

Abstract
Background
Although the parent–adolescent relationship has been studied intensely, predictors and consequences of changes in the quality of the relationship across time have not been examined.
Objectives
This study examined the role of parent depression on changes in the parent–adolescent relationship, defined as support and conflict, and subsequent effects of relationship change on adolescent psychosocial outcomes including risky behavior, substance use, depressive symptoms, and hopelessness.
Method
Using data from a large prevention study, the sample included 110 youth at risk for high school drop out from the control condition; the sample was 48.2% of female, with a mean age of 15.9 years. The data, gathered from adolescents and their parents across a period of approximately 18 months, were analyzed using growth mixture modeling.
Results
Three distinct trajectories for parent–adolescent conflict (high-decreasing, low-increasing, low-stable trajectory) were identified as well as a single growth model for support, which revealed a slight decline in support across time. Parent depression was a significant predictor of perceived support, but not of membership in trajectories of conflict. Low parent–adolescent support was associated with adolescent depression and hopelessness measured 18 months post-baseline. Adolescents in the low but increasing conflict trajectory and those having a parent with depression reported increased depression and hopelessness 18 months later.
Discussion
Parent–Adolescent support and conflict were associated with adolescent emotional outcomes, particularly depression and hopelessness. The findings provide evidence that will inform prevention strategies to facilitate parent–adolescent support, minimize the negative impact of relationship conflict, and thereby promote healthy psychosocial outcomes for at-risk adolescence.
The high prevalence rates of adolescent risky behaviors and emotional problems among U.S. adolescents highlight the need for investigations to examine the antecedents and correlates as well as consequences of the developmental underpinnings. Although the parent–adolescent relationship has received research attention, this relationship has not been studied well particularly in response to how changes in the parent–adolescent relationship influence adolescent developmental outcomes during adolescence among high-risk youth.
Researchers have examined associations between parent–adolescent relationship quality and adolescent risky behavior, however, only a few investigations have addressed how the parent–adolescent relationship changes across time and the influence of such changes on adolescent psychosocial developmental outcomes. Seiffge-Krenke, Overbeek, and Vermulst (2010) examined the longitudinal link between trajectories of the mother–adolescent relationship conflict (measured in terms of support and negative affect), and adolescent anxiety regarding romantic relationships. In this study 145 adolescents were followed for 9 years, with data gathered six times from 14 to 23 years of age. Three mother–adolescent relationship trajectories were identified: a ‘normative’ trajectory with high support and stable-low negative affect; an ‘increasing negative’ trajectory with below average levels of support and increasing levels of negative affect toward mother; and a ‘decreasing negative’ trajectory with low support and decreasing levels of negative affect toward mother. Overall, adolescents in the normative (high support) group reported lower anxiety about their romantic relationships than adolescents in the increasing negative and decreasing negative groups. This research demonstrated that the quality of the parent–adolescent relationship changes in terms of both support and conflict across stages of adolescence and suggested that variability in the relationship is associated with anxiety. The research suggests that different patterns of relationship quality across time are likely to be associated with other adolescent psychosocial outcomes, such as risky behavior, drug involvement, depression, and feelings of hopelessness.
In another investigation, using a 2-year longitudinal design, Noack and Puschner (1999) examined trajectories of parent–adolescent relationships and adolescent psychosocial adjustment with 208 youth. The investigators identified three trajectory groups based on parent–adolescent connectedness and adolescent perceived autonomy. In brief they found that adolescents least connected to their parents showed the highest levels of depressive mood and aggressiveness, though the differences were not statistically significant compared to the other two groups.
THE IMPACT OF PARENT DEPRESSION ON PARENT–ADOLESCENT RELATIONSHIPS
McCarty and McMahon (2003) examined the association between the mother–youth relationship, maternal depression, and youth behavioral outcomes with 224 youth in grades 5 and 6. Mothers with depressive symptoms showed poorer relationships with their children in preadolescence. Youth with poorer maternal relationships were more likely to have disruptive behavior disorders. In a study of 800 mothers, Nelson, Hammen, Brennan, and Ullman (2003) reported that criticism directed toward a youth by depressed mothers was a risk factor for disrupted adolescent friendships, social life, and academic performance. In another study, Brennan, Le Brocque, and Hammen (2003) found that parent–adolescent relationship quality served as a protective factor by reducing risk of depression among the adolescents (N = 816) of depressed mothers. Conversely, parent warmth and acceptance were associated with positive developmental outcomes, even for children with depressed mothers. Similarly, though studied less often, paternal depression has been shown to have a negative impact on the father–adolescent relationship as well as adolescent developmental outcomes, including behavior problems and depression. In a cross-sectional study of 133 families, those with depressed fathers showed increased negative interactions with their children, which were, in turn, linked to increased behavioral problems (Jacob & Johnson, 2001). Kane and Garber (2004), in a meta-analysis of 23 studies, demonstrated that paternal depression was a significant predictor of father–child conflict and child internalizing and externalizing symptoms.
In sum, diminished quality of the parent–adolescent relationship, linked to parental depression, is an important risk factor with respect to children’s problem behaviors. On the other hand, high-quality parent–youth relationships, where the mother or father is depressed, play a significant role in protecting youth from the potentially negative influences of parent depression.
The Present Study
The purpose of this study was to describe patterns of parent–adolescent relationships, defined in terms of perceived support and conflict, and to examine the antecedent influence of parent depression as well as psychosocial developmental consequences (risky behavior, drug use, depressive symptoms, and hopelessness) linked to patterns of parent–adolescent relationship quality. In an effort to circumscribe prospective prevention efforts, we focused specifically on a known and vulnerable youth population, youth at-risk for school failure/dropout. Better understanding of the needs of at-risk youth could lead to the consolidation of prevention resources and enable healthcare professionals to provide interventions that strongly align with youth needs and developmental trajectories.
