

Abstract
The diagnosis and staging of various gastrointestinal malignancies have been made possible with the use of endoscopic ultrasound, which is a relatively safe procedure. The field of endoscopic ultrasound is fast expanding due to advancements in therapeutic endoscopic ultrasound. Though various studies have established its role in gastrointestinal malignancies and pancreatic conditions, its potential in the field of hepatic lesions still remains vastly untapped. In this paper the authors attempt to review important and landmark trials, case series and case studies involving hepatic applications of endoscopic ultrasound, thus not only providing an overview of utilization of endoscopic ultrasound in various liver conditions but also speculating its future role.
Keywords: Endoscopic ultrasound, Drainage, Liver, Intrahepatic lesion
Core tip: To review the available published trials, case series and case reports, discuss the implications and the future role of endoscopic ultrasound in the management of various liver conditions. Through this review paper we aim to provide a unified one stop educational experience as we have attempted to amalgamate all the published data.
INTRODUCTION
Since the initial description of endoscopic ultrasonography (EUS) in 1980’s, EUS has become an indispensable method not only in diagnosing various gastrointestinal (GI) lesions but also in performing various therapeutic maneuvers[1-4]. It was the limitations imposed by standard ultrasonography that prompted the development of EUS. By placing the ultrasound transducer within the body, interposed air filled or bony structures could be avoided and simultaneously by reducing the distance it became feasible to adequately visualize deeper structures. The method is basically an endoscopy with ultrasound at the tip which helps to visualize not only the GI tract but also produce images of nearby structures such as the gall bladder and bile ducts, pancreas, liver, etc. Echoendoscopes are designed using either a radial or curvilinear array system[1]. Radial endosonography provides a high-resolution, 360 degrees circumferential imaging of the GI tract and its surrounding structures. However, it does not allow for fine needle aspiration (FNA), thus making way for development of the linear echoendoscope enabling FNA of lesions both within and adjacent to GI tract[2,3]. This ability is the cornerstone of interventional EUS and the method has been proven safe and reliable in diagnosing various benign and malignant conditions in the upper and lower GI tract as well as the mediastinum[3,4]. When compared with other techniques EUS-FNA has demonstrated improved accuracy and cost effectiveness. This was especially well demonstrated in pancreatic lesions and malignant tumors of the esophagus[3,4].
Till late 1990’s the role of EUS in evaluating hepatic lesions was only described in a few case studies[5] but the case series by Nguyen et al[6] paved the way. They theorized that close proximity of the transducer to lesions coupled with clear visualizations and accessibility of the left lobe and central segments of the liver should facilitate the use of EUS in hepatic lesions. Since EUS-FNA was first reported in 1992[2], we have seen a tremendous growth of interventional EUS with various innovations such as EUS guided tru-cut biopsy, tumor ablative therapy, vascular interventions, and various transmural drainage procedures. However, though case series have been described limited trials advocating the use of EUS for liver lesions have been published and there are no dedicated guidelines establishing the role of EUS in hepatic applications at present. The aims of this review are to summarize the published reports on hepatic applications of EUS and to speculate on its future roles.
ANATOMICAL DESCRIPTION OF THE LIVER
The adjacent organs next to the liver include the stomach and duodenum (Figure 1). The liver has a dual blood supply with the portal vein (formed by the confluence of superior mesenteric vein and splenic vein) and the hepatic artery (branch of celiac artery). These vessels terminate at porta hepatis by dividing into right and left liver branches which undergo secondary and tertiary divisions to supply the various segments. Right, middle and left hepatic veins formed by the union of intersegmental collecting veins open into the inferior vena cava (IVC). The liver can subsequently be divided into 8 segments that are served independently by a secondary or tertiary branch of the portal triad. The caudate lobe is considered to be separate as it is supplied by both branches of the portal vein and drains independently into the IVC via hepatic veins. It is located posteriorly and considered to be segment one. The rest of the liver is divided by the main portal fissure hosting the middle hepatic vein which extends from the fundus of the gall bladder to the IVC. The left hepatic vein divides the left lobe into lateral (2, 3) and medial (4a, 4b) segments. The right hepatic vein divides the right lobe into anterior (5, 8) and posterior (6, 7) segments. The portal vein divides the liver into upper (2, 4a, 8, 7) and lower (3, 4b, 5, 6) segments. The segments are labeled in a clockwise manner. In a normal frontal view segments 1, 6 and 7 are not visible.
Figure 1.
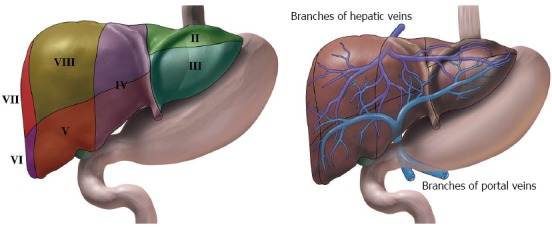
Illustrations of liver and its surrounding stomach and duodenum. A: The liver can subsequently be divided into 8 segments that is served independently by a secondary or tertiary branch of the portal triad. B: The left hepatic vein divides the left lobe into lateral (II2, III3) and medial (IV4a, IV4b) segments. The right hepatic vein divides the right lobe into anterior (V5, VIII8) and posterior (VI6, VII7) segments. The portal vein divides the liver into upper (II2, IV4a, VIII8, VII7) and lower (III3, IV4b, V5, VI6) segments. The segments are labeled in a clockwise manner. In a normal frontal view segments I1, VI6 and VII7 are not visible.
VISUALIZATION OF THE LIVER BY EUS
With currently available echoendoscopes, both mechanical and electronic transducers can scan over a range of frequencies ranging between 5 to 20 MHz. 1Scanning at higher frequencies improves image resolution but limits the penetration of the ultrasound beam to 1 to 2 cm from the probe, whereas scanning with lower frequency provides images of structures up to 6 to 8 cm from the probe. In 1986, Rifkin et al[7] incorporated 9 MHz electronic transducer on to a traditional fiber optic gastro scope and concluded that it had a better resolution than 0.5 mm.
Both the left lobe and caudate lobe lie in close proximity to the stomach and duodenum, hence providing an easy access during EUS (Figures 2 and 3). The caudate lobe and gastrohepatic space can be accessed by EUS while these are anatomically more difficult to approach by trans-abdominal ultrasound. EUS is limited in its ability to access the portion of the right lobe adjacent to the dome of the diaphragm along with its lateral and inferior portions. In spite of this, most of the right is lobe is visible from the duodenum as well as the portal hilum with its structures.
Figure 2.
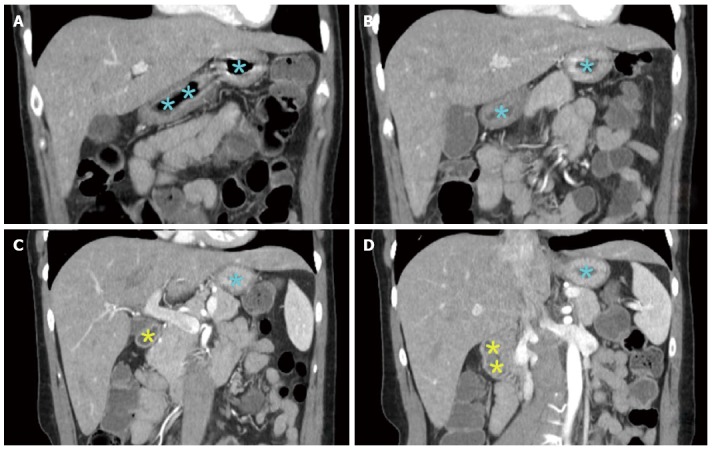
Selected computerized tomography scan images showing the liver and its surrounding stomach and duodenum. Both the left lobe and caudate lobe lie in close proximity to stomach (blue colored asterisk indicated gastric lumen) and duodenum (yellow colored asterisk indicated bulb and duodenal lumen), hence providing an easy access during endoscopic ultrasonography (EUS). The caudate lobe and gastrohepatic space can be accessed by EUS while are anatomically difficult to approached by trans-abdominal ultrasound. EUS is limited in its ability to access the portion of the right lobe adjacent to the dome of the diaphragm along with its lateral and inferior portions.
Figure 3.
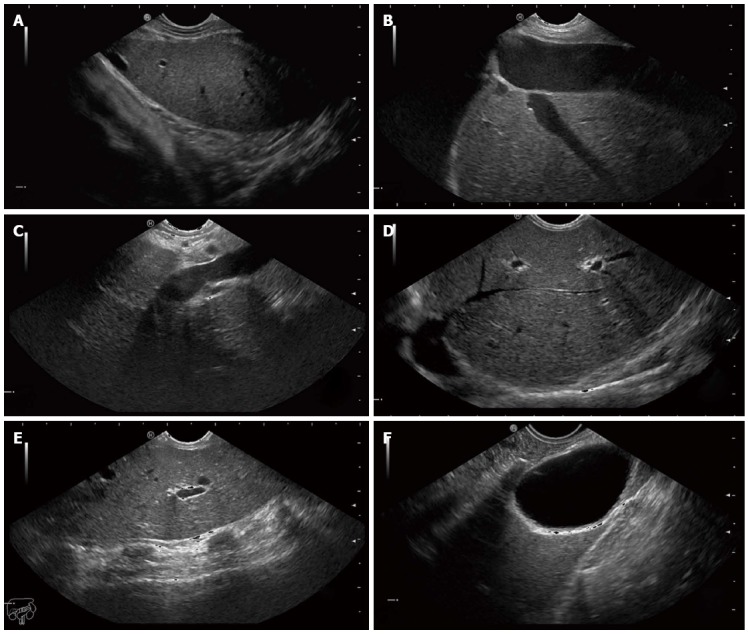
Endoscopic ultrasound images of the hepatic structures with the tip of the linear echoendoscope at different positions. A: Endoscopic ultrasound (EUS) image of the left liver lobe with the diaphragm. The image is obtained from the cardia region; B: EUS image of the left liver lobe with the inferior vena cava and a hepatic vein; C: EUS image of the liver at the portal ligament region showing from the transducer, the hepatic artery, the portal vein and a short segment of the common bile duct. The transducer is located in the stomach; D: EUS image of the liver looking over the hepatic dome; E: EUS image of the right hepatic lobe. Note the shadows from the ribs at the anterior abdominal wall; F: EUS image of the liver with the gall bladder. The transducer is located in the first part of the duodenum.
