

Abstract
AIM: CT virtual endoscopy has been used in the study of various organs of body including the biliary tract, however, CT virtual endoseopy in diagnosis of gallbladder polyps has not yet been reported. This study was to evaluate the diagnostic value of CT virtual endoscopy in polyps of the gallbladder.
METHODS: Thirty-two cases of gallbladder polyps were examined by CT virtual endoscopy, ultrasound, CT scan with oral biliary contrast separately and confirmed by operation and pathology. CT biliary cystoscopic findings were analyzed and compared with those of ultrasound and CT scan with oral biliary contrast, and evaluated in comparison with operative and pathologic findings in all cases.
RESULTS: The detection rate of gallbladder polyps was 93.8%(90/96), 96.9%(93/96) and 79.2%(76/96) for CT cystoscopy, ultrasound and CT scan with oral contrast, respectively. CT biliary cystoscopy corresponded well with ultrasound as well as pathology in demonstrating the location, size and configuration of polyps. CT endoscopy was superior to ultrasound in viewing the polyps in a more precise way, 3 dimensionally from any angle in space, and showing the surface in details. CT biliary cystoscopy was also superior to CT scan with oral biliary contrast in terms of observation of the base of polyps for the presence of a pedicle, detection rates as well as image quality. The smallest polyp detected by CT biliary cystoscopy was measured 1.5 mm×2.2 mm×2.5 mm.
CONCLUSION: CT biliary cystoscopy is a non-invasive and accurate technique for diagnosis and management of gallbladder polyps.
INTRODUCTION
Since Klein et al.[1] in 1993 reported the computed tomographic cholangiography using spiral scanning and 3D image processing, many lesions of the biliary tract have been studied[2-14]. In 1994 CT virtual endoscopy (CTVE) was introduced, its application in obtaining organ images has been described extensively[15-28]. However, we have not seen any report concerning CTVE in the
diagnosis of polyps of the gallbladder. In the current paper we reported the CTVE findings of gallbladder polyps in 32 patients.
MATERIALS AND METHODS
From January 1999 to the present study, 32 patients with gallbladder polyps confirmed by operation and pathology underwent CT biliary cystoscopy (CT virtual endoscope of the gallbladder, CTVEGB). There were 18 males and 14 females (age range, 28-47 years, mean age, 35.8 years). Eight patients had vague pain in the right upper abdomen, 4 patients had colicky pain, and the remaining 20 patients were asymptomatic. All patients had normal serum bilirubin and alkaline phosphatase levels. On the day of CTVEGB, abdominal ultrasonographic studies were done for all patients.
The CT scanner was Somatom plus 4 power helical CT (Siemens, Germany) with a Virtuoso workstation (WS). The sonographic equipment was color Doppler ultrasound HDL 5 000 (ATL USA). Sixteen hours prior to CT study, each patient took 4.5 g of iopanoic acids orally and the gastrointestinal tract was properly prepared. CT scanning parameters were: 120 kV, 200-220 mA, slice thickness 2-3 mm, pitch 1-1.2 or 1.5-2.0; image reconstruction interval: 0.8-1.2 mm or 1.5-2.0 mm, FOV 214-263 mm; scan time 25-32 s, scan speed 0.75 s per 360° revolution.
Image post processing was done by Dr. Hu. The reconstructed image was transferred to virtuoso WS. “Fly” software was used to obtain 3D stereo image of the gallbladder and surrounding structures, then virtual endoscopic image of the gallbladder was proceeded simply by double click on the mouse, threshold value was adjusted so that the normal gallbladder mucosa was displayed clearly (Figure 1). The threshold value ranged from -178-251HU. Color encoding was performed using green color (color of the bile). Endoscopy was carried out from any viewpoint in the gallbladder with varying views, size, speed and angle, and detailed scrutiny was performed. It took 1 h to complete CTVEGB. All axial source CT images were interpreted as spiral CT with oral biliary contrast (OCCT) and 3D stereo images using fly software as CTVEGB, which were done by two radiologists, who were unaware of the clinical and ultrasonographic information. Another two radiologists did ultrasonographic study. All radiologists worded together in evaluating the number, size, configuration, location, surface and base of polyps of the gallbladder. A professional statistician performed all statistical analyses by using a commercially available statistical software package (SAS Institute, Cary, Nc). The results of CTVEGB, OCCT, ultrasound and pathology were compared with each other by means of the chi-square test.