METHODS
Study Design and Participants
This study was based on longitudinal data from Preventing Drug Abuse: Parents And Youth with Schools (PAYS), a longitudinal study designed to evaluate the efficacy of the PAYS intervention program (see also Hooven, Walsh, Willgerodt, & Salazar, 2011). Participants in the initial study were chosen at random from a pool of adolescents at risk for school failure or dropout, using verified sampling criteria from school performance records including poor academic performance, poor attendance, and prior dropout status. For the larger PAYS study, initial contact was made with 2,301 youth; 1,591 indicated some interest in participating. Parent(s) of interested students were also invited to participate. A total 775 youth who had written parent consent completed the baseline assessment. Of the 775 eligible, 605 were randomly assigned to one of two experimental study conditions or to the control condition, with 500 (82%) adolescents retained in the study across time.
For the current study, we analyzed data from control group subjects (n = 153). A total 110 adolescents and their parents, none of whom were exposed to the PAYS intervention were included in the analyses. Forty-three adolescents were not included due to lack of parent depression data. Analyses were based on measures gathered from the control group at baseline (BL), 5 months after baseline (BL + 5), 10 months after baseline (BL + 10), and 18 months after baseline (BL + 18). The adolescent sample was 52% male and 48% female, ranging in age from 13 to 17 years (mean age = 15.9, SD = 0.85). Forty percent of adolescents were Caucasian, 21.8% were African-American, 10% were Asian, 7.3% were Hispanic, 12.7% were mixed race/ethnicity, and 5.5% identified as ‘other.’ The majority of parent participants were female (88.2%); the mean age was 42. Approximately half of parents were Caucasian (54.5%); 73.5% had attained some college education, with 24% having earned a BA or graduate degree.
Measures
Adolescents completed the High School Questionnaire (HSQ; Eggert, Herting, & Thompson, 1995), a multi-scale instrument that measures a broad range of adolescent behaviors including risky behaviors, drug involvement, depressed affect, feelings of hopelessness, perceived relationship (support and conflict) with parents and parental depressed affect. Items were from standard scales (e.g. Center for Epidemiological Study of Depression, CES-D) or were developed earlier by the research team. Prior studies have shown that the HSQ has good reliability and validity (Eggert et al., 1995; Thompson, Eggert, & Herting, 2000; Thompson, Mazza, Herting, Randell, & Eggert, 2005). All measures described below are scales embedded in the HSQ.
Risky behavior was assessed based on responses to six items addressing the frequency of behavior during the last year. Item examples include “Get into a physical fight with someone?” and “Run away from home for a day or more?” Participants rated these statements using Likert-type response options that included: 0 (not at all); 1 (once); 2 (twice); 3 (three times); 4 (four times); 5 (five times); and 6 (six or more times). Cronbach’s alpha was .79.
Drug involvement reflected two aspects of drug use: adverse drug consequences and drug use control problems. The measure consisted of 30 items that assessed the frequency of problems and behavior due to drugs or alcohol use within the prior month. Example items include, “There were problems between me and my friends because of my using substances” and “I usually didn’t stop with just one or two drinks.” Adolescents rated the statements using Likert-type response options that included: 0 (not at all); 1 (once); 2 (2 or 3 times); 3 (about once per week); 4 (several times per week); 5 (almost every day); and 6 (every day). Cronbach’s alpha was .86 and .91.
Adolescent depression was measured using a six-item scale for adolescents based on the CES-D scale. Sample items were: “I feel depressed,” “I feel lonely,” “Nobody truly cares about me,” and “I feel sad.” Items were rated using Likert-type response options ranging from 0 (never) to 6 (almost always). Cronbach’s alpha was .76 and .80.
Hopelessness was captured using three items reflecting a general sense of hopelessness and loss of meaning: “I feel satisfied with my life (reverse scored),” “I feel hopeless about my life,” and “my life is meaningless.” Adolescents rated these items using Likert-type response options ranging from 0 (never) to 6 (always). Cronbach’s alpha was .86.
Perceived parent–adolescent support was measured using single item scales assessing adolescent’s perceived degree of support from each parent. The scale response options ranged from − 10 (low support/help) to + 10 (high support/help). Parent support was the average of mother and father support, except for single parent families where the score was based on the single parent’s rating. Parent–Adolescent support was measured three times at BL, BL + 5, and BL + 10; correlations between mother and father support at each time point were .45, .63, and .60, respectively.
Perceived parent–adolescent conflict was measured using responses to three items: “I have serious conflicts and tensions with my parents,” “things have been so bad at home that I have thought of running away,” and “my parents approve of my friends (reverse scored).” Parent–Adolescent relationship conflict was measured four times from BL through BL + 18. Cronbach’s alpha values ranged from .53 to .76 for this brief scale.
Parent depression was measured using six items from the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977). Sample items include: “I feel depressed,” “I feel sad,” “I have trouble keeping my mind on things,” and “I have trouble sleeping.” Items were rated using Likert-type response options ranging from 0 (never) to 6 (always). Cronbach’s alpha was .73.
Data Analysis
Growth mixture modeling (GMM, Mplus 6.1) was used to identify trajectories or patterns of change for perceived support and/or conflict across time. GMM creates estimates of initial average levels (of support and conflict) and average rate of change or “growth rate,” and group cases showing similar patterns across time (Schmiege, Meek, Bryan, & Petersen, 2012). Prior to analyses, missing data were determined to be completely at random (MCAR) (Tabachnick & Fidell, 2007) and subsequently managed using maximum likelihood estimation procedures to compute multiple imputations. Following a standard analytic approach, cases were included in the analysis when data for at least one time point existed (Muthen & Muthen, 2010).