PubMed SEARCH
On December 20th, 2014, the authors performed PubMed search using these key word sets: EUS in combination with hepatic lesion, hepatic application, hepatic intervention, hepatocellular carcinoma, and hepaticogastrostomy (HGS). The inclusion criteria are: (1) english language publications only; (2) EUS is utilized; and (3) case report, series, clinical studies, potential hepatic applications in animal models, reviews on this topic. The authors excluded reports about EUS utilization in extrahepatic bile duct, gallbladder, and other extrahepatic structures except in management and diagnosis of complications of portal hypertension. We also excluded intraductal EUS application. Each published paper was reviewed and only important information was extracted for this review. Initial search yielded 731 articles out of which 584 were discarded as they did not meet the inclusion criteria. Please refer to the attached PubMed result search flow sheet for further details (Figure 4).
Figure 4.
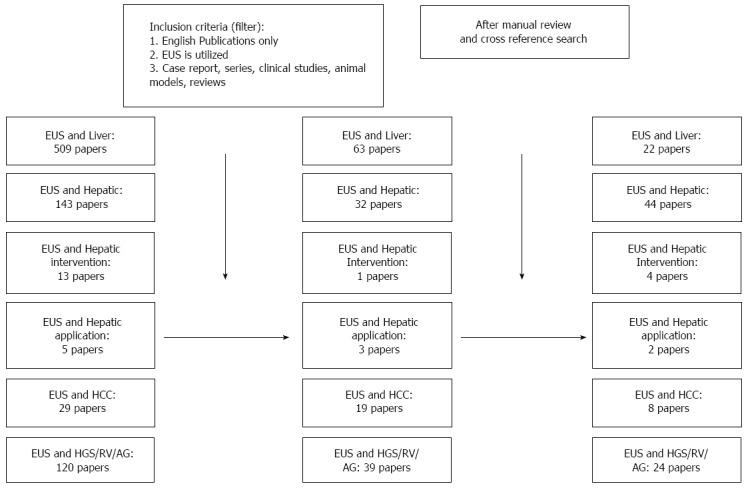
PubMed result search flow sheet. PubMed search was performed on December 20, 2014. EUS: Endoscopic ultrasound; HCC: Hepatocellular carcinoma; HGS: Hepaticogastrostomy.
ROLES OF EUS IN THE EVALUATION OF HEPATIC LESIONS
Focal liver lesions
Diagnostic EUS: Focal liver lesions include both benign (such as hepatic cysts, abscess, adenoma or hemangioma) and malignant (such as hepatocellular carcinoma, intrahepatic cholangiocarcinoma, biliary cystadenoma, and metastatic liver disease) lesions (Figure 5 and Table 1). These lesions were most often diagnosed by either abdominal imaging or by percutaneous tissue diagnosis. The last 15 to 20 years have seen rapid advancements in the applicability of EUS, especially combined with FNA cytology. Studies[8,9] have not only established its efficacy in evaluating intra-abdominal lesions but in also staging[10] of various GI tumors. However it was not till 1999[5] when EUS was used for clinical imaging of the liver. Studies[11,12] comparing intraoperative ultrasound to preoperative computed tomography (CT) scan and magnetic resonance imaging (MRI) had proven it to be superior owing to the proximity of the ultrasound probe to the liver parenchyma and the use of color flow Doppler - hence the idea of EUS for liver lesions was considered. Nguyen et al[6] evaluated the liver in 574 consecutive patients undergoing upper EUS examination for suspicion or history of GI or pulmonary tumor: 15 liver lesions were identified (5 were in the right lobe and 9 were in the left lobe) and underwent EUS-FNA, 14 of them were found to be malignant (one of the patients underwent FNA of two lesions as the first lesion revealed normal cytology). Surprisingly CT scan done prior to EUS identified only 3 of these liver lesions: 12 of the 15 lesions were less than 2 cm. Thus EUS became recognized as a modality to help detect small focal liver lesions. This was also demonstrated by a retrospective study reported by Prasad et al[13] where in liver lesions as small as 5 mm not seen by previously conducted noninvasive imaging were detected by EUS. The detection of metastatic disease is particularly important as it influences management of these patients. It is important to realize that EUS is a semi-invasive test with complications. Two patients in this study had duodenal injury. Hence, though the data appears promising more studies are needed to compare the risk benefit ratio and to establish a protocol for detection of liver masses. Awad et al[14] then evaluated 14 consecutive patients with a history of a known liver mass. They underwent both dynamic CT scan and EUS. EUS not only identified the lesions in all the 14 patients but it also recognized 4 new lesions smaller than 0.5 cm which had not been visualized by CT scan. In 2002 Tenberge et al[15] published a retrospective study wherein they sent a questionnaire to EUS-FNA centers around the world. Out of the 130 centers, 21 of them reported 167 cases of EUS-FNA of the liver with a complication rate of only 4%. Further, it helped to diagnose malignancy in cases of non-diagnostic FNA obtained under trans-abdominal ultrasound and localize primary tumor in cases where CT only reported liver metastasis. Thus the authors concluded that EUS-FNA of the liver was a safe procedure which should be considered in case the lesion is not accessible by trans-abdominal ultrasound or CT or when FNA is non diagnostic by these methods or when a liver lesion is detected during routine EUS. As described in the anatomy section EUS provides good visualization of the left hepatic lobe and EUS-FNA of liver lesions may provide important management information especially in case of detection of metastasis or hepatocellular carcinoma. Further it is hypothesized that in patients with cirrhosis percutaneous biopsy may be difficult owing to presence of ascites and coagulopathy. In such cases EUS may be a safer option as the transducer is only 1.5-3 cm away from the lesion and biopsy occurs under EUS guidance. A retrospective study[16] of 77 patients who underwent EUS FNA of various solid liver lesions helped to detect malignancy in 41% of patients who had previously had negative examination. This was the first study to include both malignant and benign lesions. They concluded that sensitivity of diagnosing malignancy ranged from 82% to 94% (7 patients from the nonmalignant group died without follow up imaging, biopsy or autopsy and hence could not be classified) and this group did not have any complications. The presence of two or more lesions with regular outer margins is more indicative of a malignant lesion. In a prospective study by Hollerbach et al[17] EUS-FNA provided appropriate biopsy specimen in 40/41 patients with an average of 1.4 needle passes. On combining both histological and cytological examination of the specimens they had a sensitivity of 94% and a specificity of 100% with a low 2.5% rate of minor complication. A Fritscher-Ravens et al[18] reported a case series of 10 patients with a biliary stricture at the hepatic hilum who underwent EUS-FNA. In 9/10 patients’ adequate specimens were obtained and 8 of these lesions were found to be malignant but one lesion was falsely identified as benign. This study highlights an important implication of EUS as various advances are being made in the management of cholangiocarcinoma, thus it is imperative that we have not only have accurate diagnosis but also stage the disease adequately. Studies so far have revealed that brush cytology from endoscopic retrograde cholangiopancreatography (ERCP) has variable sensitivity. Ryan[19] reported a sensitivity of only 44% while Glasbrenner et al[20] reported a sensitivity of 80%. Subsequently Crowe et al[21] in 2006 compared 34 percutaneous CT-FNA liver biopsies to 16 EUS-FNA liver biopsies and concluded that though they were comparable in terms of diagnostic utility for hepatic lesions, EUS was limited in its ability to access the portion of the right lobe adjacent to the dome of the diaphragm along with its lateral and inferior portions. Thus, EUS is an important tool to use in adjunction with other noninvasive imaging methods to not only detect occults metastasis but also to diagnose focal malignant lesions more so in the left hepatic lobe.
Figure 5.
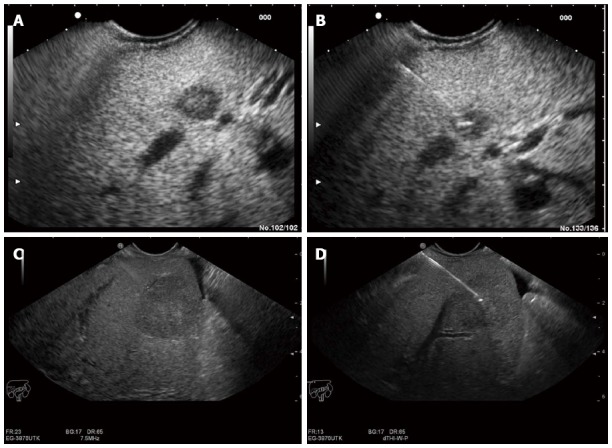
Endoscopic ultrasound image of lesion in the liver. A: Endoscopic ultrasound (EUS) image of an 8 mm metastatic lesion in the liver; B: Endoscopic ultrasound (guided biopsy from the same lesion; C: EUS image of a 25 mm lesion in the liver; D: EUS guided aspiration biopsy from the same lesion.
