

Echocardiographic assessment of myocardial function is frequently used for perioperative management of surgical and critically ill patients. However, the most common echocardiographic measure, left ventricular ejection fraction (LVEF), only assesses volume-based changes during systole and diastole, rather than measuring myocardial muscle contraction. LVEF is also limited by its reliance on geometric assumptions that are subject to measurement error. Furthermore, echocardiographic assessment of regional wall motion abnormalities is limited by subjective interpretation.1 In patients with sepsis up to two-thirds of whom may experience myocardial impairment,2,3 early myocardial dysfunction may be masked by sepsis-induced vasodilation and reduced afterload and thus LVEF may not fully assess myocardial function.3,4 A more objective, sensitive, and reproducible measure of myocardial function would be useful.
Myocardial deformation imaging has been used in research for more than a decade, but clinical use of this modality is relatively new for anesthesiologists.5 This echocardiographic technique assesses the change in ventricular shape (deformation) during myocardial contraction. During systole, the myocardium shortens in the longitudinal and circumferential dimension while thickening radially. Measures of myocardial deformation include strain, defined as the percent change in length of a myocardial segment relative to its resting length, and strain rate, which is the rate of this deformation. Myocardial shortening in the longitudinal and circumferential direction is reported as a negative number, while elongation or thickening in the radial direction is positive (Figure 1). Although normal reference values have not yet been established, longitudinal strain in healthy individuals by transthoracic echocardiography is typically between −18 and −21%,5–7 while strain rate is −1.1 ± 0.2 sec−1.5,6 Describing a change in myocardial function with negative strain values can cause confusion; thus, the absolute value is considered when determining whether strain increases or decreases;8 for example, a change from −15 to −12% in longitudinal strain describes a decrease in longitudinal shortening and is referred to as a decrease in strain.
Figure 1.
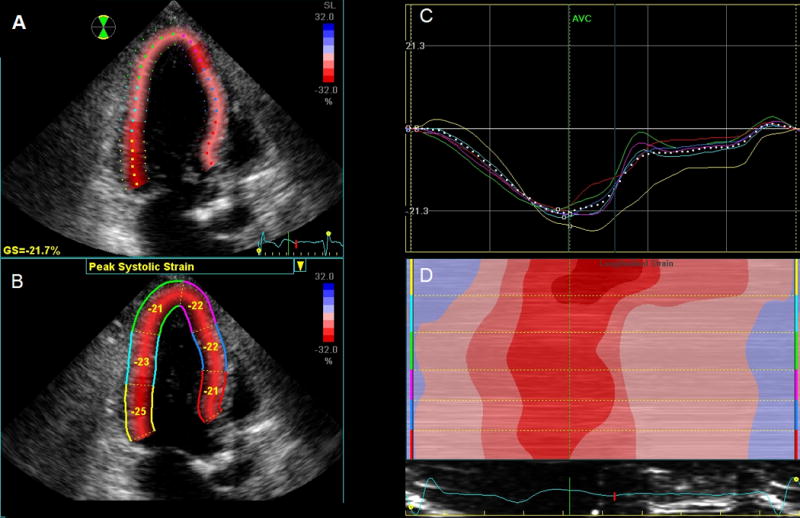
This bright and colorful demonstration of a typical left ventricular (LV) strain analysis from a transthoracic apical long-axis view using speckle tracking echocardiography looks like fun and games! A) Proper tracking of the LV demonstrating normal global strain (GS) of −21.7%. B) The myocardium is divided into 6 color-coded segments where each segment is labeled with percent regional strain. C) Strain curves for each myocardial segment (which correspond to color-coded myocardial segments in panels A and B) demonstrate myocardial shortening (negative curves) during systole peaking at aortic valve closure (AVC). D) Color M-mode display of the LV (segments are color-coded at the left edge to correspond to myocardial segments in panels A, B, and C), which demonstrates myocardial deformation over time according to the red-to-blue scale in panels A and B.