To evaluate the degree to which the GMM parameter estimates fit the hypothesized model, we used several indices including the Akaike Information Criterion (AIC), Bayesian information criterion (BIC), sample size adjusted BIC (SSBIC), and entropy (Ram & Grimm, 2009). Relatively smaller values for these fit indices indicate a better fitting model (Muthen, 2004). AIC is a modification of the χ2 statistic (χ 2 - 2df), thus a lower AIC is preferable when comparing models (Kline, 2005). A low BIC value indicates a well-fitting model. Model differences of 0 to 2 BIC points provides weak evidence, 2 to 6 shows moderate evidence, 6 to 10 suggests strong evidence, and a difference larger than ten provides strong evidence, particularly for complex models (Kass & Raftery, 1995). Entropy was evaluated for values > .80. We estimated and compared models with one and up to four trajectories. The analytic approach accounted for the fact that the intervals between data collections were unequal.
Multiple linear regression and multinomial logistic regression (SPSS 17 MVA) were used to examine if parent depression was associated with membership in different trajectories defined by parent–adolescent relationship quality (support and conflict). Multiple regression was also used to examine for associations between trajectory membership and adolescent outcomes. Membership in the conflict trajectories was coded using dummy variables, with the normative group serving as the referent category. Based on the empirical literature, we controlled for demographic and potentially confounding variables—baseline adolescent age, sex, drug use, and depression—known to influence parent–adolescent relationship quality in previous studies (Branje, Hale, Frijns, & Meeus, 2010; De Goede, Branje, & Meeus, 2009; Noack & Puschner, 1999).
RESULTS
The means and standard deviations for the key variables are reported in Table 1. The heterogeneity in parent–adolescent support across time was examined first. For support, the initial model, which included the parameter estimate for slope variance, did not converge because the slope variance was negligible, that is close to zero. Thus, the slope variance was constrained to zero (Muthen, 2004) for subsequent model tests. Table 2a summarizes the model fit indices and the number of cases for each model tested. The 2-trajectory model had low entropy (<.80). The 3-trajectory model showed fit improvement based on the BIC and entropy (>.80) (Ram & Grimm, 2009), but one trajectory included only two cases, too few cases (<5%) to be considered a distinct trajectory. The single trajectory was the best fitting model (BIC = 1614.89, AIC = 1598.69, CFI/TLI =.995). The pattern revealed, in general, moderately high parent–adolescent support with minimal change in support across time.
Table 1.
Descriptive Statistics for Key Study Variables (N = 110).
| Variable/Time | Mean | (SD) |
|---|---|---|
| Risky behavior BL + 10 | 0.49 | 0.68 |
| Drug involvement BL + 10 | 0.17 | 0.31 |
| Adolescent depression BL + 10 | 1.30 | 1.09 |
| Hopelessness BL + 10 | 0.90 | 0.95 |
| Parent depression BL | 1.43 | 0.88 |
| Adolescent depression BL | 1.37 | 1.18 |
| Parent support BL | 5.14 | 4.33 |
| Parent support BL + 5 | 5.16 | 4.11 |
| Parent support BL + 10 | 5.38 | 4.38 |
| Parent conflict BL | 1.65 | 1.27 |
| Parent conflict BL + 5 | 1.31 | 1.17 |
| Parent conflict BL + 10 | 1.24 | 1.23 |
| Parent conflict BL + 18 | 1.04 | 0.96 |
Table 2.
a Growth Mixture Models and Fit Indices for Parent–Adolescent Relationship Support.
| Number of trajectories | Log- likelihood | # of parameters | BIC | BICadj | AIC | Entropy | LRT
|
Cases/
|
|---|---|---|---|---|---|---|---|---|
| p-value | group | |||||||
| 1 | −791.58 | 6 | 1614.89 | 1595.93 | 1598.69 | NA | NA | 110 |
| 2 | −783.20 | 9 | 1608.70 | 1580.26 | 1584.40 | .79 | .28 | 75 |
| 35 | ||||||||
| 3 | −769.84 | 12 | 1596.09 | 1558.17 | 1563.68 | .86 | .15 | 75 |
| 33 | ||||||||
| 2 | ||||||||
|
b Growth Mixture Models and Fit Indices for Parent–Adolescent Relationship Conflict.
| ||||||||
| Number trajectories | Log-likelihood | # of parameter | BIC | BICadj | AIC | Entropy | LRT p-value | Cases/Group |
|
| ||||||||
| 1 | −564.39 | 8 | 1166.37 | 1141.09 | 1144.77 | NA | NA | 110 |
| 2 | −550.17 | 12 | 1156.75 | 1118.83 | 1124.35 | .95 | .07 | 104 |
| 6 | ||||||||
| 3 | −536.27 | 16 | 1147.75 | 1097.19 | 1104.55 | .87 | .25 | 85 |
| 15 | ||||||||
| 10 | ||||||||
| 4 | −529.14 | 20 | 1152.30 | 1089.10 | 1098.29 | .84 | .42 | 76 |
| 15 | ||||||||
| 13 | ||||||||
| 6 | ||||||||
Note. AIC = Akaike information criterion; BIC = Bayesian Information Criteria; BICadj = sample size-adjusted BIC. LRT p-value for k-1. Lower values of AIC and BIC indicate favorable model.
Trajectories of perceived conflict were evaluated using similar analytic procedures. Table 2b summarizes model comparisons. The 3-trajectory model was the best fitting model, with the lowest BIC and AIC values, and acceptable entropy (.87). The 2-trajectory model was rejected because one trajectory included only six cases. Compared to the 3-trajectory model, the 4-trajectory model resulted in higher AIC and BIC, and the number of cases (6) in the additional trajectory was small.
Fig. 1 depicts the three conflict trajectories with lines representing the estimated means of parent–adolescent conflict across 1.5 years. Trajectory 1, or the low-increasing trajectory, represented 9% of the sample (n = 10), showed low levels of conflict at baseline that increased dramatically by five months (BL + 5) and remained high throughout the study. Trajectory 2, or the high-decreasing trajectory, represents 13.6% of the sample (n = 15). This group had high levels of conflict at baseline that decreased and remained at moderate levels. The majority of adolescents, or 77.2% of the sample (n = 85), was in the low-stable trajectory. This group reported, on average, low levels of conflict over time. For each case, trajectory membership was saved as a new categorical variable for testing if trajectory membership was linked to adolescent developmental outcomes.