Table 1.
Reported diagnostic yields of endoscopic ultrasound guided fine needle aspiration of hepatic solitary lesions
| Ref. | Patient number/lesion sampled | Diagnostic yields |
| Nguyen et al[6] | 574/15 | CT before EUS depicted liver lesions in 3 of the 14 patients (21%) |
| Awad et al[14] | 14/9 | EUS identified additional lesions in 28% of the patients and changed clinical management in 67% of the patients |
| TenBerge et al[15] | 167/167 | EUS-FNA diagnosed malignancy in 89% of cases after non diagnostic FNA under trans abdominal US guidance |
| DeWitt et al[16] | 77/77 | 45 (58%) were diagnostic for malignancy, 25 (33%) were benign and seven (9%) were non diagnostic. EUS detected malignancy in 41% of patients with previously negative exam |
| HollerBach et al[17] | 41/41 | With combination of histological and cytological examination sensitivity and specificity for detecting malignancy was 94% and 100% |
| Prasad et al[13] | 222/21 | Diagnostic of malignancy in 15 (6.8%) 5 of whom (2.3%) had normal imaging prior |
| Crowe et al[21] | 50/16 | Diagnostic of malignancy in 56% of the cases, comparable to CT scan |
| McGrath et al[105] | 98/5 | The sensitivity of EUS-FNA for liver lesions was 80%. These lesions were not evident on prior noninvasive imaging |
| Singh et al[106] | 132/26 | The diagnostic accuracy of EUS/EUS-FNA and CT scan was 98% and 92% respectively |
EUS: Endoscopic ultrasonography; FNA: Fine needle aspiration; CT: Computed tomography.
More recently, EUS elastography used for visualization of tissue elasticity during routine EUS[22] is an upcoming modality for diagnosing focal liver lesions. It is based on the same principle of trans-abdominal elastography but it offers an additional advantage of comparing the echoes over several seconds of normal breathing and blood circulation thus overcoming the need for applying manual pressure. This technique was utilized by Rustemovic et al[23] in diagnosis of focal liver masses Since the malignant tumor tissue is harder than benign tumors, efforts have been made to utilize this modality in differentiating benign from malignant tumors. This principle was already established in other tumors such as prostate[24], pancreas[25]and breast[26]. In 2008 Kato et al[27] established that intraoperative usage of real time elastrography could help distinguish between HCC and metastases by dividing the tumors into four different types based on elasticity. In 2012, Sandulesco et al[28] published a pilot study using real time sonography to differentiate focal liver lesions and concluded that the sensitivity, specificity, and accuracy of differentiation of benign and malignant masses were 92.5%, 88.8%, and 88.6%, respectively. Hara et al[29] described a novel approach to assess vascular invasion at the hepatic hilum by using the linear scanning which they postulated had a superior visualization of abdominal vessels than radial scanning.
Therapeutic EUS in focal liver lesions: More recently there are case reports pushing the frontiers of EUS from being just a diagnostic tool to one with therapeutic benefits. EUS guided ethanol injection in treatment of hepatic metastasis was first described in 2002[30]. Since then few more cases[31-33] have been reported but unfortunately there are no long term data or larger case series to draw any significant conclusions. In 2011 Di Matteo et al[34] described the use of Nd: YAG laser ablation of hepatocellular carcinoma in the caudate lobe. More recently fiducial placement for stereotactic body radiation under EUS guidance for hepatic and pancreatic malignancies was reported[35].
Hepatic cysts
With the increasing imaging using ultrasound and CT scan, simple hepatic cysts are now routinely detected in 2.5%-7% of the population[36]. In majority of the time they are asymptomatic and need no further treatment. Only 10%-16% of such cysts are producing symptoms such as abdominal pain, hepatomegaly, early satiety, bile duct compression necessitating the need for treatment. Traditionally a surgical approach (complete cyst excision or fenestration of cyst) or percutaneous aspiration were the modalities used to treat large symptomatic hepatic cysts. Percutaneous aspiration is associated with a recurrence rate of nearly 100% in 2 years[37]. In 1985 Bean and Rodan[38] described successful percutaneous aspiration of 6 hepatic cysts followed by sclerotherapy with alcohol. No recurrence was noted during a 6-18 mo follow up period. These authors concluded that alcohol caused cellular destruction followed by fibrotic obliteration of the cysts. Since then multiple studies have established the efficacy of percutaneous aspiration with sclerotherapy. Lee et al[39] conducted a retrospective study where he hypothesized that EUS guided aspiration and lavage therapy without a percutaneous drainage catheter, would enable it to be performed in a single step. A total of 17 patients with 19 hepatic cysts were enrolled with a median cysts volume of 368.9 mL. Ten cysts were drained by a percutaneous approach and 8 cysts underwent EUS guided aspiration and lavage treatment. In a 15-mo follow up the EUS guided group showed 100% reduction. The authors concluded that EUS guided drainage was a safe method for left sided hepatic cysts while percutaneous catheter drainage is preferred for large right sided cysts.
Hepatic abscesses
Hepatic abscesses are collections of infected materials in the parenchyma which usually develop directly from the biliary tree or from extension of intra-abdominal infection or hematogenously from bacteremia. Conventionally hepatic abscesses have been treated with either surgical or percutaneous drainage[40,41]. Owing to high morbidity and mortality (almost 32%) associated with surgical drainage[40,41]. percutaneous drainage with success rates of 80%-100% has emerged as the first line of therapy[42]. Unfortunately this is also associated with certain side effects[43] such as injury to surrounding vascular structures, intraperitoneal bleeding, hepato-venous fistula[44] and patient discomfort due to external drainage. EUS guided hepatic abscess drainage[45] was suggested as an alternative to overcome some of the complications. As described before, both the left lobe and caudate lobe lie in close proximity to the stomach and duodenum, hence providing an easy access during EUS. In 2005 Seewald et al[45] described a case report of a large hepatic abscess in the lateral segments of the left lobe that did not resolve with one week of intravenous antibiotic therapy. The authors performed EUS guided transgastric drainage of the hepatic abscess. At 6 mo follow up the patient still remained asymptomatic. In 2010 Noh et al[46] described a case series of three hepatic abscesses localized to the caudate lobe and the gastrohepatic space which were anatomically difficult to drain percutaneously. These patients underwent EUS guided drainage and had complete resolution on follow up. The EUS method was hypothesized to be better as it provided excellent visualization of the abscess cavity and the close approximation of the transducer to the cavity wall aided in direct passage of the needle into the cavity. Color Doppler prevented accidental puncturing of interposed vessels. A total of 7 cases have been reported with no single complication and a success rate of 100%[47]. Moving forward we need further studies to establish its efficacy and recommend as a standard therapy. Further, its use may be limited in right sided abscesses. As of now it can be offered to patients as an attractive alternative especially if percutaneous drainage fails.
Hemobilia
With the advent of invasive hepatobiliary procedures[48] such as percutaneous biopsy, biliary drainage and transhepatic cholecystography the incidence of hemobilia has been on a rise. Most common causes include accidental or iatrogenic trauma. The bleeding typically starts within 4 wk[48] of the trauma though cases with longer time periods have been reported. They are most commonly diagnosed by hepatic angiography and often treated with embolization[49]. Cattan et al[50] described a case report where in hemobilia occurred nearly 4 mo after hepatic injury and was diagnosed successfully by EUS. The patient underwent upper endoscopy with both front viewing and side viewing endoscopy along with EUS which revealed the presence of mobile hyperechoic material with no acoustic shadow in the bile duct and gall bladder suggestive of hemobilia. Trakarnsanga et al[51] described another case where a patient presented with abdominal pain and jaundice and underwent EUS with Doppler which revealed a large cystic lesion with a detectable to and fro color flow arising from the common hepatic artery. Diagnosing hemobilia is always challenging, ultrasound and CT scan help by detecting the presence of hematoma or arteriovenous fistula. On occasions they may also detect blood clots in the bile ducts, however these findings are not always present[52]. Hence we postulate that in cases of unexplained GI bleeding especially after hepatic trauma, certain imaging studies such as EUS should be considered.
