T: Region Örebro County, U: Västmanland County Council, W: Dalarna County Council, X: Region Gävleborg, Y: Västernorrland County Council, Z: Region Jämtland Härjedalen.
FIGURE 2.
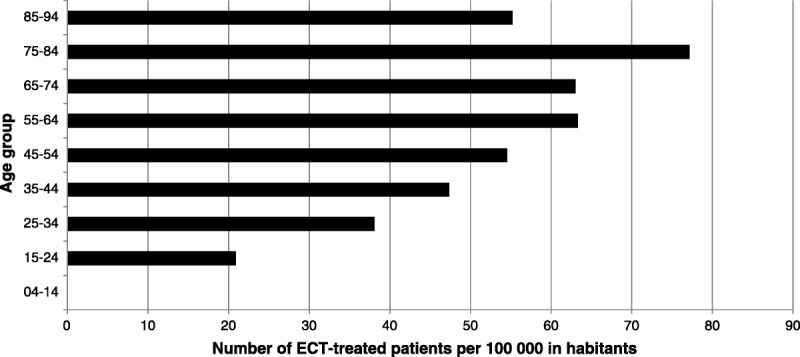
The number of ECT-treated patients per 100,000 inhabitants in different age groups in Sweden.
Of the patients treated with ECT in Sweden in 2013, 85% opted to participate in the national quality register. The register contained 3246 patients that received a total of 35,875 ECT sessions divided into 3746 index series and 738 continuation series. The median age of these patients was 55 years (range, 15–94 years), and 63% were women. Six patients were below 18 years of age, and 20 patients were older than 90 years.
Diagnostic Indications
The indications reported to the quality register that conform to the Swedish clinical guidelines for ECT are listed in Table 1. In 20% (894/4484) of the treatment series, the indication for ECT was not listed in clinical guidelines. The most common indications in this group were affective disorders not otherwise specified (433/894). Obsessive-compulsive disorder (19 treatment series), anxiety disorders (17 treatment series), and borderline personality disorder (13 treatment series) were the most common indications for ECT that are not recommended by the Swedish clinical guidelines.
TABLE 1.
Indications for ECT That Conform to the Swedish Clinical Guidelines
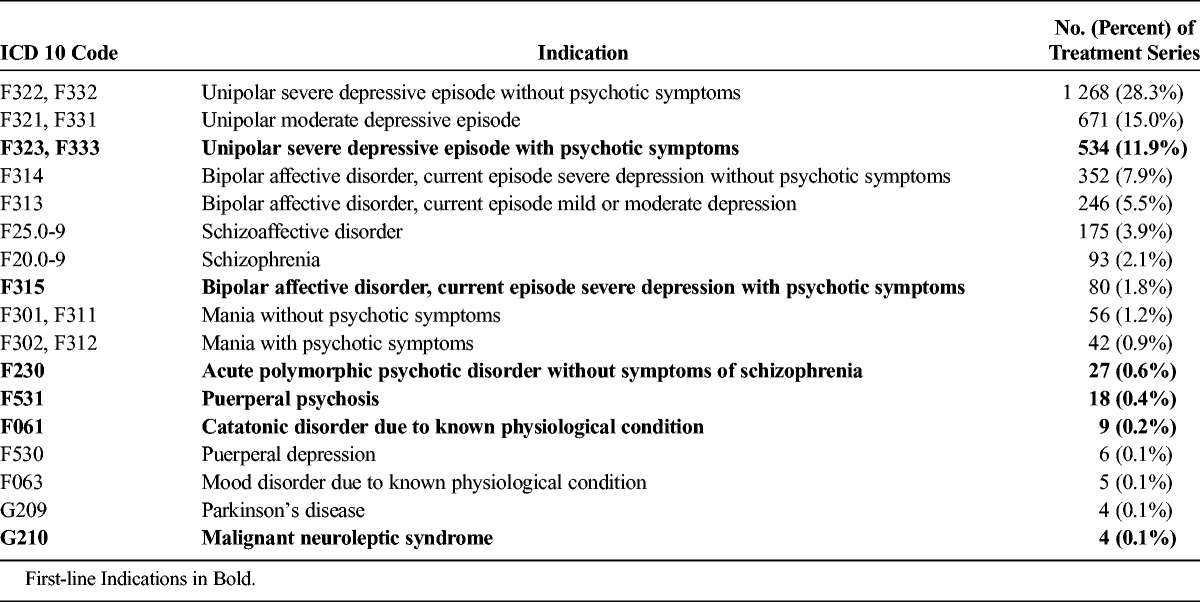
Of 4711 hospitalized patients that were treated for severe depression in 2013 according to the mandatory register, 38% received ECT. The proportion of severely depressed inpatients that received ECT was higher among women (1105/2771; 40%) than men (661/1940; 34%). According to the Swedish clinical guidelines for ECT, ECT is the first-line treatment for catatonia, cycloid psychosis, psychotic depressions, puerperal psychosis, and malignant neuroleptic syndrome. In 2013, there were 1694 inpatients with one of these diagnoses, and 38% of these received ECT. This proportion was higher among women (417/1028; 41%) than men (233/666; 35%). Of 29 inpatients younger than 18 years with one of these diagnoses, three received ECT (10%).