Fig. 1.
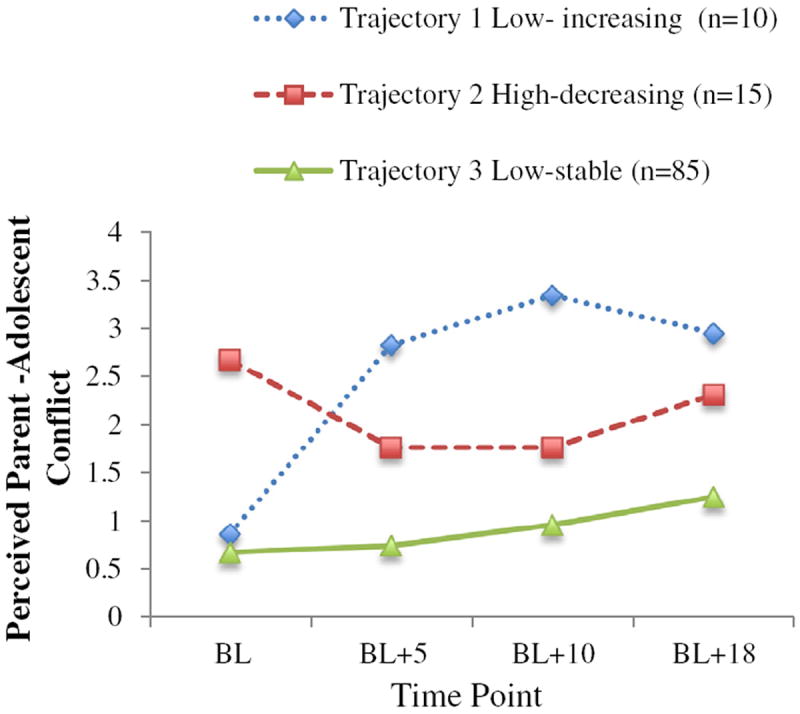
Perceived parent–adolescent conflict. This figure illustrates three trajectories of parent–adolescent relationship conflict with at-risk adolescents across a 1.5-year period. BL = baseline, BL + 5 = 5 months after baseline, BL + 10 = 10 months after baseline, and BL + 18 = 18 months after baseline. Trajectory 1 shows low levels of conflict at baseline and a sharp increase that remained high throughout the study. Trajectory 2 reflects relatively high levels of conflict throughout the study. Trajectory 3 shows low levels of conflict throughout the study.
Parent depression, demographic variables (adolescent age and sex) and potential confounding variables (adolescent depression and drug involvement at baseline) were entered simultaneously in the multiple linear regression model. The findings (Table 3) showed that parent depression (b = −0.97, p = .003) and adolescent depression (b = −1.13, p < .001) were significant and independent predictors of perceived parent–adolescent support. Adolescents with depressed affect reported less parent support as did adolescents whose parents reported symptoms of depression. Adolescent sex (b = −0.57, p = .04) was also a sig-nificant predictor: male adolescents reported less support from parents than did female adolescents. Adolescent drug involvement and age were not associated with perceived parent–adolescent support.
Table 3.
Muliple Linear Regression Examining the Influence of Baseline (T1) Predictors on Perceived Parent–Adolescent Relationship Support.
| Predictor | Multiple linear regression
|
|||||
|---|---|---|---|---|---|---|
| R2change | Fchange | R2Adj | b | (SE) | t | |
| Adolescent factors | ||||||
| Model 1 | 0.17 | 5.13 | 0.13 | |||
| Intercept | 5.35 | 0.27 | 19.57** | |||
| Age | −0.25 | 0.28 | −0.89 | |||
| Male vs. female | −0.57 | 0.28 | −2.06* | |||
| Depression BL | −1.13 | 0.28 | −3.98*** | |||
| Drug involvement BL | −0.02 | 0.28 | −0.09 | |||
| Parent factors | ||||||
| Model 1 | 0.08 | 8.97 | 0.07 | |||
| Intercept | 6.67 | 0.54 | 12.35*** | |||
| Depression BL | −0.97 | 0.32 | −3.00** | |||
Note. DI = drug involvement.
p < .10.
p < .05.
p < .01.
p < .001.
Using multinomial logistic regression, we examined for associations between parent and adolescent depression and membership in one of the three conflict trajectories. Neither adolescent nor parent depression distinguished whether adolescents were in the low-increasing conflict or the high-decreasing conflict trajectory, compared to normative trajectory (Table 4). None of the potential confounding variables was significant.
Table 4.
Baseline Predictors of Membership in Parent–Adolescent Conflict Trajectories: Parameter Estimates, Odds Ratios, and Confidence Limits for Multinomial Logistic Regression.