Portal hypertensive complications and hepatic cirrhosis
The past decade has seen increasing interest in using EUS for not only early diagnosis of portal hypertension but also for treatment of varices. EUS combined with the Doppler technique helps in the detailed evaluation of the distal esophagus. Though initial studies[53] were not encouraging, later studies[54] showed that EUS could adequately identify high risks of bleeding by determining the size of the varix. Careful examination of the gastroesophageal junction with upper endoscopy helps to identify large varices, however small varices and gastric varices may be missed. In a study by Choudhuri et al[55], gastric varices were detected more often with EUS than with endoscopy alone. In addition EUS can also help to identify deep venous plexus such as peri-esophageal and para-esophageal varices. In his study, Lee et al[56] compared cirrhotics and patients with dyspepsia to assess gastroesophageal varices and extra luminal venous abnormalities. EUS detected gastric varices in 30.8% when compared to 17.3% detected via upper endoscopy alone. Further with EUS extraluminal venous abnormality was noted in 92% of people with cirrhosis. These changes include early formation and engorgement of collateral vessels in the distal esophagus, proximal stomach and splenic vein. Thus there is a potential for possible early detection of cirrhosis as these changes cannot be seen by regular endoscopy. This was further demonstrated by a study done by Mckiernan et al[57] in Birmingham, United Kingdom where 16 children with intestinal failure underwent both endoscopy and EUS to assess for the need of combined intestinal and liver transplant if indicated by presence of intestinal failure associated liver disease. In 7 patients gastroesophageal varices was only detected by EUS and not by regular endoscopy thus resulting in fewer liver biopsies in this subset of patients. Various studies conducted over the last decade helped to establish that EUS can also be used to predict the recurrences of esophageal varices after therapy. Irisawa et al[58] in 2001 published a retrospective study of 38 patients who had undergone endoscopic injection sclerotherapy. Presence of severe type peri-esophageal collateral veins and large perforating veins were associated with increased recurrence of esophageal varices. In 2003[59] he studied 18 patients and concluded that para-esophageal collateral veins detected after the sclerotherapy sessions predicted recurrence. Sato et al[60] studied 306 patients whose varices had been treated with endoscopic injection sclerotherapy with endoscopic color Doppler ultrasonography and concluded that presence of patent inflowing perforating veins before and after sclerotherapy was predictive of early variceal recurrence. Presence of severe cardial sub mucosal veins and severe grade perforating veins[54] and presence of rapid hepatofugal flow velocity of 12 cm/s or more (The group tested a variety of cutoff points from 5 to 18 cm/s, and chose 12 cm/s as the cutoff point since it gave the maximal differences in prognoses between the low- and high-risk groups) in the left gastric vein[61] have also been reported to be associated with early recurrence of esophageal varices after treatment. Benefits of EUS extend not only to diagnosis but studies have shown therapeutic benefits as well. Especially in fundal varices which are not amenable to band ligation, EUS guided techniques such as injection of cyanoacrylate[62] and/or cyanoacrylate with coiling[63] eradicating of gastric varices have been useful. Romero-Castro et al[63] conducted a multicenter study comparing cyanoacrylate against EUS guided coil application. Though it was a small non randomized group, the EUS guided coil application group required fewer endoscopies and had fewer adverse effects. In a randomized control trial by de Paulo et al[64], EUS guided sclerotherapy was proven to be as effective as endoscopic sclerotherapy. However larger randomized controlled trials are needed to substantiate the claim.
Initially described in 1969[65], transjugular intrahepatic portosystemic shunt has certainly come a long way to becoming an effective tool in the management of portal hypertension[66], especially in the management of refractory ascites and variceal bleeding not responding to endoscopic therapy[67]. With the emerging role of EUS in diagnosis and management of various hepatobiliary conditions there have been studies conducted which push the boundaries a bit further. In 2004 Lai et al[68] demonstrated for the first time the feasibility of EUS guided extrahepatic portal vein puncture and portography in an animal model. Since then few studies[69,70] on porcine models have established the efficacy and feasibility of EUS guided portal vein catheterization in portal angiography and portal vein pressure measurements. Subsequently, in 2009 Buscaglia et al[71] reported the first successful endoscopic creation of intrahepatic portosystemic shunt (IPSS) in 10 porcine models without any complications. They concluded that their technique of EUS guided IPSS was technically feasible and a comparative alternative with few advantages such as avoiding the entrance through heart or IVC and decreasing the radiation exposure to both the patient and physician. Further studies are needed with large diameter covered stents[72], deployment of the proximal end of the stent into the hepatic vein-IVC confluence to promote stent patency[73] and in cirrhotics to test the safety of this technique prior to conducting human studies.
Detection of fibrosis of the liver has important management implications and although liver biopsy is still considered “a gold standard”, studies have proven this technique to be less perfect owing to sampling errors, inter-observer variability[74] and complications[75]. Various serum markers and imaging tests[76] such as FibroScan (EchoSens, Paris, France)[77] have been developed and are being tested to assess their efficacy in staging the liver disease. In 2009, Rimbaş et al[78] postulated that mapping of the tissue elasticity distribution might prove to be useful in accurately determining stages of liver disease. He further commented that in comparison to FibroScan, real time EUS elastography not only allows for estimation of liver stiffness in all patients (irrespective of obesity) but it can also differentiate between steatosis and fibrosis thus giving it an edge. Further studies are needed to confirm these hypotheses.
Portal vein
In patients undergoing extensive hepatectomy preoperative embolization of portal vein branches causing atrophy of the segments to be removed with subsequent compensatory hypertrophy of the remaining segments[79] has proven to be safe and effective[79,80]. Matthes et al[81] reported the first successful EUS guided selective embolization of the portal vein with Enteryx (ethylene-vinyl alcohol copolymer) in a single swine model. The group thus concluded that EUS guidance appears to be feasible and a potential minimally invasive preoperative treatment option for patients undergoing extensive hepatectomy. Moving forward more studies need to be conducted to establish its clinical efficacy.
INTRAHEPATIC BILE DUCT
Currently ERCP is considered be a gold standard for relieving biliary obstruction and when this fails the only alternative is surgery or percutaneous approach both of which are unfortunately associated with higher mortality and morbidity[82]. With the advent of EUS and the easy access of left hepatic duct from the gastric wall paved the way for EUS guided transgastric approach to biliary system. This was initially described[83] in patients with biliary obstruction who had failed either endoscopic or percutaneous transhepatic drainage by Giovannini et al[83] in 2003. Following this few more case reports[84,85] were published expanding interventional EUS guided biliary drainage as an attractive alternative. Subsequently, Bories et al[86] published a pilot series of 11 patients who underwent EUS guided transgastric drainage of the left hepatic system. Out of 11 patients the procedure was a success in 10 of them. Panpimanmas et al[87] also reported successful EUS guided HGS in two patients with hilar cholangiocarcinoma who had failed ERCP. Currently there are three endoscopic drainage procedures[88,89] described in the literature which includes above mentioned EUS-guided transluminal biliary drainage including choledocoduodenostomy and hepaticogastrostomy (EUS-HGS), EUS-rendezvous technique (EUS-RV), and EUS-antegrade approach (EUS-AG) of which EUS-HGS is indicated in cases of surgically altered anatomy and duodenal obstruction with tumor invasion that precludes the passage of echo endoscope. There are certain limitations to this approach as were listed by Itoi et al[90] in his review such as nonapposed gastric wall and left liver lobe causing procedure failure, difficulty of puncture in cases of liver cirrhosis and risk of puncturing the portal vein. A multicenter retrospective study[91] was conducted across seven tertiary centers in Japan where 64 patients were enrolled. Out of these 20 of them underwent EUS-HGS. Technical success rate was 95% but the stent dysfunction rate and 3 mo dysfunction free patency rate was 32% and 51% respectively with 6/20 patients experiencing procedure related complications. The most common complications associated with this include bile leakage and stent misplacement. EUS guided ante grade stenting (EUS-AS) was developed as an alternative to reduce the complications. Ogura et al[92] described a pilot study in 12 patients where he combined the EUS-HGS with EUS-AS of the biliary obstruction using an uncovered metallic stent. At the time of follow up only one patient had experienced mild pancreatitis. Ogura et al[93] also described a novel method called locking stent method using the end-bare covered metallic stents to prevent stent dysfunction. Initially its scope was limited only to the left intrahepatic drainage but in 2014 Ogura et al[94] described a successful biliary drainage of hepatic hilar obstruction further expanding its horizons. EUS-RV technique is indicated when the biliary cannulation fails or there is a biliary stricture that cannot be passed. It involves creation of temporary fistula using EUS and placement of guidewire via the biliary duct and ampulla into the duodenum. After this ERCP is re attempted to cannulate the bile duct using the guidewire. It can be divided into two types transhepatic and transduodenal. Transduodenal can be further divided into two types according to the endoscope position: long (push) and short (pull)[95]. In 2004 Mallery et al[96] described feasibility of rendezvous technique for biliary drainage in 6 cases. Few studies[97,98] with over 40 patients have been published which have reported technical success rate in 60’s and 70’s. A retrospective study by Dhir et al[99] comparing the precut papillotomy to Rendezvous technique in patients with failed cannulation revealing higher success rate with EUS-RV.
EUS guided antegrade techniques are suitable for patients with altered surgical anatomy[100] or upper intestinal obstruction which prohibits the scope from reaching the biliary orifice. It involves accessing the intrahepatic biliary duct by creation of a temporary fistula between the intestine and IHBD followed by dilation of the fistula with subsequent stent placement or balloon dilation for biliary obstruction.
Park et al[101] in 2012 successfully described EUS-guided transhepatic antegrade balloon dilation in a 45-year-old female with hepaticojejunostomy. She had presented with bilioenteric anastomotic stricture and had failed deep enteroscopy with a pediatric colonoscopy and double balloon enteroscope. Further in a prospective series by Park et al[102] 14 patients underwent antegrade technique out of which it was successful in 8 of them. A retrospective study by Shah et al[103] reported a success rate of 81%.
In 2013, Park et al[104] published a prospective series in which he not only described but also evaluated the technical feasibility and safety of EUS-guided hepaticoduodenostomy (EUS-HD) in cases of isolated right intrahepatic duct (IHD) obstruction. EUS guided cholangiography of the right IHD was successfully performed in all 6 patients and he described 3 kinds of approaches: (1) using a cholangiogram obtained by EUS-guided transduodenal puncture of the right hepatic duct as a “roadmap” to assist retrograde cannulation; (2) EUS-guided antegrade transanastomotic balloon dilation with or without stenting; and (3) EUS-BD with transluminal stenting between the right hepatic duct and the duodenal wall as an antegrade bypass stenting. Though it is an attractive alternative to PTBD in patients with isolated IHD more studies are needed to establish its efficacy.