ECT Practice Parameters
The median number of treatments per index series was seven (interquartile range, 6–9) (reported in all treatment series). Electrode placement was reported in all index series. Unilateral treatment was used in 86% of the treatment series, bitemporal treatment in 11%, and bifrontal treatment in 3%. Of the patients in the quality register, 11% went on to receive outpatient continuation ECT after their index series.
MECTA devices (MECTA Corp, Lake Oswego, OR) were used in 44 hospitals (79%), and Thymatron devices (Somatic, LLC, Lake Bluff, IL) were used in the remaining 12 hospitals (21%). The stimulus parameters for the electrical stimulus at first ECT were reported to the register in 2263/3746 (60%) of index series. The median stimulus was as follows: pulse width, 0.5 ms; frequency, 70 Hz; duration, 7.5 s; current, 800 mA; and charge, 358 mC. In Sweden, the apparatus for ECT can deliver higher charges than the apparatus permitted in the United States. In 13% of the treatment series, the charge was greater than 576 mC. The median duration of the epileptic seizure as measured with electroencephalogram was 36 s (reported in 2155/3746 index series).
Anesthesia
Anesthesia was provided by an anesthesiologist in 41% of the hospitals and by an anesthesia nurse in 24% of the hospitals, according to the survey. In the remaining hospitals, anesthesiologists and anesthesia nurses alternated. Propofol was used in 23% of the treatment series (median dosage, 100 mg), and pentobarbital was used in the remaining 77% (median dosage, 300 mg) (doses reported in 2361/3746 index series).
Organization
According to the survey, all hospitals provided ECT for outpatients, and all hospitals except two provided ECT for inpatients. A few persons alternated to deliver the electrical stimulus in each of the 56 hospitals, and they had various levels of training. Psychiatrists participated in delivering ECT in 21 hospitals, anesthesiologists participated in 2 hospitals, psychiatric residents participated in 11 hospitals, nurses participated in 49 hospitals, and nursing assistants (unlicensed assistant personnel) participated in 20 hospitals.
Legal Requirements and Consent
Before ECT was delivered, patients were provided with written and oral information on the treatment options and their benefits and risks. Verbal consent is standard for ECT and surgical procedures in Sweden. In the patient’s chart, the psychiatrist noted when information was provided and the patient’s attitude toward ECT. It is possible to administer ECT to a patient that has not consented if the patient is treated under the Swedish act on compulsory psychiatric care. Patients qualify for the Swedish act on compulsory psychiatric care if 2 physicians confirm that the patient has a severe mental disorder and an indispensable need for psychiatric care and the patient does not consent to the psychiatric care. Less than 15% of the patients that received ECT in Sweden in 2013 were treated under the Swedish act on compulsory psychiatric care.
DISCUSSION
This is the first systematic study of the use and practice of ECT in Sweden since 1975. We found that the proportion of the population of Sweden that received ECT was nearly the same in 2013 (41 per 100,000) as in 1975 (42 per 100,000).5 Thus, despite the increased number of drugs used to treat severe mental illness, ECT remains an important treatment option.