| Parameter | Comparison of low-increasing conflict versus low-stable conflict
|
Comparison of high-decreasing conflict versus low-stable conflict
|
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | (SE) | Wald χ2-test | Odds ratio | 95% CL for odds ratio
|
p-value | Estimate | (SE) | Wald χ2-test | Odds ratio | 95% CL for odds ratio
|
p – value | |||
| Lower | Upper | Lower | Upper | |||||||||||
| Adolescent factors BL | ||||||||||||||
| Intercept | −2.02 | (.46) | 19.26 | NA | NA | NA | <.001 | −1.86 | (.43) | 18.60 | NA | NA | NA | <.001 |
| Age | −.44 | (.36) | 1.55 | .64 | .32 | 1.29 | .21 | −.42 | (.31) | 1.78 | .66 | .36 | 1.22 | .18 |
| Male vs. female | −.48 | (.71) | .46 | .62 | .15 | .25 | .50 | .12 | (.59) | 1.30 | 1.31 | .36 | 3.58 | .84 |
| Depression | .39 | (.34) | 1.32 | 1.47 | .76 | 2.85 | .25 | −.03 | (.32) | .01 | .97 | .52 | 1.83 | .93 |
| Drug involvement | −.24 | (.46) | .28 | .79 | .32 | 1.92 | .79 | .27 | (.24) | 1.30 | 1.31 | .82 | 2.08 | .25 |
| Parent factors BL | ||||||||||||||
| Intercept | −2.22 | (.36) | 38.26 | NA | NA | NA | <.001 | −1.75 | (.29) | 37.73 | NA | NA | NA | <.001 |
| Age | −.43 | (.36) | 1.41 | .65 | .32 | 1.32 | .24 | −.29 | (.30) | .93 | .75 | .42 | 1.34 | .34 |
| Depression | −.21 | (.37) | .32 | .82 | .40 | 1.67 | .57 | .04 | (.28) | .02 | 1.04 | .60 | 1.80 | .89 |
Longitudinally, perceived parent–adolescent support predicted lower levels of adolescent depressive symptoms (b = −0.09, p = .008) and less hopelessness (b = −0.09, p = .002), but did not predict risky behavior or drug involvement (Table 5a). In examining the influence of perceived conflict, the low-stable conflict class served as the reference group. Compared to this normative group, being in the low-increasing conflict trajectory predicted adolescent depression (b = 0.97, p = .005) and hopelessness (b = 0.92, p = .02). Being a member of the low-increasing conflict trajectory was a marginally significant predictor of risky behavior (b = 0.40, p = .08). Adolescents whose parents reported more depression reported significantly increased hopelessness (b = 0.23, p = .007), and marginally significant risky behavior and depression. On the other hand, being a member of the high-decreasing conflict trajectory, compared with being a member of low-stable conflict trajectory, did not predict adolescent outcomes (Table 5b).
Table 5.
a Multiple Linear Regression Examining the Influence of Baseline Parent Depression and Relationship Support on Adolescent Outcomes.
| Variables | Regression
|
Variables | Regression
|
||||
|---|---|---|---|---|---|---|---|
| b | (SE) | t | b | (SE) | t | ||
| Risky behavior BL + 10 | Drug involvement BL + 10 | ||||||
| Support | −0.04 | 0.03 | −1.42 | Support | 0.00 | 0.01 | −0.45 |
| Parent depression BL | 0.07 | 0.07 | 1.00 | Parent depression BL | 0.00 | 0.03 | −0.03 |
| Depression BL + 10 | Hopelessness BL + 10 | ||||||
| Support | −0.09 | 0.03 | −2.64** | Support | −0.09 | 0.03 | −3.10** |
| Parent depression BL | 0.09 | 0.11 | 0.78 | Parent depression BL | 0.14 | 0.09 | 1.58 |
|
| |||||||
|
b Multiple Linear Regression Examining the Influence of Baseline Parent Depression and Relationship Conflict on Adolescent Outcomes at 10 Months After Baseline.
| |||||||
| Risky behavior BL + 10 | Drug involvement BL + 10 | ||||||
| Low-increasing class | 0.40 | 0.23 | 1.74† | Low-increasing class | −0.04 | 0.11 | −0.361 |
| High-decreasing class | 0.16 | 0.19 | 0.83 | High-decreasing class | −0.05 | 0.09 | −0.512 |
| Parent depression BL | 0.11 | 0.64 | 1.70† | Parent depression BL | 0.00 | 0.03 | 0.10 |
| Depression BL + 10 | Hopelessness BL + 10 | ||||||
| Low-increasing class | 0.97 | 0.35 | 2.79** | Low-increasing class | 0.92 | 0.30 | 3.08* |
| High-decreasing class | 0.02 | 0.29 | 0.06 | High-decreasing class | 0.37 | 0.25 | 1.474 |
| Parent depression BL | 0.18 | 0.10 | 1.76† | Parent depression BL | 0.23 | 0.09 | 2.69** |
p < .10.
p < .05.
p < .001.
p < .01.
DISCUSSION
There was no substantial change in parent–adolescent support across the three assessment periods. The overall pattern showed relatively high levels of perceived support at baseline that decreased very gradually over time. This general pattern is consistent with prior findings from cross-sectional and longitudinal studies (Loeber et al., 2000; Shanahan, McHale, Crouter, & Osgood, 2007). The findings confirm the dampening effect of adolescent depression on perceived parent–adolescent support (Branje et al., 2010), as well as the subsequent ameliorative effect of parent–adolescent support on adolescent depression.
Three distinct trajectories of parent–adolescent conflict were observed: low-increasing conflict, high-decreasing conflict; and low-stable conflict. These findings were not consistent relative to earlier studies, which have reported curvilinear and linear patterns of parent–adolescent conflict (Laursen, Coy, & Collins, 1998; Shanahan, McHale, Osgood, & Crouter, 2007). The majority of adolescents in the current study showed relatively low levels of conflict (low-stable conflict) with levels that never exceeded those of the other two trajectories. Thus, in this sample, low, incremental changes in parent–adolescent conflict in mid-adolescence were normative, which can be understood by two critical parent–adolescence developmental tasks in this transition: increasing parity between parent and adolescent and increasing independence of the youth (De Goede et al., 2009).
Parent Depression and Parent–Adolescent Relationship
Unique to this study is evidence of predictive influences of parent depression on specific patterns of both positive and negative aspects of the parent–adolescent relationship over time. Parent depression was linked to perceived support among adolescents, although the direct effects of parent depression on adolescent developmental outcomes (risky behavior, drug use, depression and hopelessness) were not significant. Empirical evidence shows that parent depression is negatively related to nurturance, warmth, and acceptance, and associated with neglectful and low responsiveness parenting, which might be experienced by adolescents as low parental support (Elgar, Mills, McGrath, Waschbusch, & Brownridge, 2007; Lovejoy, Graczyk, O’Hare, & Neuman, 2000; Luthar & Sexton, 2007).