Figure 1.
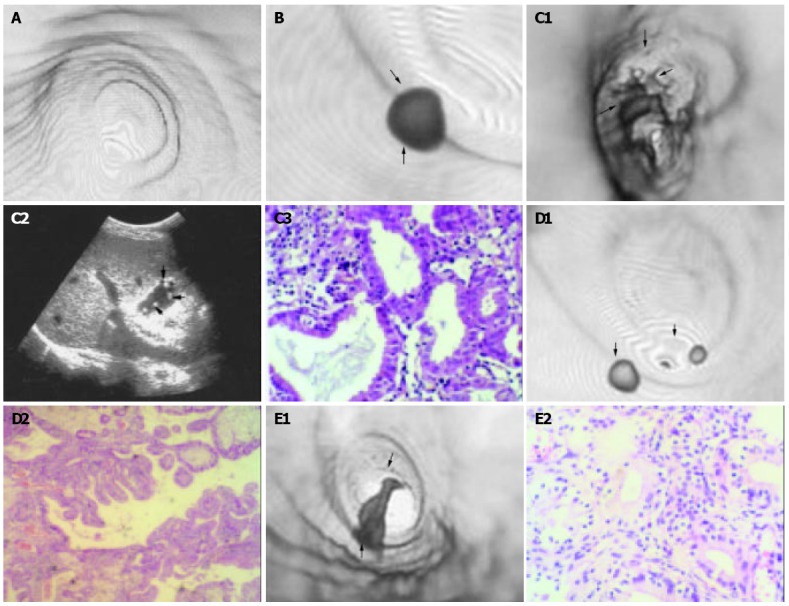
CTVEGB detection of gallbladder polyps. A: Surface detail of gallbladder displayed by CTVEGB in a 47-year old normal man. B: Smallest single cholesterol polyp (arrow head) detected by CTVEGB in a 28-year-old man. C: Multiple gallbladder polyps in a 30- year-old man. (1) Multiple polyps of cauliflower appearance and small polyps (arrow head). (2) Color ultrasonography found multiple polyps of cauliflower appearance and small polyps (arrow head). (3) Multiple polyps were inflammatory polyps on pathology (HE × 20). D: Multiple cholesterol gallbladder polyps in a 30-year-old woman. Two cholesterol polyps (arrow head) were proved by pathology (HE × 20). E: Single inflammatory gallbladder polyps in a 29-year-old woman. An irregular inflamma-tory polyp was proved by pathology (HE × 20).
RESULTS
On OCCT, the gallbladder was clearly visualized in 32 cases. The 3D stereo view clearly displayed the gallbladder and its surrounding structures such as the liver, ribs and spine on maximum intensity projection (MIP) protocol. CTVEGB images were obtained from all patients. No procedure-related adverse reaction was observed in all 32 cases.
Correlation of CTVEGB with ultrasound
The 3D image, CTVEGB image (Figure 1A) and axial source image could be displayed simultaneously on Virtuoso WS. CTVEGB could be manipulated flexibly from multiple views and various angles so that the location, size, configuration, surface and base of the polyps could be clearly shown better on CTVEGB than on ultrasound images. Among the 32 cases with gallbladder polyps, the detection rate of polyps was 96.9(93/96) by ultrasound and 93.8%(90/96) by CTVEGB. Comparison of ultrasound and CTVEGB with operative and pathologic findings is shown in Table 1. The smallest polyp detected by CTVEGB measured 1.5 mm×2.2 mm×2.5 mm (Figure 1B). One polyp with cauliflower appearance (Figure 1C) and another butterfly-like one were detected by CTVEGB, which were in accordance with ultrasound (Figure 1D) and operative findings. Pathologically both were confirmed to be inflammatory polyps of the gallbladder (Figure 1E).