From a global perspective, Sweden has a relatively high rate of use of ECT,2 similar to that in Belgium (41 per 100,000 inhabitants)7 and Australia (40–44 per 100,000 inhabitants).8,9 By contrast, very low rates of use have recently been reported in Croatia10 (1.3 per 100,000 inhabitants) and Ukraine.11 Higher rates were reported in Slovakia (29 per 100,000),12 Canada (23–25 per 100,000),13 and Norway (24 per 100,000).14 The rate of use in Germany in 2008 was 3.5 per 100,000 inhabitants and was increasing,15 in contrast to a recent study from the United States, where the rate of inpatient hospital care including ECT was estimated to be 7.2 per 100,000 inhabitants and declining.16 Although it seems that Sweden has a relatively high rate of use of ECT, we cannot exclude the possible impact of the difference between occasional national surveys and a national mandatory reporting system. We believe that Sweden in this aspect has a unique opportunity to provide reliable data on the national use of ECT.
In accordance with data from other western countries,2 we found a predominance of women receiving ECT, and the median age of patients receiving ECT was above middle age. Electroconvulsive therapy is not prohibited for minors, but the treatment is not recommended for children by the National Board of Health and Welfare; our data show that there was no use of ECT for children below the age of 15 years.
The rate of use of ECT varies between counties in Sweden; the reasons for this difference still need to be elucidated. Regional variation within countries has been attributed to service factors or barriers to access as well as regional treatment traditions.13,14,17–19 Different regional treatment traditions might also influence the within-country availability of ECT in Sweden, as might the regional differences of availability of anesthesiologists and psychiatrists.
Depression and affective disorders were the most common indications for ECT in Sweden in 2013, and this is in line with the practice in the rest of Europe and in North America.2 A high proportion of patients received ECT for indications that are in line with clinical guidelines.6,20 However, the pattern of use revealed in the quality register also showed that ECT is used, albeit sparsely, in disorders where the treatment is not recommended. The guidelines support the use of ECT for severe and moderate depression but not for mild depression. If the diagnosis is depression not otherwise specified, the indication for ECT is not considered accurate enough according to the Swedish clinical guidelines, pointing to the importance of accurately selecting patients for ECT.
In addition, 62% of inpatients with a first-line indication for ECT according to Swedish clinical guidelines did not receive ECT. Electroconvulsive therapy is a highly effective treatment for severe depression,21,22 is superior to pharmacological treatment,22,23 and is more beneficial in psychotic depression than in less-severe depression.24 Electroconvulsive therapy also offers prompt and rapid symptom relief in other life-threatening disorders, such as catatonic states.25 In these conditions, the patient’s need for rapid symptom relief is obvious. In addition, there is increasing evidence that structural reductions in different brain regions relate to the course of illness in depression,26,27 including the duration of each episode,28,29 emphasizing the importance of rapid and marked symptomatic improvement. Our data show that there is room for improvement in the availability of ECT in Sweden, as its use was delayed in disorders where ECT is recommended as a first-line treatment. In particular, 90% of adolescent inpatients with these diagnoses did not receive ECT, indicating that many adolescents were denied the benefit of ECT.
Written consent for ECT is common in Europe,3 but the suggestion to standardize the consent procedure for ECT across Europe is problematic because of different traditions between the countries. Written consent is not used for any medical or surgical procedures in Sweden, and verbal consent is standard.3 In 2014, a new law was issued in Sweden, the patient law (Patientlag (2014:821)), relevant for all medical care, except for patients treated under the law concerning involuntary psychiatric treatment (Lag om psykiatrisk tvångsvård (1991:1128)). According to the patient law, complete information to the patient is mandatory. As concerns consent, it is said that the patients´ right to self-determination and integrity must be respected. Furthermore, it is stated that the medical care is not allowed to be given without the consent of the patient. However, it is clearly stated that the consent can be communicated in writing, orally or in some other way that indicates that the patient consents to the medical care. It would surprise patients if they needed to sign a form to receive ECT but could have brain surgery or heart transplantation without signing a consent form. Therefore, if written consent were to be required in Sweden, only for ECT and not for other treatments, there is a risk that mental disease and ECT would be stigmatized even more than it is today. Moreover, in situations where the need for ECT is most urgent, decision making and capacity to fill in forms are often impaired. Rather, we suggest that as soon as it is possible, the patient and next of kin should be invited to participate in decisions regarding adjustments to optimize treatment benefit.