Parent depression, on the other hand, did not predict membership in trajectories of parent–adolescent conflict, but had a significant effect on adolescent developmental outcomes. Thus, although parent depression was not linked with different patterns of conflict, parent depression influenced adolescent outcomes, suggesting that the mechanisms of influence are other than patterning of conflict in the parent–adolescent relationship. Also, although parent depression might not contribute directly to increased parent–adolescent conflict, it is associated with reductions in the frequency of parent–adolescent interactions that are fundamental to creating relationship conflict (Gross, Shaw, Burwell, & Nagin, 2009). Moreover, the use of harsh and coercive parenting, associated with parent depression (McCarty & McMahon, 2003; Snyder, 1991), may directly contribute to negative developmental outcomes for adolescents through other processes such as reduced personal competencies, dysfunctional communication, and reduction in adolescent emotional-well being.
Findings regarding the link between parent depression and adolescent emotional difficulties are particularly salient as well as consistent with knowledge that depressed parents are more likely to communicate inefficiently and to use negative parenting methods, which can lead to deficits in adolescent emotional adjustment (Elgar et al., 2007). Alternative explanations might also account for the link between parent depression and adolescent emotional maladjustment. For instance, adolescents with depressed parents might be more vulnerable to depression or other emotional problems, and parenting behavior may be only a partial contributing factor or may not be the causally contributing factor.
Adolescent Developmental Outcomes
Support and Developmental Outcomes
Parent–Adolescent support positively influenced adolescent adjustment. Adolescents with high perceived support tended to report less depression and hopelessness across time. This finding underscores other research demonstrating that support not only protects against maladjustment, but also directly enhances adolescent mental health (Ge, Natsuaki, Neiderhiser, & Reiss, 2009). Support from parents promotes the development of self-esteem, social competence, coping strategies as well as optimistic attitudes toward the future, all of which have protective and potentially moderating effects for adolescents (Aronowitz & Morrison-Beedy, 2004). Moreover, these psychosocial capacities become critical resources for adolescents who face adversity allowing for healthy adjustment regardless of the circumstances (Ge et al., 2009).
Second, an important role of parent support is to protect against negative effects of inevitable parent–adolescent conflict and/or potentially negative parenting behaviors (Crean, 2008; Sheeber, Davis, Leve, Hops, & Tildesley, 2007). In one study, which examined the association between mother’s and father’s emotional support and adolescent behavior problems among Latino youth (N = 329), parent support, in particular the mother’s support, moderated the association between parental conflict and both internalizing and externalizing problem behavior (Crean, 2008). That is, youth whose mothers were supportive were less likely to report internalizing and externalizing behaviors regardless of the amount of conflict with fathers.
Conflict and Developmental Outcomes
The current research provides an essential contribution to the field of adolescent mental health by demonstrating that variations in parent–adolescent conflict across time significantly influence adolescent developmental outcomes. While increasing parent–adolescent conflict is normative in adolescence, an abrupt increase in conflict followed by extended exposure to high levels of conflict may deter or impair adolescent psychosocial adjustment. Importantly, these findings are consistent with and supplement other research. For example, Burt, McGue, Iacono, and Krueger (2006) examine the influence of the parent–adolescent relationship on externalizing symptoms among adolescent twins (N = 974). Controlling for genetic factors, high parent–adolescent conflict was related to problematic behavior in late adolescence (Burt et al., 2006). Parent–Adolescent conflict may also inhibit the development of self-esteem, confidence, and problem solving skills. The absence of such capacities increases the likelihood of adolescent maladjustment (Shek, 1998).
Consideration of study limitations is important for interpreting the study findings. First, the study sample size was relatively small, which potentially attenuated the power to uncover the hypothesized relationships. The sample size also precluded supplemental data analyses, such as examining for potential differences in trajectories associated with gender, and investigating potential differences of maternal versus paternal depression on the evolving parent–adolescent relationship and adolescent development. Second, the study period was relatively brief to observe developmental change in the parent–adolescent relationship. Third, without an age-cohort sample, we were unable to examine for age-specific effects; age, however, controlled in all analyses, had little effect on study findings. Finally, due to data limitations, we were unable to explore for the potential influence of parent depression treatment on the parent–adolescent relationship or adolescent developmental outcomes.
Future research will need to incorporate larger, regionally or nationally representative samples as well as longitudinal designs based on age cohorts ranging from pre-adolescence through late adolescence or early adulthood. Such designs will build understanding of changes in the parent–adolescent relationship, knowledge of factors that influence changes, and the impact of relationship changes on critical adolescent developmental outcomes. In addition, larger samples will allow for examination of the relative influences of paternal versus maternal depression on the parent–adolescent relationship and developmental outcomes. With sufficiently large samples and appropriate design, researchers could examine the influence of parental depression in same vs. different gender parent–child dyads, that is mother–daughter vs. father–son dyads as well as mother–son and father–daughter.
The findings have valuable implications for both nursing practice and nursing research. Specifically, the results provide important new insights for health care professionals who work with high-risk youth in a range of settings. The results underscore the importance of understanding the impact of risks factors across the adolescent years, the need to include parents (Hooven et al., 2011), and to assess both positive and negative aspects of the parent–adolescent relationship in both treatment planning and research design. Given that the parent–adolescent relationship predicts adolescent adaptation (Brennan et al., 2003; Burt et al., 2006), the findings also point to opportunities for intervention. The finding that parent depression and adolescent depression are independently associated with the quality of the parent–adolescent relationship suggests that depressed youth and parents represent a high-risk population and that interventions should focus, in part, on strengthening their relationships. Especially relevant is the need to promote parent–adolescent support to diminish the risk of parent–adolescent relationship conflict.
This study expands knowledge about the trajectories of parent–adolescent support and conflict among at-risk adolescents, reveals how adolescent and parent factors shape these trajectories, and uncovers the influence of these trajectories on adolescent psychosocial outcomes. Notable influences were found for adolescent emotional adjustment, specifically for depression and hopelessness. The findings highlight the importance of early identification of and intervention for parents with depression. Particularly relevant for nursing practice is the identified need to promote parent–adolescent support because parent support not only reduces the risk of adolescent maladjustment, but also diminishes the risk of parent–adolescent conflict. The findings point to the need to create and study interventions that include for both parents and at-risk adolescents as a means of promoting parent–adolescent support and building relational skills to reduce conflict.