Myocardial deformation imaging was initially based on tissue Doppler echocardiography, but angle-dependence and cumbersome analysis techniques impeded its use. Subsequent development of speckle tracking echocardiography, which assesses changes in the ultrasound backscatter speckle pattern within B-mode echocardiographic images, has overcome these limitations and is more robust than Doppler-based methods.5,9 Speckle tracking echocardiography provides semiobjective, quantitative, angle-independent global and regional measurements and allows assessment of two orthogonal planes simultaneously. Improved software analysis programs have increased ease of use and the clinical application of myocardial deformation imaging with speckle tracking echocardiography.
In this issue of Anesthesia & Analgesia, Shahul and colleagues10 used myocardial deformation imaging to advance our understanding of sepsis-induced myocardial dysfunction. Myocardial function was assessed in patients with septic shock and those with sepsis alone using longitudinal, circumferential, and radial strain as well as LVEF on admission and 24 hours later. The authors reported that longitudinal strain decreased in patients with septic shock but not sepsis alone, and that LVEF, cirumferential and radial strain were not changed.
Shahul and colleagues10 should be commended for using this advanced echocardiographic technique to investigate myocardial impairment in patients with sepsis and septic shock. Several strengths of this investigation include the collection of prospective echocardiographic data and blinding of the echocardiographic analysis to timing (0 vs. 24 hours) and diagnosis (sepsis vs. septic shock). Because strain is a load-dependent measure, the authors adjusted strain measurements for left ventricular end-diastolic volume and vasopressor use and demonstrated consistent results to further support their conclusions. Unlike longitudinal strain, Shahul et al. found that circumferential and radial strain remained unchanged. However, longitudinal strain has higher reliability and reproducibility than circumferential or radial strain11 and is a more clinically useful prognostic indicator. As an example, longitudinal strain is a better predictor of mortality than LVEF in patients with valvular heart disease, heart failure, and ischemic cardiomyopathy.12–14 Although the decrease in longitudinal strain was only seen in patients with septic shock, it is interesting to note that the mean baseline longitudinal strain was abnormal in both groups (approximately −15%) even though LVEF was normal.
An important aspect of this report by Shahul and colleagues10 is that patients who had a decline in longitudinal strain were also more severely ill, as documented by higher APACHE II and SOFA scores, a greater requirement for mechanical ventilation, and higher mortality. In contrast, conventional echocardiography has not identified an association between severity of illness and worsening myocardial function, possibly because LVEF is insensitive to subtle myocardial dysfunction. This investigation also provides evidence that myocardial deformation imaging with speckle tracking echocardiography offers an early indication of worsening myocardial function before conventional measures of contractility, which may lead to earlier therapeutic intervention. Certainly, myocardial strain imaging detects early signs of myocardial dysfunction in patients with aortic regurgitation15 and those receiving cancer chemotherapy.16 Shahul et al.10 make a case for applying echocardiographic strain measurement more broadly to assess myocardial function during other critical illnesses and the perioperative period.
The authors describe several methodologic limitations to this investigation, such as the potential for confounding by patient co-morbidities. Because of the small sample size limited to a single institution, these results may not be widely generalizable and require confirmation in a larger patient population. The analysis did not correct for multiple comparisons, but the actual P-value for longitudinal strain was highly significant (P < 0.0001) reducing risk of a Type I error. This investigation cannot prove that the effects of septic shock on myocardial performance occurred early after shock onset because other time periods were not investigated. It is also important to note that a change in myocardial function between hospital admission and 24 hours later reflects not only severity of disease but also response to treatment given during this time period. Evidence supports measurement of global peak systolic strain from a single apical 4-chamber view, though with wide limits of agreement.17 Thus, analysis of the usual 3 apical views could improve accuracy of the data. Shahul and colleagues previously reported excellent intra- and interobserver reliability in strain analysis18 and including a similar result would be useful since this measurement is unfamiliar to many readers.
What’s next? This investigation provides a strong rationale for further investigation to examine myocardial function in septic patients. Future studies are needed to elucidate the cause or mechanism of septic shock-associated myocardial dysfunction and to determine whether this condition is reversible. The clinical impact of sepsis-induced attenuation of longitudinal strain on long-term outcomes as well as evaluation of potential therapies to improve myocardial function in patients who are critically ill needs to be explored.