Table 1.
Comparison of ultrasound and CTVEGB in 96 gallbladder polyps
| Modality | Polyps (n) | Diameter (mm) |
Location (n) |
Configuration (n) |
Base (n) peduncle |
|||||||||
| < 5 | 5-10 | 10- | Neck | Body | Base | Spherical | Papillary | Irregular | Butterfly | Cauliflower | (-) | (+) | ||
| Pathology | 96 | 54 | 30 | 12 | 24 | 64 | 8 | 81 | 7 | 6 | 1 | 1 | 58 | 38 |
| Ultrasound | 93 | 51 | 30 | 12 | 24 | 61 | 8 | 78 | 7 | 6 | 1 | 1 | 55 | 38 |
| CTVEGB | 90 | 48 | 30 | 12 | 24 | 58 | 8 | 75 | 7 | 6 | 1 | 1 | 52 | 38 |
| χ2 | 0.466 | 0.485 | 0.478 | 0.471 | 0.482 | |||||||||
| P value | > 0.05 | > 0.05 | > 0.05 | > 0.05 | > 0.05 | |||||||||
No statistical significance (P > 0.05, a = 0.05) between ultrasound and CTVEGB findings; 2. CTVEGB is abbreviation of CT virtual endoscopy of the gall bladder.
Comparison between CTVEGB and OCCT
On OCCT, the gallbladder filled with contrast medium was well visualized, the polyps appeared as filling detects of various sizes and numbers. Among the 96 polyps, OCCT detected 76 while CTVEGB detected 90, the detection rate was 79.2% and 93.8% respectively. The correlation with operative and pathologic findings is shown in Table 2. CTVEGB missed 3 polyps with a diameter < 3 mm, while OCCT missed 20 polyps with a diameter < 5 mm. The difference was statistically significant (P < 0.01, a = 0.05).
Table 2.
Comparison of OCCT and CTVEGB in 96 gallbladder polyps
| Modality | Polyps | Diameter (mm) |
Location (n) |
Configuration (n) |
Base (n) peduncle |
|||||||||
| < 5 | 5-10 | 10- | Neck | Body | Base | Spherical | Papillary | Irregular | Butterfly | Cauliflower | (-) | (+) | ||
| Pathology | 96 | 54 | 30 | 12 | 24 | 64 | 8 | 81 | 7 | 6 | 1 | 1 | 58 | 38 |
| OCCT | 76 | 34 | 30 | 12 | 24 | 44 | 8 | 61 | 7 | 6 | 1 | 1 | 52 | 24 |
| CTVEGB | 90 | 48 | 30 | 12 | 24 | 58 | 8 | 75 | 7 | 6 | 1 | 1 | 52 | 38 |
| χ2 | 7.518 | 8.561 | 8.157 | 7.743 | 14.797 | |||||||||
| P value | < 0.01 | < 0.01 | < 0.01 | < 0.01 | < 0.01 | |||||||||
1. Statistical difference between ultrasound and CTVEGB findings (P < 0.01, a = 0.05); 2. CTVEGB is abbreviation of CT virtual endoscopy of the gall bladder; 3. OCCT is abbreviation of spiral CT with oral biliary contrast.