Acknowledgments
This study was funded by the Hester McLaws Nursing Scholarship from the University of Washington School of Nursing. Data for this study were drawn from a National Institutes of Health research grant (R01 DA10317) awarded to Leona L. Eggert and Brooke P. Randell (Principal Investigators) funded by the National Institute on Drug Abuse.
The authors would like to thank the adolescents and their parents who participated in the study and all Reconnecting Youth staff members who supported the PAYS research endeavor. Special appreciation goes to Drs. Jerald Herting and Elizabeth Sanders who provided statistical consultation.
Footnotes
The authors have no conflict of interest to disclose.
References
- Aronowitz T, Morrison-Beedy D. Resilience to risk-taking behaviors in impoverished African American girls: The role of mother-daughter connectedness. Research in Nursing and Health. 2004;27:29–39. doi: 10.1002/nur.20004. http://dx.doi.org/10.1002/nur.20004. [DOI] [PubMed] [Google Scholar]
- Branje SJ, Hale WW, III, Frijns T, Meeus WHJ. Longitudinal associations between perceived parent–child relationship quality and depressive symptoms in adolescence. Journal of Abnormal Child Psychology. 2010;38:751–763. doi: 10.1007/s10802-010-9401-6. http://dx.doi.org/10.1007/s10802-010-9401-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brennan PA, Le Brocque R, Hammen C. Maternal depression, parent–child relationships, and resilient outcomes in adolescence. Journal of American Academy of Child and Adolescent Psychiatry. 2003;42:1469–1477. doi: 10.1097/00004583-200312000-00014. http://dx.doi.org/10.1097/00004583-200312000-00014. [DOI] [PubMed] [Google Scholar]
- Burt SA, McGue M, Iacono WG, Krueger RF. Differential parent–child relationships and adolescent externalizing symptoms: Cross-lagged analyses within a monozygotic twin differences design. Developmental Psychology. 2006;42:1289–1298. doi: 10.1037/0012-1649.42.6.1289. http://dx.doi.org/10.1037/0012-1649.42.6.1289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crean HF. Conflict in the Latino parent-youth dyad: The role of emotional support from the opposite parent. Journal of Family Psychology. 2008;22:484–493. doi: 10.1037/0893-3200.22.3.484. http://dx.doi.org/10.1037/0893-3200.22.3.484. [DOI] [PubMed] [Google Scholar]
- De Goede IH, Branje SJ, Meeus WH. Developmental changes in adolescents’ perceptions of relationships with their parents. Journal of Youth and Adolescence. 2009;38:75–88. doi: 10.1007/s10964-008-9286-7. http://dx.doi.org/10.1007/s10964-008-9286-7. [DOI] [PubMed] [Google Scholar]
- Eggert LL, Herting JR, Thompson EA. The High School Questionnaire: Profile of experience. Seattle: University of Washington: Department of Psychosocial and Community Health; 1995. [Google Scholar]
- Elgar FJ, Mills RS, McGrath PJ, Waschbusch DA, Brownridge DA. Parent and paternal depressive symptoms and child maladjustment: The mediating role of parent behavior. Journal of Abnormal Child Psychology. 2007;35:943–955. doi: 10.1007/s10802-007-9145-0. http://dx.doi. org/10.1007/s10802-007-9145-0. [DOI] [PubMed] [Google Scholar]
- Ge X, Natsuaki MN, Neiderhiser JM, Reiss D. The longitudinal effects of stressful life events on adolescent depression are buffered by parent–child support. Development and Psychopathology. 2009;21:621–635. doi: 10.1017/S0954579409000339. http://dx.doi.org/10.1017/S0954579409000339. [DOI] [PubMed] [Google Scholar]
- Gross HE, Shaw DS, Burwell RA, Nagin DS. Transactional processes in child disruptive behavior and maternal depression: A longitudinal study from early childhood to adolescence. Development and Psychopathology. 2009;21:139–156. doi: 10.1017/S0954579409000091. http://dx.doi.org/10.1017/S0954579409000091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hooven C, Walsh E, Willgerodt M, Salazar A. Increasing participation in prevention research: Strategies for youths, parents, and schools. Journal of Child and Adolescent Psychiatric Nursing. 2011;24:137–149. doi: 10.1111/j.1744-6171.2011.00288.x. http://dx.doi.org/10.1111/j.1744-6171.2011.00288.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacob T, Johnson SL. Sequential interactions in the parent–child communications of depressed fathers and depressed mothers. Journal of Family Psychology. 2001;15:38–52. http://dx.doi.org/10.1037/0893-3200.15.1.38. [PubMed] [Google Scholar]
- Kane P, Garber J. The relations among depression in fathers, children’s psycho-pathology, and father-child conflict: A meta-analysis. Clinical Psychology Review. 2004;24:339–360. doi: 10.1016/j.cpr.2004.03.004. http://dx.doi.org/10.1016/j.cpr.2004.03.004. [DOI] [PubMed] [Google Scholar]
- Kass RE, Raftery AE. Bayes factors. Journal of the American Statistical Association. 1995;90:773–795. http://dx.doi.org/10.1080/01621459.1995.10476572. [Google Scholar]
- Kline RB. Principles and practice of structural equation modeling. 2. New York, NY: The Guilford Press; 2005. [Google Scholar]
- Laursen B, Coy KC, Collins WA. Reconsidering changes in parent–child conflict across adolescence: A meta-analysis. Child Development. 1998;69:817–832. http://dx.doi.org/10.1111/j.1467-8624.1998.tb06245.x. [PMC free article] [PubMed] [Google Scholar]