This investigation and others will likely increase the use of strain analysis with speckle tracking echocardiography in clinical care and research investigations. Significant challenges, however, currently hinder its widespread use. Strain and strain rate are load-dependent measures of myocardial function and thus cannot explicitly state whether contractile function is impaired or whether observed changes in strain are a consequence of altered loading conditions. Speckle tracking also requires images with excellent endocardial definition, which can be challenging in critically ill or surgical patients. Further, because adequate training and experience is needed, the potential for misinterpretation, especially by a novice user, is high. Though improvements have been made in recent software programs to simplify strain analysis, these techniques are still relatively cumbersome and challenging to perform when caring for a critically ill patient in the intensive care unit or operating room. Moreover, standardization between echocardiographic workstations and software analysis packages is in progress, but more work remains.8
Despite the limitations of strain analysis, the ability to measure regional and global myocardial function using a semiobjective, quantitative, and reproducible method provides new opportunities to improve our understanding of myocardial impairment resulting from sepsis and other critical illnesses. Ultimately, strain analysis with speckle tracking echocardiography may arise as the superior technique for assessing myocardial function – more than just fun and games.
Acknowledgments
Funding: Andra Duncan, M.D., M.S. receives funding from NIH HL093065.
Footnotes
The authors declare no conflicts of interest.
Disclosures
Name: Andra E. Duncan, M.D., M.S.
Contribution: This author prepared the manuscript.
Attestation: Dr. Andra Duncan approved the final manuscript.
This manuscript will be handled by: Avery Tung, MD
Reprints will not be available from the authors.
References
- 1.Bergquist BD, Leung JM, Bellows WH. Transesophageal echocardiography in myocardial revascularization: I. Accuracy of intraoperative real-time interpretation. Anesth Analg. 1996;82:1132–8. doi: 10.1097/00000539-199606000-00006. [DOI] [PubMed] [Google Scholar]
- 2.Pulido JN, Afessa B, Masaki M, Yuasa T, Gillespie S, Herasevich V, Brown DR, Oh JK. Clinical spectrum, frequency, and significance of myocardial dysfunction in severe sepsis and septic shock. Mayo Clin Proc. 2012;87:620–8. doi: 10.1016/j.mayocp.2012.01.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Vieillard-Baron A, Caille V, Charron C, Belliard G, Page B, Jardin F. Actual incidence of global left ventricular hypokinesia in adult septic shock. Crit Care Med. 2008;36:1701–6. doi: 10.1097/CCM.0b013e318174db05. [DOI] [PubMed] [Google Scholar]
- 4.Furian T, Aguiar C, Prado K, Ribeiro RV, Becker L, Martinelli N, Clausell N, Rohde LE, Biolo A. Ventricular dysfunction and dilation in severe sepsis and septic shock: relation to endothelial function and mortality. J Crit Care. 2012;27:319 e9–15. doi: 10.1016/j.jcrc.2011.06.017. [DOI] [PubMed] [Google Scholar]
- 5.Duncan AE, Alfirevic A, Sessler DI, Popovic ZB, Thomas JD. Perioperative assessment of myocardial deformation. Anesth Analg. 2014;118:525–44. doi: 10.1213/ANE.0000000000000088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Marwick TH, Leano RL, Brown J, Sun JP, Hoffmann R, Lysyansky P, Becker M, Thomas JD. Myocardial strain measurement with 2-dimensional speckle-tracking echocardiography: definition of normal range. JACC Cardiovasc Imaging. 2009;2:80–4. doi: 10.1016/j.jcmg.2007.12.007. [DOI] [PubMed] [Google Scholar]