CTVEGB and pathological classification
The incidence of polyps was related to the pathologic type. Of the 90 polyps detected by CTVEGB, 60 were cholesterol polyps, in which 12(20%) were single cholesterol polyps (Figure 1B) and 48(80%) were multiple cholesterol polyps (Figure 1D). Among the 30 inflammatory polyps, 15(50%) were single polyps (Figure 1F) and 15 were multiple types (Figure 1C). The size of gallbladder polyps was related to pathologic types. Among the 90 polyps detected by CTVEGB, 60 were cholesterol polyps, in which 38(63%) had the greatest diameter ≤ 5 mm, 22 (37%) had a diameter of 5-10 mm and 0(0%) had a diameter of ≥ 10 mm. There were 30 inflammatory polyps, 10(33%) were ≤ 5 mm, 8(27%) were 5-10 mm and 12(40%) were ≥ 10 mm. The configuration of polyps was related to pathologic types. Among the 60 cholesterol polyps, 52(87%) had a spherical configuration, 7(11%) were papillary and 1(2%) irregular in outline. Of the 30 inflammatory polyps, 23(77%) were spherical and 7(23%) were irregular and none was papillary in form. The location of gallbladder polyps was related to pathologic types. Of the cholesterol polyps, 40(67%) were located in the body of gallbladder, 19(31%) in the neck and 1(2%) in the base. Of the 30 inflammatory polyps, 18(60%) were located in the body of gallbladder, 5(17%) in the neck and 7(23%) in the base. The presence or absence of a pedicle was related to pathologic type. There were 36(60%) cholesterol polyps with a pedicle and 24(40%) devoid of a pedicle. Two (7%) inflammatory polyps were pedunculated and 28(93%) not.
DISCUSSION
A lot of techniques have been developed for studying the biliary tract. Ultrasonography, the technique of choice for studying the gallbladder, is of limited value in the evaluation of polyps of gallbladder, depending on the operator’s skill. Intravenous cholangiography is a safe technique, but does not adequately opacify the polyps of gallbladder. Conventional computed tomography (CT) is inadequate for detection of low-density lesions of the gallbladder. ERCP and PTC can provide excellent delineation of biliary anatomy and pathology, but both are invasive and associated with risks and complications. MR cholangiography is a popular noninvasive technique and has been shown to be both sensitive to and specific for visualization of various conditions of the biliary tract. Although it is safe, the technique is contraindicated in patients with aneurysm clips or cardiac pacemakers. In addition, MR cholangiography may not be suitable for patients with claustrophobia or those with multiple metallic clips, which may cause artifacts. There are few alternatives to the invasive techniques, and additional noninvasive techniques are in demand.
Spiral CT allows imaging of a volume of tissue during a single breath-hold. Axial CT data could be reconstructed into two-dimensional multi-planar or three-dimensional (3D) volume-rendered images using workstations and image-rendering software[1]. This CT technology combined with the administration of IV cholangiographic contrast agents could produce diagnostic images of the biliary tract[2-7,9,10,14], and has been used for diagnosis of obstructive biliary disease, choledochocele, choledocholithiasis and aberrance bile ducts. The main limitation of this technique is that the rate of allergic reactions and renal or hepatic toxicity (or both) are relatively
high due to by these contrast agents.
Oral cholangiographic contrast agents are a potential alternative to IV contrast agents. Unlike the later, these contrast agents had few side effects, such as diarrhea, loose stools, nausea and stinging on urination[8]. Because the patients ingested 6 g iopanoic acid before CT examination[8,11,13], the contrast agents were decreased to 4.5 g iopanoic acid. No side effect was found in our study. CT cholangiography was used to assess choledoch variants and describe choledocholithiasis[8,11,13]. To our knowledge, there have been few studies or reports in which IV cholangiograhpic contrast agents were used to diagnose gallbladder polyps[10]. It has not yet been established whether these oral contrast agents can reliably demonstrate gallbladder polyps on CTVEGB.
Some factors could influence the image quality of CTVEGB, which is important for precise diagnostic information. Usually 16 h after oral administration of 4.5 g iopanoic acid, CTVEGB could yield the image of gallbladder with a good quality. With a dose of 3.0 g, visualization of the gallbladder would be inadequate. Inadequate control of respiratory motion has adverse impact on image quality, resulting in failure to detect small lesions or ragged distortion of large lesions. Optimal image quality is achieved by single breath hold. Higher reconstruction rates such as 0.8-1.2 mm are more helpful in displaying minute lesions and the details. Higher pitch (1.5-2.0) may produce artifact-mimicking polyps or miss small lesions. Pitch 1.0-1.2 is a good choice. FOV is related to the displayed area of the surrounding structures but not to observation of the polyps. However, adequate FOV can clearly demonstrate the stereo relation of gallbladder and surrounding structures. The threshold value seriously affects effective observation of polyps. Variation of the threshold value leads to marked change in visualization of the size and appearance of polyps, therefore selecting appropriate threshold value is critical to avoid image distortion. Generally, a threshold value is selected so that the normal gallbladder mucosa is shown clearly.