CONCLUSION
Although diagnostic and therapeutic EUS is an established tool for upper GI and pancreatic applications, the authors believe that its indications and utilizations in hepatic pathologies are under-recognized. For example, EUS is able to depict and biopsy even small solid lesions in the liver that are either not visualized by other imaging modalities or visualized during routine staging procedures of GI or pulmonary cancers. However, its diagnostic role for hepatic applications is at present not fully defined. Comparative studies are needed. The therapeutic role of EUS in hepatic applications is increasing in particular regarding internal drainage procedures in patients with intrahepatic abscesses in the left lobe and in patients with biliary obstruction and altered anatomy of the GI tract. However close monitoring of the results is mandatory due to the risk of complications such as bile leakage.
EUS is definitely one of the most emerging technologies with significant clinical ramifications. There has also been a substantial interest in the future roles of EUS. The authors expect future development and expanded hepatic applications of EUS in two directions: improved diagnostic yield and evolved indications with new EUS imaging technologies and hard wares, and growth in therapeutic EUS with new EUS and other endoscopic devices. Since the left lobe and caudate lobe lie in close proximity to stomach and duodenum, providing an easy access during EUS, more EUS applications should be seen within left, caudate lobe, and gastrohepatic space. With current technology, EUS is limited in its ability to access the portion of the right lobe adjacent to the dome of the diaphragm along with its lateral and inferior portions, trans-abdominal ultrasound can complement EUS and achieve total hepatic coverage by ultrasound imaging. Interventional EUS and/or trans-abdominal ultrasound can be utilized to approach various pathologies associated with hepatic parenchyma, intrahepatic biliary system, and vascular structures. The authors expect to see more EUS guided injection ablative therapy for hepatic tumors or cysts with ethanol, sclerosant, chemotherapeutics, and biologics, and EUS guided fiducial placement for stereotactic body radiation.
Footnotes
Conflict-of-interest statement: No potential conflicts of interest relevant to this article were reported.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: May 11, 2015
First decision: September 11, 2015
Article in press: October 13, 2015
P- Reviewer: Kitano M, Mendez-Sanchez N, Picardi A S- Editor: Qi Y L- Editor: A E- Editor: Zhang DN
References
- 1.Tierney WM, Adler DG, Chand B, Conway JD, Croffie JM, DiSario JA, Mishkin DS, Shah RJ, Somogyi L, Wong Kee Song LM, et al. Echoendoscopes. Gastrointest Endosc. 2007;66:435–442. doi: 10.1016/j.gie.2007.05.028. [DOI] [PubMed] [Google Scholar]
- 2.Vilmann P, Jacobsen GK, Henriksen FW, Hancke S. Endoscopic ultrasonography with guided fine needle aspiration biopsy in pancreatic disease. Gastrointest Endosc. 1992;38:172–173. doi: 10.1016/s0016-5107(92)70385-x. [DOI] [PubMed] [Google Scholar]
- 3.Kaul V, Adler DG, Conway JD, Farraye FA, Kantsevoy SV, Kethu SR, Kwon RS, Mamula P, Pedrosa MC, Rodriguez SA, et al. Interventional EUS. Gastrointest Endosc. 2010;72:1–4. doi: 10.1016/j.gie.2010.01.023. [DOI] [PubMed] [Google Scholar]
- 4.Alvarez-Sánchez MV, Jenssen C, Faiss S, Napoléon B. Interventional endoscopic ultrasonography: an overview of safety and complications. Surg Endosc. 2014;28:712–734. doi: 10.1007/s00464-013-3260-5. [DOI] [PubMed] [Google Scholar]
- 5.Bogstad J, Vilmann P, Burcharth F. Early detection of recurrent hepatocellular carcinoma by endosonographically guided fine-needle aspiration biopsy. Endoscopy. 1997;29:322–324. doi: 10.1055/s-2007-1004198. [DOI] [PubMed] [Google Scholar]
- 6.Nguyen P, Feng JC, Chang KJ. Endoscopic ultrasound (EUS) and EUS-guided fine-needle aspiration (FNA) of liver lesions. Gastrointest Endosc. 1999;50:357–361. doi: 10.1053/ge.1999.v50.97208. [DOI] [PubMed] [Google Scholar]
- 7.Rifkin MD, Gordon SJ. Sonoendoscopic evaluation of extraesophageal and extragastric abnormalities: a review. Scand J Gastroenterol Suppl. 1986;123:68–73. doi: 10.3109/00365528609091865. [DOI] [PubMed] [Google Scholar]
- 8.Jhala NC, Jhala DN, Chhieng DC, Eloubeidi MA, Eltoum IA. Endoscopic ultrasound-guided fine-needle aspiration. A cytopathologist’s perspective. Am J Clin Pathol. 2003;120:351–367. doi: 10.1309/MFRF-J0XY-JLN8-NVDP. [DOI] [PubMed] [Google Scholar]
- 9.Shin HJ, Lahoti S, Sneige N. Endoscopic ultrasound-guided fine-needle aspiration in 179 cases: the M. D. Anderson Cancer Center experience. Cancer. 2002;96:174–180. doi: 10.1002/cncr.10614. [DOI] [PubMed] [Google Scholar]
- 10.Chang KJ, Katz KD, Durbin TE, Erickson RA, Butler JA, Lin F, Wuerker RB. Endoscopic ultrasound-guided fine-needle aspiration. Gastrointest Endosc. 1994;40:694–699. [PubMed] [Google Scholar]
- 11.Clarke MP, Kane RA, Steele G, Hamilton ES, Ravikumar TS, Onik G, Clouse ME. Prospective comparison of preoperative imaging and intraoperative ultrasonography in the detection of liver tumors. Surgery. 1989;106:849–855. [PubMed] [Google Scholar]
- 12.Soyer P, Elias D, Zeitoun G, Roche A, Levesque M. Surgical treatment of hepatic metastases: impact of intraoperative sonography. AJR Am J Roentgenol. 1993;160:511–514. doi: 10.2214/ajr.160.3.8430544. [DOI] [PubMed] [Google Scholar]
- 13.Prasad P, Schmulewitz N, Patel A, Varadarajulu S, Wildi SM, Roberts S, Tutuian R, King P, Hawes RH, Hoffman BJ, et al. Detection of occult liver metastases during EUS for staging of malignancies. Gastrointest Endosc. 2004;59:49–53. doi: 10.1016/s0016-5107(03)02378-2. [DOI] [PubMed] [Google Scholar]
- 14.Awad SS, Fagan S, Abudayyeh S, Karim N, Berger DH, Ayub K. Preoperative evaluation of hepatic lesions for the staging of hepatocellular and metastatic liver carcinoma using endoscopic ultrasonography. Am J Surg. 2002;184:601–64; discussion 601-64;. doi: 10.1016/s0002-9610(02)01092-9. [DOI] [PubMed] [Google Scholar]
- 15.tenBerge J, Hoffman BJ, Hawes RH, Van Enckevort C, Giovannini M, Erickson RA, Catalano MF, Fogel R, Mallery S, Faigel DO, et al. EUS-guided fine needle aspiration of the liver: indications, yield, and safety based on an international survey of 167 cases. Gastrointest Endosc. 2002;55:859–862. doi: 10.1067/mge.2002.124557. [DOI] [PubMed] [Google Scholar]
- 16.DeWitt J, LeBlanc J, McHenry L, Ciaccia D, Imperiale T, Chappo J, Cramer H, McGreevy K, Chriswell M, Sherman S. Endoscopic ultrasound-guided fine needle aspiration cytology of solid liver lesions: a large single-center experience. Am J Gastroenterol. 2003;98:1976–1981. doi: 10.1111/j.1572-0241.2003.07638.x. [DOI] [PubMed] [Google Scholar]
- 17.Hollerbach S, Willert J, Topalidis T, Reiser M, Schmiegel W. Endoscopic ultrasound-guided fine-needle aspiration biopsy of liver lesions: histological and cytological assessment. Endoscopy. 2003;35:743–749. doi: 10.1055/s-2003-41593. [DOI] [PubMed] [Google Scholar]
- 18.Fritscher-Ravens A, Broering DC, Sriram PV, Topalidis T, Jaeckle S, Thonke F, Soehendra N. EUS-guided fine-needle aspiration cytodiagnosis of hilar cholangiocarcinoma: a case series. Gastrointest Endosc. 2000;52:534–540. doi: 10.1067/mge.2000.109589. [DOI] [PubMed] [Google Scholar]
- 19.Ryan ME. Cytologic brushings of ductal lesions during ERCP. Gastrointest Endosc. 1991;37:139–142. doi: 10.1016/s0016-5107(91)70671-8. [DOI] [PubMed] [Google Scholar]