- 7.Yingchoncharoen T, Agarwal S, Popovic ZB, Marwick TH. Normal ranges of left ventricular strain: a meta-analysis. J Am Soc Echocardiogr. 2013;26:185–91. doi: 10.1016/j.echo.2012.10.008. [DOI] [PubMed] [Google Scholar]
- 8.Voigt JU, Pedrizzetti G, Lysyansky P, Marwick TH, Houle H, Baumann R, Pedri S, Ito Y, Abe Y, Metz S, Song JH, Hamilton J, Sengupta PP, Kolias TJ, d’Hooge J, Aurigemma GP, Thomas JD, Badano LP. Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. J Am Soc Echocardiogr. 2015;28:183–93. doi: 10.1016/j.echo.2014.11.003. [DOI] [PubMed] [Google Scholar]
- 9.Amundsen BH, Helle-Valle T, Edvardsen T, Torp H, Crosby J, Lyseggen E, Støylen A, Ihlen H, Lima JA, Smiseth OA, Slørdahl SA. Noninvasive myocardial strain measurement by speckle tracking echocardiography: Validation against sonomicrometry and tagged magnetic resonance imaging. J Am Coll Cardiol. 2006;47:789–93. doi: 10.1016/j.jacc.2005.10.040. [DOI] [PubMed] [Google Scholar]
- 10.Shahul S, Gulati G, Hacker MR, Mahmood F, Canelli R, Nizamuddin J, Mahmood B, Simon BA, Novack V, Talmor D. Detection of myocardial dysfunction in septic shock: A speckle tracking echocardiography study. Anesth Analg. doi: 10.1213/ANE.0000000000000943. IN THIS ISSUE. [DOI] [PubMed] [Google Scholar]
- 11.Risum N, Ali S, Olsen NT, Jons C, Khouri MG, Lauridsen TK, Samad Z, Velazquez EJ, Sogaard P, Kisslo J. Variability of global left ventricular deformation analysis using vendor dependent and independent two-dimensional speckle-tracking software in adults. J Am Soc Echocardiogr. 2012;25:1195–203. doi: 10.1016/j.echo.2012.08.007. [DOI] [PubMed] [Google Scholar]
- 12.Dahl JS, Videbæk L, Poulsen MK, Rudbæk TR, Pellikka PA, Møller JE. Global Strain in Severe Aortic Valve Stenosis: Relation to Clinical Outcome After Aortic Valve Replacement. Circulation: Cardiovascular Imaging. 2012;5:613–620. doi: 10.1161/CIRCIMAGING.112.973834. [DOI] [PubMed] [Google Scholar]
- 13.Mignot A, Donal E, Zaroui A, Reant P, Salem A, Hamon C, Monzy S, Roudaut R, Habib G, Lafitte S. Global longitudinal strain as a major predictor of cardiac events in patients with depressed left ventricular function: a multicenter study. J Am Soc Echocardiogr. 2010;23:1019–24. doi: 10.1016/j.echo.2010.07.019. [DOI] [PubMed] [Google Scholar]
- 14.Bertini M, Ng ACT, Antoni ML, Nucifora G, Ewe SH, Auger D, Marsan NA, Schalij MJ, Bax JJ, Delgado V. Global longitudinal strain predicts long-term survival in patients with chronic ischemic cardiomyopathy. Circulation: Cardiovascular Imaging. 2012;5:383–391. doi: 10.1161/CIRCIMAGING.111.970434. [DOI] [PubMed] [Google Scholar]
- 15.Marciniak A, Sutherland GR, Marciniak M, Claus P, Bijnens B, Jahangiri M. Myocardial deformation abnormalities in patients with aortic regurgitation: A strain rate imaging study. Eur J Echocardiogr. 2009;10:112–9. doi: 10.1093/ejechocard/jen185. [DOI] [PubMed] [Google Scholar]
- 16.Thavendiranathan P, Poulin F, Lim KD, Plana JC, Woo A, Marwick TH. Use of myocardial strain imaging by echocardiography for the early detection of cardiotoxicity in patients during and after cancer chemotherapy: a systematic review. J Am Coll Cardiol. 2014;63:2751–68. doi: 10.1016/j.jacc.2014.01.073. [DOI] [PubMed] [Google Scholar]
- 17.Bagger T, Sloth E, Jakobsen CJ. Left ventricular longitudinal function assessed by speckle tracking ultrasound from a single apical imaging plane. Crit Care Res Pract. 2012;2012:361824. doi: 10.1155/2012/361824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Shahul S, Rhee J, Hacker MR, Gulati G, Mitchell JD, Hess P, Mahmood F, Arany Z, Rana S, Talmor D. Subclinical left ventricular dysfunction in preeclamptic women with preserved left ventricular ejection fraction: a 2D speckle-tracking imaging study. Circ Cardiovasc Imaging. 2012;5:734–9. doi: 10.1161/CIRCIMAGING.112.973818. [DOI] [PMC free article] [PubMed] [Google Scholar]