Based on our clinical experience in diagnosing gallbladder polyps by CTVEGB, TVEGB can clearly display the normal anatomy of the interior of gallbladder. CTVEGB can clearly show the size, configuration, location, surface and base of gallbladder polyps in accordance with color ultrasound, operative and pathologic findings. The smallest polyp reported in this article was 1.5 mm×2.2 mm×2.5 mm. Localization of the polyps was accurate. Good depiction of polyp configuration could be obtained. In this series 12 polyps with irregular appearance were proved to be inflammatory in nature with adhesions. Detailed observation of the base of polyps to confirm the presence of a pedicle by CTVEGB was possible by viewing from different angles and in this respect, CTVEGB was superior to color ultrasound. Among the 96 polyps, CTVEGB missed 6 polyps with the diameter less than 3 mm. Color ultrasound missed 3 polyps because of adhesion with surrounding tissues. The difference, however, was not statistically significant (P>0.05). The correspondence was good. OCTT, being a safe, simple and efficient method[1-7], is capable of detecting biliary calculus, tumor, anomaly and dilatation of the biliary tract and protruding lesions with a bigger size. However, limited by the concentration of contrast medium, small polypous lesions are easily obscured and thus escaping detection by OCCT. In this series, 20 polyps with a diameter less than 5 mm were missed. OCCT is also inferior to CTVEGB in terms of observation of the base of polyps for the presence of a pedicle, detection rate as well as image quality.
In comparison of the findings of CTVEGB with pathological changes, in cholesterol polyps, multiple polyps were far more frequently seen than single polyps (80% vs 20%). While in inflammatory polyps, the incidence was 50% for each, indicating that most cholesterol polyps were multiple, while single polyp and multiple ones were equally common in inflammatory polyps. Among the cholesterol polyps, 63% were ≤ 5 mm, 37% were between 5-10 mm, none was ≥ 10 mm. While in inflammatory polyps, 33% were ≤ 5 mm, 27% was between 5-10 mm, 40% were ≥ 10 mm, indicating that smaller polyps (≤ 5 mm) were common in cholesterol polyps and bigger ones (≥ 10 mm) were common in inflammatory polyps. Among cholesterol polyps, spherical type was most common (87%), followed by papillary type (11%), then irregular type (2%). For inflammatory polyps, 77% were spherical type, 23% irregular type. There was no papillary inflammatory polyp in this series. For cholesterol polyps, 67% occurred in the body of gallbladder, 31% in the neck and 2% in the base. Whereas for inflammatory polyps, they were 60%, 23% and 17% in the body, base and neck respectively. Cholesterol polyps usually occurred in the body and neck of the gallbladder, while for inflammatory polyps usually in the body and base. Sixty percent of the cholesterol polyps were pedunculated and 40% were devoid of a pedicle. Most of the inflammatory polyps (93%) were non-pedunculated.
Footnotes
Supported by the Scientific Bureau of Shenzhen City, No. 200006012.