- 20.Glasbrenner B, Ardan M, Boeck W, Preclik G, Möller P, Adler G. Prospective evaluation of brush cytology of biliary strictures during endoscopic retrograde cholangiopancreatography. Endoscopy. 1999;31:712–717. doi: 10.1055/s-1999-73. [DOI] [PubMed] [Google Scholar]
- 21.Crowe DR, Eloubeidi MA, Chhieng DC, Jhala NC, Jhala D, Eltoum IA. Fine-needle aspiration biopsy of hepatic lesions: computerized tomographic-guided versus endoscopic ultrasound-guided FNA. Cancer. 2006;108:180–185. doi: 10.1002/cncr.21912. [DOI] [PubMed] [Google Scholar]
- 22.Saftoiu A, Vilman P. Endoscopic ultrasound elastography-- a new imaging technique for the visualization of tissue elasticity distribution. J Gastrointestin Liver Dis. 2006;15:161–165. [PubMed] [Google Scholar]
- 23.Rustemovic N, Hrstic I, Opacic M, Ostojic R, Jakic-Razumovic J, Kvarantan M, Pulanic R, Vucelic B. EUS elastography in the diagnosis of focal liver lesions. Gastrointest Endosc. 2007;66:823–824; discussion 824. doi: 10.1016/j.gie.2007.06.047. [DOI] [PubMed] [Google Scholar]
- 24.Tsutsumi M, Miyagawa T, Matsumura T, Kawazoe N, Ishikawa S, Shimokama T, Shiina T, Miyanaga N, Akaza H. The impact of real-time tissue elasticity imaging (elastography) on the detection of prostate cancer: clinicopathological analysis. Int J Clin Oncol. 2007;12:250–255. doi: 10.1007/s10147-007-0669-7. [DOI] [PubMed] [Google Scholar]
- 25.Săftoiu A, Vilmann P, Gorunescu F, Gheonea DI, Gorunescu M, Ciurea T, Popescu GL, Iordache A, Hassan H, Iordache S. Neural network analysis of dynamic sequences of EUS elastography used for the differential diagnosis of chronic pancreatitis and pancreatic cancer. Gastrointest Endosc. 2008;68:1086–1094. doi: 10.1016/j.gie.2008.04.031. [DOI] [PubMed] [Google Scholar]
- 26.Itoh A, Ueno E, Tohno E, Kamma H, Takahashi H, Shiina T, Yamakawa M, Matsumura T. Breast disease: clinical application of US elastography for diagnosis. Radiology. 2006;239:341–350. doi: 10.1148/radiol.2391041676. [DOI] [PubMed] [Google Scholar]
- 27.Kato K, Sugimoto H, Kanazumi N, Nomoto S, Takeda S, Nakao A. Intra-operative application of real-time tissue elastography for the diagnosis of liver tumours. Liver Int. 2008;28:1264–1271. doi: 10.1111/j.1478-3231.2008.01701.x. [DOI] [PubMed] [Google Scholar]
- 28.Sandulescu L, Padureanu V, Dumitrescu C, Braia N, Streba CT, Gheonea DI, Cazacu S, Ciurea T, Rogoveanu I, Saftoiu A. A pilot study of real time elastography in the differentiation of focal liver lesions. Curr Health Sci J. 2012;38:32–35. [PMC free article] [PubMed] [Google Scholar]
- 29.Hara K, Bhatia V, Hijioka S, Mizuno N, Yamao K. A convex EUS is useful to diagnose vascular invasion of cancer, especially hepatic hilus cancer. Dig Endosc. 2011;23 Suppl 1:26–28. doi: 10.1111/j.1443-1661.2011.01137.x. [DOI] [PubMed] [Google Scholar]
- 30.Barclay RL, Perez-Miranda M, Giovannini M. EUS-guided treatment of a solid hepatic metastasis. Gastrointest Endosc. 2002;55:266–270. doi: 10.1067/mge.2002.120784. [DOI] [PubMed] [Google Scholar]
- 31.Hu YH, Tuo XP, Jin ZD, Liu Y, Guo Y, Luo L. Endoscopic ultrasound (EUS)-guided ethanol injection in hepatic metastatic carcinoma: a case report. Endoscopy. 2010;42 Suppl 2:E256–E257. doi: 10.1055/s-0030-1255653. [DOI] [PubMed] [Google Scholar]
- 32.Nakaji S, Hirata N, Iwaki K, Shiratori T, Kobayashi M, Inase M. Endoscopic ultrasound (EUS)-guided ethanol injection for hepatocellular carcinoma difficult to treat with percutaneous local treatment. Endoscopy. 2012;44 Suppl 2 UCTN:E380. doi: 10.1055/s-0032-1309918. [DOI] [PubMed] [Google Scholar]
- 33.DiMaio CJ, Krishnan S, Roayaie S. EUS-guided ethanol ablation for management of metastatic hepatocellular carcinoma. J Intervent Gastroenterol. 2014;4:13–14. [Google Scholar]
- 34.Di Matteo F, Grasso R, Pacella CM, Martino M, Pandolfi M, Rea R, Luppi G, Silvestri S, Zardi E, Costamagna G. EUS-guided Nd: YAG laser ablation of a hepatocellular carcinoma in the caudate lobe. Gastrointest Endosc. 2011;73:632–636. doi: 10.1016/j.gie.2010.08.019. [DOI] [PubMed] [Google Scholar]
- 35.Choi JH, Seo DW, Park do H, Lee SK, Kim MH. Fiducial placement for stereotactic body radiation therapy under only endoscopic ultrasonography guidance in pancreatic and hepatic malignancy: practical feasibility and safety. Gut Liver. 2014;8:88–93. doi: 10.5009/gnl.2014.8.1.88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Karam AR, Connolly C, Fulwadhva U, Hussain S. Alcohol sclerosis of a giant liver cyst following failed deroofings. J Radiol Case Rep. 2011;5:19–22. doi: 10.3941/jrcr.v5i2.634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Saini S, Mueller PR, Ferrucci JT, Simeone JF, Wittenberg J, Butch RJ. Percutaneous aspiration of hepatic cysts does not provide definitive therapy. AJR Am J Roentgenol. 1983;141:559–560. doi: 10.2214/ajr.141.3.559. [DOI] [PubMed] [Google Scholar]
- 38.Bean WJ, Rodan BA. Hepatic cysts: treatment with alcohol. AJR Am J Roentgenol. 1985;144:237–241. doi: 10.2214/ajr.144.2.237. [DOI] [PubMed] [Google Scholar]
- 39.Lee S, Seo DW, Paik WH, Park do H, Lee SS, Lee SK, Kim MH. Ethanol lavage of huge hepatic cysts by using EUS guidance and a percutaneous approach. Gastrointest Endosc. 2014;80:1014–1021. doi: 10.1016/j.gie.2014.03.037. [DOI] [PubMed] [Google Scholar]
- 40.Bertel CK, van Heerden JA, Sheedy PF. Treatment of pyogenic hepatic abscesses. Surgical vs percutaneous drainage. Arch Surg. 1986;121:554–558. doi: 10.1001/archsurg.1986.01400050072009. [DOI] [PubMed] [Google Scholar]
- 41.Bergamini TM, Larson GM, Malangoni MA, Richardson JD. Liver abscess. Review of a 12-year experience. Am Surg. 1987;53:596–599. [PubMed] [Google Scholar]
- 42.Liu CH, Gervais DA, Hahn PF, Arellano RS, Uppot RN, Mueller PR. Percutaneous hepatic abscess drainage: do multiple abscesses or multiloculated abscesses preclude drainage or affect outcome? J Vasc Interv Radiol. 2009;20:1059–1065. doi: 10.1016/j.jvir.2009.04.062. [DOI] [PubMed] [Google Scholar]
- 43.Tazawa J, Sakai Y, Maekawa S, Ishida Y, Maeda M, Marumo F, Sato C. Solitary and multiple pyogenic liver abscesses: characteristics of the patients and efficacy of percutaneous drainage. Am J Gastroenterol. 1997;92:271–274. [PubMed] [Google Scholar]
- 44.Chung YF, Tay KH, Stan B, Htoo AM, Thng CH, Chow PK, Ooi LL, Lau TN. Percutaneous drainage of liver abscess complicated by hepato-venous fistula. Singapore Med J. 2003;44:299–301. [PubMed] [Google Scholar]
- 45.Seewald S, Imazu H, Omar S, Groth S, Seitz U, Brand B, Zhong Y, Sikka S, Thonke F, Soehendra N. EUS-guided drainage of hepatic abscess. Gastrointest Endosc. 2005;61:495–498. doi: 10.1016/s0016-5107(04)02848-2. [DOI] [PubMed] [Google Scholar]
- 46.Noh SH, Park do H, Kim YR, Chun Y, Lee HC, Lee SO, Lee SS, Seo DW, Lee SK, Kim MH. EUS-guided drainage of hepatic abscesses not accessible to percutaneous drainage (with videos) Gastrointest Endosc. 2010;71:1314–1319. doi: 10.1016/j.gie.2009.12.045. [DOI] [PubMed] [Google Scholar]
- 47.Singhal S, Changela K, Lane D, Anand S, Duddempudi S. Endoscopic ultrasound-guided hepatic and perihepatic abscess drainage: an evolving technique. Therap Adv Gastroenterol. 2014;7:93–98. doi: 10.1177/1756283X13506178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Yoshida J, Donahue PE, Nyhus LM. Hemobilia: review of recent experience with a worldwide problem. Am J Gastroenterol. 1987;82:448–453. [PubMed] [Google Scholar]
- 49.Curet P, Baumer R, Roche A, Grellet J, Mercadier M. Hepatic hemobilia of traumatic or iatrogenic origin: recent advances in diagnosis and therapy, review of the literature from 1976 to 1981. World J Surg. 1984;8:2–8. doi: 10.1007/BF01658356. [DOI] [PubMed] [Google Scholar]