In most countries, ECT is provided by a psychiatrist. In Sweden, only psychiatrists can prescribe ECT, but the ECT was often delivered by a nurse or even nursing assistant, and psychiatrists participated in the delivery of ECT in a minority of hospitals. There are no national regulations concerning the qualifications of the personnel delivering ECT. Most nurses and nursing assistants that deliver ECT have only a few days of training on the theoretical background and practice of ECT. We as authors do not support the delegation of ECT to unlicensed assistant personnel and recommend that Swedish psychiatrists become more involved in the delivery of ECT. However, as the praxis differs in different parts of Sweden, we intend to use the quality register to compare the outcome, the side effects and the complications of ECT delivered by psychiatrists with ECT delivered by nurses or nursing assistants.
CONCLUSIONS
This is the first study of the use of ECT in Sweden since 1975. We found that, in Sweden, ECT is used more often than it is used in most other western countries and that the treatment rate was unchanged since the last survey in 1975. The selection of patients for ECT and the treatment technique was similar to that in other western countries, but the consent procedure and the involvement of nurses and nursing assistants in the delivery of ECT differentiate Sweden from most other countries. We also conclude that there is room for improvement in the specificity of use and availability of ECT in disorders where ECT is considered a first-line treatment.
Footnotes
Research based on the national quality register for ECT is supported by the Swedish foundation for strategic research. The authors have no conflicts of interest or financial disclosures to report.
REFERENCES
- 1. Swartz C. Electroconvulsive and Neuromodulation Therapies. Cambridge; New York: Cambridge University Press; 2009. [Google Scholar]
- 2. Leiknes KA, Jarosh-von Schweder L, Hoie B. Contemporary use and practice of electroconvulsive therapy worldwide. Brain Behav. 2012; 2: 283– 344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Gazdag G, Takacs R, Ungvari GS, et al. The practice of consenting to electroconvulsive therapy in the European Union. J ECT. 2012; 28: 4– 6. [DOI] [PubMed] [Google Scholar]
- 4.Socialstyrelsen. ECT-treatment, a pilot study Socialstyrelsen (Artikel nr 2010-4-3). Available at: http://www.socialstyrelsen.se/publikationer2010/2010-4-3. Accessed December 1, 2010.
- 5. Frederiksen SO, D'Elia G. Electroconvulsive therapy in Sweden. Br J Psychiatry. 1979; 134: 583– 587. [DOI] [PubMed] [Google Scholar]
- 6. Nordanskog P, Nordenskjold A. Kliniska riktlinjer för elektrokonvulsiv terapi. Gothia Fortbildning AB: 2014. [Google Scholar]
- 7. Sienaert P, Dierick M, Degraeve G, et al. Electroconvulsive therapy in Belgium: a nationwide survey on the practice of electroconvulsive therapy. J Affect Dis. 2006; 90: 67– 71. [DOI] [PubMed] [Google Scholar]
- 8. Chanpattana W. A questionnaire survey of ECT practice in Australia. J ECT. 2007; 23: 89– 92. [DOI] [PubMed] [Google Scholar]
- 9. Wood DA, Burgess PM. Epidemiological analysis of electroconvulsive therapy in Victoria, Australia. Aust N Z J Psychiatry. 2003; 37: 307– 311. [DOI] [PubMed] [Google Scholar]
- 10. Kuzman MR, Pranjkovic T, Degmecic D, et al. Electroconvulsive therapy in Croatia. J ECT. 2014; 30: e42– e43. [DOI] [PubMed] [Google Scholar]
- 11. Olekseev A, Ungvari GS, Gazdag G. Electroconvulsive therapy practice in Ukraine. J ECT. 2014; 30: 216– 219. [DOI] [PubMed] [Google Scholar]