Edited by Zhu LH and Wang XL Proofread by Xu FM
References
- 1.Klein HM, Wein B, Truong S, Pfingsten FP, Günther RW. Computed tomographic cholangiography using spiral scanning and 3D image processing. Br J Radiol. 1993;66:762–767. doi: 10.1259/0007-1285-66-789-762. [DOI] [PubMed] [Google Scholar]
- 2.Van Beers BE, Lacrosse M, Trigaux JP, de Cannière L, De Ronde T, Pringot J. Noninvasive imaging of the biliary tree before or after laparoscopic cholecystectomy: use of three-dimensional spiral CT cholangiography. AJR Am J Roentgenol. 1994;162:1331–1335. doi: 10.2214/ajr.162.6.8191994. [DOI] [PubMed] [Google Scholar]
- 3.Fleischmann D, Ringl H, Schöfl R, Pötzi R, Kontrus M, Henk C, Bankier AA, Kettenbach J, Mostbeck GH. Three-dimensional spiral CT cholangiography in patients with suspected obstructive biliary disease: comparison with endoscopic retrograde cholangiography. Radiology. 1996;198:861–868. doi: 10.1148/radiology.198.3.8628884. [DOI] [PubMed] [Google Scholar]
- 4.Galeon M, Deprez P, Van Beers BE, Pringot J. Spiral CT cholangiography of choledochocele. J Comput Assist Tomogr. 1996;20:814–815. doi: 10.1097/00004728-199609000-00026. [DOI] [PubMed] [Google Scholar]
- 5.Stockberger SM, Sherman S, Kopecky KK. Helical CT cholangiography. Abdom Imaging. 1996;21:98–104. doi: 10.1007/s002619900024. [DOI] [PubMed] [Google Scholar]
- 6.Nascimento S, Murray W, Wilson P. Computed tomography intravenous cholangiography. Australas Radiol. 1997;41:253–261. doi: 10.1111/j.1440-1673.1997.tb00669.x. [DOI] [PubMed] [Google Scholar]
- 7.Kwon AH, Uetsuji S, Ogura T, Kamiyama Y. Spiral computed tomography scanning after intravenous infusion cholangiography for biliary duct anomalies. Am J Surg. 1997;174:396–401; discussion 401-2. [PubMed] [Google Scholar]
- 8.Chopra S, Chintapalli KN, Ramakrishna K, Rhim H, Dodd GD. Helical CT cholangiography with oral cholecystographic contrast material. Radiology. 2000;214:596–601. doi: 10.1148/radiology.214.2.r00fe47596. [DOI] [PubMed] [Google Scholar]
- 9.Takahashi M, Saida Y, Itai Y, Gunji N, Orii K, Watanabe Y. Re-evaluation of spiral CT cholangiography: basic consideration and reliability for detecting choledocholithiasis in 80 patients. J Comput Assist Tomogr. 2000;24:859–865. doi: 10.1097/00004728-200011000-00007. [DOI] [PubMed] [Google Scholar]
- 10.Hirao K, Miyazaki A, Fujimoto T, Isomoto I, Hayashi K. Evaluation of aberrant bile ducts before laparoscopic cholecystectomy: helical CT cholangiography versus MR cholangiography. AJR Am J Roentgenol. 2000;175:713–720. doi: 10.2214/ajr.175.3.1750713. [DOI] [PubMed] [Google Scholar]
- 11.Soto JA, Alvarez O, Múnera F, Velez SM, Valencia J, Ramírez N. Diagnosing bile duct stones: comparison of unenhanced helical CT, oral contrast-enhanced CT cholangiography, and MR cholangiography. AJR Am J Roentgenol. 2000;175:1127–1134. doi: 10.2214/ajr.175.4.1751127. [DOI] [PubMed] [Google Scholar]
- 12.Breen DJ, Nicholson AA. The clinical utility of spiral CT cholangiography. Clin Radiol. 2000;55:733–739. doi: 10.1053/crad.2000.0511. [DOI] [PubMed] [Google Scholar]
- 13.Caoili EM, Paulson EK, Heyneman LE, Branch MS, Eubanks WS, Nelson RC. Helical CT cholangiography with three-dimensional volume rendering using an oral biliary contrast agent: feasibility of a novel technique. AJR Am J Roentgenol. 2000;174:487–492. doi: 10.2214/ajr.174.2.1740487. [DOI] [PubMed] [Google Scholar]