- 50.Cattan P, Cuillerier E, Cellier C, Cuenod CA, Roche A, Landi B, Barbier JP. Hemobilia caused by a pseudoaneurysm of the hepatic artery diagnosed by EUS. Gastrointest Endosc. 1999;49:252–255. doi: 10.1016/s0016-5107(99)70497-9. [DOI] [PubMed] [Google Scholar]
- 51.Trakarnsanga A, Sriprayoon T, Akaraviputh T, Tongdee T. Massive hemobilia from a ruptured hepatic artery aneurysm detected by endoscopic ultrasound (EUS) and successfully treated. Endoscopy. 2010;42 Suppl 2:E340–E341. doi: 10.1055/s-0030-1255940. [DOI] [PubMed] [Google Scholar]
- 52.Bloechle C, Izbicki JR, Rashed MY, el-Sefi T, Hosch SB, Knoefel WT, Rogiers X, Broelsch CE. Hemobilia: presentation, diagnosis, and management. Am J Gastroenterol. 1994;89:1537–1540. [PubMed] [Google Scholar]
- 53.Caletti G, Brocchi E, Baraldini M, Ferrari A, Gibilaro M, Barbara L. Assessment of portal hypertension by endoscopic ultrasonography. Gastrointest Endosc. 1990;36:S21–S27. doi: 10.1016/s0016-5107(90)71011-5. [DOI] [PubMed] [Google Scholar]
- 54.Konishi Y, Nakamura T, Kida H, Seno H, Okazaki K, Chiba T. Catheter US probe EUS evaluation of gastric cardia and perigastric vascular structures to predict esophageal variceal recurrence. Gastrointest Endosc. 2002;55:197–203. doi: 10.1067/mge.2002.121338. [DOI] [PubMed] [Google Scholar]
- 55.Choudhuri G, Dhiman RK, Agarwal DK. Endosonographic evaluation of the venous anatomy around the gastro-esophageal junction in patients with portal hypertension. Hepatogastroenterology. 1996;43:1250–1255. [PubMed] [Google Scholar]
- 56.Lee YT, Chan FK, Ching JY, Lai CW, Leung VK, Chung SC, Sung JJ. Diagnosis of gastroesophageal varices and portal collateral venous abnormalities by endosonography in cirrhotic patients. Endoscopy. 2002;34:391–398. doi: 10.1055/s-2002-25286. [DOI] [PubMed] [Google Scholar]
- 57.McKiernan PJ, Sharif K, Gupte GL. The role of endoscopic ultrasound for evaluating portal hypertension in children being assessed for intestinal transplantation. Transplantation. 2008;86:1470–1473. doi: 10.1097/TP.0b013e3181891d63. [DOI] [PubMed] [Google Scholar]
- 58.Irisawa A, Saito A, Obara K, Shibukawa G, Takagi T, Shishido H, Sakamoto H, Sato Y, Kasukawa R. Endoscopic recurrence of esophageal varices is associated with the specific EUS abnormalities: severe periesophageal collateral veins and large perforating veins. Gastrointest Endosc. 2001;53:77–84. doi: 10.1067/mge.2001.108479. [DOI] [PubMed] [Google Scholar]
- 59.Irisawa A, Obara K, Bhutani MS, Saito A, Shishido H, Shibukawa G, Takagi T, Yamamoto G, Seino O, Shishido F, et al. Role of para-esophageal collateral veins in patients with portal hypertension based on the results of endoscopic ultrasonography and liver scintigraphy analysis. J Gastroenterol Hepatol. 2003;18:309–314. doi: 10.1046/j.1440-1746.2003.02956.x. [DOI] [PubMed] [Google Scholar]
- 60.Sato T, Yamazaki K, Toyota J, Karino Y, Ohmura T, Akaike J. Endoscopic ultrasonographic evaluation of hemodynamics related to variceal relapse in esophageal variceal patients. Hepatol Res. 2009;39:126–133. doi: 10.1111/j.1872-034X.2008.00415.x. [DOI] [PubMed] [Google Scholar]
- 61.Kuramochi A, Imazu H, Kakutani H, Uchiyama Y, Hino S, Urashima M. Color Doppler endoscopic ultrasonography in identifying groups at a high-risk of recurrence of esophageal varices after endoscopic treatment. J Gastroenterol. 2007;42:219–224. doi: 10.1007/s00535-006-1992-x. [DOI] [PubMed] [Google Scholar]
- 62.Romero-Castro R, Pellicer-Bautista FJ, Jimenez-Saenz M, Marcos-Sanchez F, Caunedo-Alvarez A, Ortiz-Moyano C, Gomez-Parra M, Herrerias-Gutierrez JM. EUS-guided injection of cyanoacrylate in perforating feeding veins in gastric varices: results in 5 cases. Gastrointest Endosc. 2007;66:402–407. doi: 10.1016/j.gie.2007.03.008. [DOI] [PubMed] [Google Scholar]
- 63.Romero-Castro R, Ellrichmann M, Ortiz-Moyano C, Subtil-Inigo JC, Junquera-Florez F, Gornals JB, Repiso-Ortega A, Vila-Costas J, Marcos-Sanchez F, Muñoz-Navas M, et al. EUS-guided coil versus cyanoacrylate therapy for the treatment of gastric varices: a multicenter study (with videos) Gastrointest Endosc. 2013;78:711–721. doi: 10.1016/j.gie.2013.05.009. [DOI] [PubMed] [Google Scholar]
- 64.de Paulo GA, Ardengh JC, Nakao FS, Ferrari AP. Treatment of esophageal varices: a randomized controlled trial comparing endoscopic sclerotherapy and EUS-guided sclerotherapy of esophageal collateral veins. Gastrointest Endosc. 2006;63:396–402; quiz 463. doi: 10.1016/j.gie.2005.10.039. [DOI] [PubMed] [Google Scholar]
- 65.Rösch J, Hanafee WN, Snow H. Transjugular portal venography and radiologic portacaval shunt: an experimental study. Radiology. 1969;92:1112–1114. doi: 10.1148/92.5.1112. [DOI] [PubMed] [Google Scholar]
- 66.Colombato L. The role of transjugular intrahepatic portosystemic shunt (TIPS) in the management of portal hypertension. J Clin Gastroenterol. 2007;41 Suppl 3:S344–S351. doi: 10.1097/MCG.0b013e318157e500. [DOI] [PubMed] [Google Scholar]
- 67.Wong F. The use of TIPS in chronic liver disease. Ann Hepatol. 2006;5:5–15. [PubMed] [Google Scholar]
- 68.Lai L, Poneros J, Santilli J, Brugge W. EUS-guided portal vein catheterization and pressure measurement in an animal model: a pilot study of feasibility. Gastrointest Endosc. 2004;59:280–283. doi: 10.1016/s0016-5107(03)02544-6. [DOI] [PubMed] [Google Scholar]
- 69.Giday SA, Ko CW, Clarke JO, Shin EJ, Magno P, Jagannath SB, Buscaglia JM, Kantsevoy SV. EUS-guided portal vein carbon dioxide angiography: a pilot study in a porcine model. Gastrointest Endosc. 2007;66:814–819. doi: 10.1016/j.gie.2007.05.056. [DOI] [PubMed] [Google Scholar]
- 70.Giday SA, Clarke JO, Buscaglia JM, Shin EJ, Ko CW, Magno P, Kantsevoy SV. EUS-guided portal vein catheterization: a promising novel approach for portal angiography and portal vein pressure measurements. Gastrointest Endosc. 2008;67:338–342. doi: 10.1016/j.gie.2007.08.037. [DOI] [PubMed] [Google Scholar]
- 71.Buscaglia JM, Dray X, Shin EJ, Magno P, Chmura KM, Surti VC, Dillon TE, Ducharme RW, Donatelli G, Thuluvath PJ, et al. A new alternative for a transjugular intrahepatic portosystemic shunt: EUS-guided creation of an intrahepatic portosystemic shunt (with video) Gastrointest Endosc. 2009;69:941–947. doi: 10.1016/j.gie.2008.09.051. [DOI] [PubMed] [Google Scholar]
- 72.Bureau C, Pagan JC, Layrargues GP, Metivier S, Bellot P, Perreault P, Otal P, Abraldes JG, Peron JM, Rousseau H, Bosch J, Vinel JP. Patency of stents covered with polytetrafluoroethylene in patients treated by transjugular intrahepatic portosystemic shunts: long-term results of a randomized multicentre study. Liver Int. 2007;27:742–747. doi: 10.1111/j.1478-3231.2007.01522.x. [DOI] [PubMed] [Google Scholar]
- 73.Clark TW, Agarwal R, Haskal ZJ, Stavropoulos SW. The effect of initial shunt outflow position on patency of transjugular intrahepatic portosystemic shunts. J Vasc Interv Radiol. 2004;15:147–152. doi: 10.1097/01.rvi.0000109401.52762.56. [DOI] [PubMed] [Google Scholar]
- 74.Bedossa P, Dargère D, Paradis V. Sampling variability of liver fibrosis in chronic hepatitis C. Hepatology. 2003;38:1449–1457. doi: 10.1016/j.hep.2003.09.022. [DOI] [PubMed] [Google Scholar]
- 75.Cadranel JF, Rufat P, Degos F. Practices of liver biopsy in France: results of a prospective nationwide survey. For the Group of Epidemiology of the French Association for the Study of the Liver (AFEF) Hepatology. 2000;32:477–481. doi: 10.1053/jhep.2000.16602. [DOI] [PubMed] [Google Scholar]
- 76.Albanis E, Friedman SL. Diagnosis of hepatic fibrosis in patients with chronic hepatitis C. Clin Liver Dis. 2006;10:821–833. doi: 10.1016/j.cld.2006.08.027. [DOI] [PubMed] [Google Scholar]