- 12. Dragasek J. Electroconvulsive therapy in Slovakia. J ECT. 2012; 28: e7– e8. [DOI] [PubMed] [Google Scholar]
- 13. Martin BA, Delva NJ, Graf P, et al. Delivery of electroconvulsive therapy in Canada: A first national survey report on usage, treatment practice, and facilities. J ECT. 2014. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 14. Schweder LJ, Lydersen S, Wahlund B, et al. Electroconvulsive therapy in Norway: rates of use, clinical characteristics, diagnoses, and attitude. J ECT. 2011; 27: 292– 295. [DOI] [PubMed] [Google Scholar]
- 15. Loh N, Nickl-Jockschat T, Sheldrick AJ, et al. Accessibility, standards and challenges of electroconvulsive therapy in Western industrialized countries: a German example. World J Biol Psychiatry. 2013; 14: 432– 440. [DOI] [PubMed] [Google Scholar]
- 16. Case BG, Bertollo DN, Laska EM, et al. Declining use of electroconvulsive therapy in U.S. general hospitals is not restricted to unipolar depression. Biol Psychiatry. 2013; 74: e19– e20. [DOI] [PubMed] [Google Scholar]
- 17. Lookene M, Kisuro A, Maciulis V, et al. Use of electroconvulsive therapy in the Baltic states. World J Biol Psychiatry. 2014; 15: 419– 424. [DOI] [PubMed] [Google Scholar]
- 18. Kaliora SC, Braga RJ, Petrides G, et al. The practice of electroconvulsive therapy in Greece. J ECT. 2013; 29: 219– 224. [DOI] [PubMed] [Google Scholar]
- 19. Nelson AI. A national survey of electroconvulsive therapy use in the Russian Federation. J ECT. 2005; 21: 151– 157. [DOI] [PubMed] [Google Scholar]
- 20. The American Psychiatric Asssociation's task force on electroconvulsive therapy The Practice of Electroconvulsive Therapy—Recommendations for Treatment, Training, and Privileging. 2nd ed Washington D.C.: American Psychiatric Publishing; 2001. [Google Scholar]
- 21. Fink M, Taylor MA. Electroconvulsive therapy: evidence and challenges. JAMA. 2007; 298: 330– 332. [DOI] [PubMed] [Google Scholar]
- 22. The UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis. Lancet. 2003; 361: 799– 808. [DOI] [PubMed] [Google Scholar]
- 23. Kho KH, van Vreeswijk MF, Simpson S, et al. A meta-analysis of electroconvulsive therapy efficacy in depression. J ECT. 2003; 19: 139– 147. [DOI] [PubMed] [Google Scholar]
- 24. Nordenskjold A, von Knorring L, Engstrom I. Predictors of the short-term responder rate of electroconvulsive therapy in depressive disorders—A population based study. BMC Psychiatry. 2012; 12: 115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Fink M. Rediscovering catatonia: the biography of a treatable syndrome. Acta Psychiatr Scand Suppl. 2013; 441: 1– 47. [DOI] [PubMed] [Google Scholar]
- 26. Koolschijn PC, van Haren NE, Lensvelt-Mulders GJ, et al. Brain volume abnormalities in major depressive disorder: a meta-analysis of magnetic resonance imaging studies. Hum Brain Mapping. 2009; 30: 3719– 3735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. MacQueen GM, Campbell S, McEwen BS, et al. Course of illness, hippocampal function, and hippocampal volume in major depression. Proc Natl Acad Sci U S A. 2003; 100: 1387– 1392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Sheline YI, Sanghavi M, Mintun MA, et al. Depression duration but not age predicts hippocampal volume loss in medically healthy women with recurrent major depression. J Neurosci. 1999; 19: 5034– 5043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Sheline YI, Gado MH, Kraemer HC. Untreated depression and hippocampal volume loss. Am J Psychiatry. 2003; 160: 1516– 1518. [DOI] [PubMed] [Google Scholar]