- 14.Cabada Giadas T, Sarria Octavio de Toledo L, Martinez-Berganza Asensio MT, Cozcolluela Cabrejas R, Alberdi Ibanez I, Alvarez Lopez A, Garcia-Asensio S. Helical CT cholangiography in the evaluation of the biliary tract: application to the diagnosis of choledocholithiasis. Abdom Imaging. 2002;27:61–70. doi: 10.1007/s00261-001-0043-6. [DOI] [PubMed] [Google Scholar]
- 15.Sun CH, Li ZP, Yan F, Yu SP, Xu DS, Xie HB, Lin PZ. CT virtual endoscopy of intravenous cystography: experimental study and clinical application. Zhonghua Fangshexue Zazhi. 2003;37:537–541. [Google Scholar]
- 16.Wang D, Zhang WS, Xiong MH, Xu JX, Yu M, Xu CY. CT virtual endoscopy of the auditory ossicular chain and its preliminary clinical application. Zhonghua Fangshexue Zazhi. 2000;34:459–461. [Google Scholar]
- 17.Han P. CT virtual endoscopy: a study of the capability to display the structures and abnormalities in nasal cavity. Zhonghua Fangshexue Zazhi. 1999;33:7–11. doi: 10.1007/BF02887060. [DOI] [PubMed] [Google Scholar]
- 18.Xiao Y, Tian JM, Wang PJ, Zuo CJ, Wang MJ, Cui HW, Zeng H, Lu TZ, Xue H, Fan Yl. Clinical application of CT virtual endos-copy in the diagnosis of aortic diseases. Zhonghua Fangshexue Zazhi. 2000;34:540–542. [Google Scholar]
- 19.Wang D, Zhang WS, Xiong MH, Xu JX. CT virtual endoscopy of the larynx and hypo pharynx and its preliminary clinical application. Zhonghua Fangshexue Zazhi. 2000;34:548–550. [Google Scholar]
- 20.Hu CA, Hao JM, Qian ZB. Preliminary clinical experience of spi-ral CT virtual colonoscopy for detection of colorectal polyps. Zhonghua Fangshexue Zazhi. 2000;34:313–315. [Google Scholar]
- 21.Tan LL, Li YB, Li SX, Jiang JD, Liang TJ, Liu K. Application of SCTA and CTVE in diagnosing aortic dissection. Zhongguo Linchuangyixue Yingxiang Zazhi. 2002;13:190–202. [Google Scholar]
- 22.Chen F, Zheng KE, Liu WH, Ju SH, Xu QZ. Evaluation of image quality of CT virtual endoscopy. Zhonghua Fangshexue Zazhi. 2000;34:765–769. [Google Scholar]
- 23.Zhang LQ, Zhang J, Zhong GC. Application of CT virtual endoscopy to diseases of digestive system. Shiyong Yiji Zazhi. 2002;9:33–34. [Google Scholar]
- 24.Xie BJ, Zheng XH, Li KX, Wan JH, Wu ZY. Anatomy structures of nasal cavity and paranasal sinus on virtual endoscopy and coronal image. Linchuang Erbihouke Zazhi. 2001;15:483–485. [PubMed] [Google Scholar]
- 25.Xu XJ, Huang G, Gou Q, Ren XS. Clinical applications of multislice helic CT virtual gastroscopy and three-dimensional imaging in gastric tumors. Shiyong Fangshexue Zazhi. 2002;18:475–878. [Google Scholar]
- 26.Ding GQ, Li XD, Yu DM, Zhang QW, Rui XF, Zhang DH, Li GH. Clinical applications of virtual endoscopy based on spiral CT scan in bladder neoplasm. Linchang Chaoshengxue Zazhi. 2002;17:656–658. [Google Scholar]
- 27.Liewald F, Lang G, Fleiter T, Sokiranski R, Halter G, Orend KH. Comparison of virtual and fiberoptic bronchoscopy. Thorac Cardiovasc Surg. 1998;46:361–364. doi: 10.1055/s-2007-1010254. [DOI] [PubMed] [Google Scholar]
- 28.Han P, Pirsig W, Ilgen F, Gorich J, Sokiranski R. Virtual endos-copy of the nasal cavity in comparison with fiberoptic endoscopy. Eur Arch Otorhinolaryngol. 2000;257:578–583. doi: 10.1007/s004050000284. [DOI] [PubMed] [Google Scholar]