- Loeber R, Drinkwater M, Yin Y, Anderson SJ, Schmidt LC, Crawford A. Stability of family interaction from ages 6 to 18. Journal of Abnormal Child Psychology. 2000;28:353–369. doi: 10.1023/a:1005169026208. http://dx.doi.org/10.1023/a:1005169026208. [DOI] [PubMed] [Google Scholar]
- Lovejoy MC, Graczyk PA, O’Hare E, Neuman G. Parent depression and parenting behavior: A meta-analytic review. Clinical Psychology Review. 2000;20:561–592. doi: 10.1016/s0272-7358(98)00100-7. http://dx.doi.org/10.1016/S0272-7358(98)00100-7. [DOI] [PubMed] [Google Scholar]
- Luthar SS, Sexton CC. Maternal drug abuse versus maternal depression: Vulnerability and resilience among school-age and adolescent offspring. Development and Psychopathology. 2007;19:205–225. doi: 10.1017/S0954579407070113. http://dx.doi.org/10.1017/S0954579407070113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCarty CA, McMahon RJ. Mediators of the relation between parent depressive symptoms and child internalizing and disruptive behavior disorders. Journal of Family Psychology. 2003;17:545–556. doi: 10.1037/0893-3200.17.4.545. http://dx.doi.org/10.1037/0893-3200.17.4.545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthen B. Latent variable analysis: Growth mixture modeling and related technique for longitudinal data. In: Kaplan D, editor. Handbook of quantitative methodology for the social science. Newbury Park, CA: Sage Publications; 2004. pp. 345–368. [Google Scholar]
- Muthen LK, Muthen BO. Mplus user’s guide. 6. Los Angeles, CA: Muthen & Muthen; 2010. [Google Scholar]
- Nelson DR, Hammen C, Brennan PA, Ullman JB. The impact of parent depression on adolescent adjustment: The role of expressed emotion. Journal of Consulting and Clinical Psychology. 2003;71:935–944. doi: 10.1037/0022-006X.71.5.935. http://dx.doi.org/10.1037/0022-006X.71.5.935. [DOI] [PubMed] [Google Scholar]
- Noack P, Puschner B. Differential trajectories of parent–child relationships and psychosocial adjustment in adolescents. Journal of Adolescence. 1999;22:795–804. doi: 10.1006/jado.1999.0270. http://dx.doi.org/10.1006/jado.1999.0270. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Pychological Measurement. 1977;1:385–401. http://dx.doi.org/10.1177/014662167700100306. [Google Scholar]
- Ram N, Grimm KJ. Methods and measures: Growth mixture modeling: A method for identifying differences in longitudinal change among unobserved groups. International Journal of Behavioral Development. 2009;33:565–576. doi: 10.1177/0165025409343765. http://dx.doi.org/10.1177/0165025409343765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmiege SJ, Meek P, Bryan AD, Petersen H. Latent variable mixture modeling: A flexible statistical approach for identifying and classifying heterogeneity. Nursing Research. 2012;61:204–212. doi: 10.1097/NNR.0b013e3182539f4c. http://dx.doi.org/10.1097/NNR.0b013e3182539f4c. [DOI] [PubMed] [Google Scholar]
- Seiffge-Krenke I, Overbeek G, Vermulst A. Parent–Child relationship trajectories during adolescence: Longitudinal associations with romantic outcomes in emerging adulthood. Journal of Adolescence. 2010;33:159–171. doi: 10.1016/j.adolescence.2009.04.001. http://dx.doi.org/10.1016/j.adolescence.2009.04.001. [DOI] [PubMed] [Google Scholar]
- Shanahan L, McHale SM, Crouter AC, Osgood DW. Warmth with mothers and fathers from middle childhood to late adolescence: Within- and between-families comparisons. Developmental Psychology. 2007a;43:551–563. doi: 10.1037/0012-1649.43.3.551. http://dx.doi.org/10.1037/0012-1649.43.3.551. [DOI] [PubMed] [Google Scholar]
- Shanahan L, McHale SM, Osgood DW, Crouter AC. Conflict frequency with mothers and fathers from middle childhood to late adolescence: Within- and between-families comparisons. Developmental Psychology. 2007b;43:539–550. doi: 10.1037/0012-1649.43.3.539. http://dx.doi.org/10.1037/0012-1649.43.3.539. [DOI] [PubMed] [Google Scholar]
- Sheeber LB, Davis B, Leve C, Hops H, Tildesley E. Adolescents’ relationships with their mothers and fathers: Associations with depressive disorder and subdiagnostic symptomatology. Journal of Abnormal Psychology. 2007;116:144–154. doi: 10.1037/0021-843X.116.1.144. http://dx.doi.org/10.1037/0021-843X.116.1.144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shek DT. A longitudinal study of the relations between parent-adolescent conflict and adolescent psychological well-being. The Journal of Genetic Psychology. 1998;159:53–67. doi: 10.1080/00221329809596134. http://dx.doi.org/10.1080/00221329809596134. [DOI] [PubMed] [Google Scholar]
- Snyder J. Discpline as a mediator of the impact of maternal stress and mood on child conduct problems. Development and Psychopathology. 1991;3:263–276. http://dx.doi.org/10.1017/S0954579400005307. [Google Scholar]
- Tabachnick BG, Fidell LS. Using multivariate statistics. 5. Upper Saddle River, NJ: Pearson Education; 2007. [Google Scholar]
- Thompson EA, Eggert LL, Herting JR. Mediating effects of an indicated prevention program for reducing youth depression and suicide risk behaviors. Suicide & Life-Threatening Behavior. 2000;30:252–271. http://dx.doi.org/10.1111/j.1943-278X.2000.tb00990.x. [PubMed] [Google Scholar]
- Thompson EA, Mazza JJ, Herting JR, Randell BP, Eggert LL. The mediating roles of anxiety depression, and hopelessness on adolescent suicidal behaviors. Suicide & Life-Threatening Behavior. 2005;35:14–34. doi: 10.1521/suli.35.1.14.59266. http://dx.doi.org/10.1521/suli.35.1.14.59266. [DOI] [PubMed] [Google Scholar]