- 77.Wells RG. The role of matrix stiffness in hepatic stellate cell activation and liver fibrosis. J Clin Gastroenterol. 2005;39:S158–S161. doi: 10.1097/01.mcg.0000155516.02468.0f. [DOI] [PubMed] [Google Scholar]
- 78.Rimbaş M, Gheonea DI, Săndulescu L, Săftoiu A, Vilmann P, Ciurea T. EUS Elastography in Evaluating Chronic Liver Disease. Why not from Inside? Curr Health Sci J. 2009;35:225–227. [PMC free article] [PubMed] [Google Scholar]
- 79.Hemming AW, Reed AI, Howard RJ, Fujita S, Hochwald SN, Caridi JG, Hawkins IF, Vauthey JN. Preoperative portal vein embolization for extended hepatectomy. Ann Surg. 2003;237:686–691; discussion 691-693. doi: 10.1097/01.SLA.0000065265.16728.C0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Liu H, Fu Y. Portal vein embolization before major hepatectomy. World J Gastroenterol. 2005;11:2051–2054. doi: 10.3748/wjg.v11.i14.2051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Matthes K, Sahani D, Holalkere NS, Mino-Kenudson M, Brugge WR. Feasibility of endoscopic ultrasound-guided portal vein embolization with Enteryx. Acta Gastroenterol Belg. 2005;68:412–415. [PubMed] [Google Scholar]
- 82.Winick AB, Waybill PN, Venbrux AC. Complications of percutaneous transhepatic biliary interventions. Tech Vasc Interv Radiol. 2001;4:200–206. doi: 10.1016/s1089-2516(01)90026-5. [DOI] [PubMed] [Google Scholar]
- 83.Giovannini M, Dotti M, Bories E, Moutardier V, Pesenti C, Danisi C, Delpero JR. Hepaticogastrostomy by echo-endoscopy as a palliative treatment in a patient with metastatic biliary obstruction. Endoscopy. 2003;35:1076–1078. doi: 10.1055/s-2003-44596. [DOI] [PubMed] [Google Scholar]
- 84.Kahaleh M, Yoshida C, Kane L, Yeaton P. Interventional EUS cholangiography: A report of five cases. Gastrointest Endosc. 2004;60:138–142. doi: 10.1016/s0016-5107(04)01528-7. [DOI] [PubMed] [Google Scholar]
- 85.Püspök A, Lomoschitz F, Dejaco C, Hejna M, Sautner T, Gangl A. Endoscopic ultrasound guided therapy of benign and malignant biliary obstruction: a case series. Am J Gastroenterol. 2005;100:1743–1747. doi: 10.1111/j.1572-0241.2005.41806.x. [DOI] [PubMed] [Google Scholar]
- 86.Bories E, Pesenti C, Caillol F, Lopes C, Giovannini M. Transgastric endoscopic ultrasonography-guided biliary drainage: results of a pilot study. Endoscopy. 2007;39:287–291. doi: 10.1055/s-2007-966212. [DOI] [PubMed] [Google Scholar]
- 87.Panpimanmas S, Ratanachu-ek T. Endoscopic ultrasound-guided hepaticogastrostomy for hilar cholangiocarcinoma: the first trial in Thailand. J Med Assoc Thai. 2011;94 Suppl 2:S129–S134. [PubMed] [Google Scholar]
- 88.Giovannini M, Bories E. EUS-Guided Biliary Drainage. Gastroenterol Res Pract. 2012;2012:348719. doi: 10.1155/2012/348719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Sarkaria S, Lee HS, Gaidhane M, Kahaleh M. Advances in endoscopic ultrasound-guided biliary drainage: a comprehensive review. Gut Liver. 2013;7:129–136. doi: 10.5009/gnl.2013.7.2.129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Itoi T, Sofuni A, Itokawa F, Tsuchiya T, Kurihara T, Ishii K, Tsuji S, Ikeuchi N, Umeda J, Moriyasu F, et al. Endoscopic ultrasonography-guided biliary drainage. J Hepatobiliary Pancreat Sci. 2010;17:611–616. doi: 10.1007/s00534-009-0196-1. [DOI] [PubMed] [Google Scholar]
- 91.Kawakubo K, Isayama H, Kato H, Itoi T, Kawakami H, Hanada K, Ishiwatari H, Yasuda I, Kawamoto H, Itokawa F, et al. Multicenter retrospective study of endoscopic ultrasound-guided biliary drainage for malignant biliary obstruction in Japan. J Hepatobiliary Pancreat Sci. 2014;21:328–334. doi: 10.1002/jhbp.27. [DOI] [PubMed] [Google Scholar]
- 92.Ogura T, Masuda D, Imoto A, Takeushi T, Kamiyama R, Mohamed M, Umegaki E, Higuchi K. EUS-guided hepaticogastrostomy combined with fine-gauge antegrade stenting: a pilot study. Endoscopy. 2014;46:416–421. doi: 10.1055/s-0034-1365020. [DOI] [PubMed] [Google Scholar]
- 93.Ogura T, Kurisu Y, Masuda D, Imoto A, Hayashi M, Malak M, Umegaki E, Uchiyama K, Higuchi K. Novel method of endoscopic ultrasound-guided hepaticogastrostomy to prevent stent dysfunction. J Gastroenterol Hepatol. 2014;29:1815–1821. doi: 10.1111/jgh.12598. [DOI] [PubMed] [Google Scholar]
- 94.Ogura T, Masuda D, Imoto A, Umegaki E, Higuchi K. EUS-guided hepaticogastrostomy for hepatic hilar obstruction. Endoscopy. 2014;46 Suppl 1 UCTN:E32–E33. doi: 10.1055/s-0033-1359133. [DOI] [PubMed] [Google Scholar]
- 95.Kawakubo K, Isayama H, Sasahira N, Nakai Y, Kogure H, Hamada T, Miyabayashi K, Mizuno S, Sasaki T, Ito Y, et al. Clinical utility of an endoscopic ultrasound-guided rendezvous technique via various approach routes. Surg Endosc. 2013;27:3437–3443. doi: 10.1007/s00464-013-2896-5. [DOI] [PubMed] [Google Scholar]
- 96.Mallery S, Matlock J, Freeman ML. EUS-guided rendezvous drainage of obstructed biliary and pancreatic ducts: Report of 6 cases. Gastrointest Endosc. 2004;59:100–107. doi: 10.1016/s0016-5107(03)02300-9. [DOI] [PubMed] [Google Scholar]
- 97.Maranki J, Hernandez AJ, Arslan B, Jaffan AA, Angle JF, Shami VM, Kahaleh M. Interventional endoscopic ultrasound-guided cholangiography: long-term experience of an emerging alternative to percutaneous transhepatic cholangiography. Endoscopy. 2009;41:532–538. doi: 10.1055/s-0029-1214712. [DOI] [PubMed] [Google Scholar]
- 98.Iwashita T, Lee JG, Shinoura S, Nakai Y, Park DH, Muthusamy VR, Chang KJ. Endoscopic ultrasound-guided rendezvous for biliary access after failed cannulation. Endoscopy. 2012;44:60–65. doi: 10.1055/s-0030-1256871. [DOI] [PubMed] [Google Scholar]
- 99.Dhir V, Bhandari S, Bapat M, Maydeo A. Comparison of EUS-guided rendezvous and precut papillotomy techniques for biliary access (with videos) Gastrointest Endosc. 2012;75:354–359. doi: 10.1016/j.gie.2011.07.075. [DOI] [PubMed] [Google Scholar]
- 100.Itoi T, Sofuni A, Tsuchiya T, Ijima M, Iwashita T. Endoscopic ultrasonography-guided transhepatic antegrade stone removal in patients with surgically altered anatomy: case series and technical review (with videos) J Hepatobiliary Pancreat Sci. 2014;21:E86–E93. doi: 10.1002/jhbp.165. [DOI] [PubMed] [Google Scholar]
- 101.Park do H, Jang JW, Lee SS, Seo DW, Lee SK, Kim MH. EUS-guided transhepatic antegrade balloon dilation for benign bilioenteric anastomotic strictures in a patient with hepaticojejunostomy. Gastrointest Endosc. 2012;75:692–693. doi: 10.1016/j.gie.2011.04.013. [DOI] [PubMed] [Google Scholar]
- 102.Park do H, Jeong SU, Lee BU, Lee SS, Seo DW, Lee SK, Kim MH. Prospective evaluation of a treatment algorithm with enhanced guidewire manipulation protocol for EUS-guided biliary drainage after failed ERCP (with video) Gastrointest Endosc. 2013;78:91–101. doi: 10.1016/j.gie.2013.01.042. [DOI] [PubMed] [Google Scholar]
- 103.Shah JN, Marson F, Weilert F, Bhat YM, Nguyen-Tang T, Shaw RE, Binmoeller KF. Single-operator, single-session EUS-guided anterograde cholangiopancreatography in failed ERCP or inaccessible papilla. Gastrointest Endosc. 2012;75:56–64. doi: 10.1016/j.gie.2011.08.032. [DOI] [PubMed] [Google Scholar]
- 104.Park SJ, Choi JH, Park do H, Choi JH, Lee SS, Seo DW, Lee SK, Kim MH. Expanding indication: EUS-guided hepaticoduodenostomy for isolated right intrahepatic duct obstruction (with video) Gastrointest Endosc. 2013;78:374–380. doi: 10.1016/j.gie.2013.04.183. [DOI] [PubMed] [Google Scholar]
- 105.McGrath K, Brody D, Luketich J, Khalid A. Detection of unsuspected left hepatic lobe metastases during EUS staging of cancer of the esophagus and cardia. Am J Gastroenterol. 2006;101:1742–1746. doi: 10.1111/j.1572-0241.2006.00665.x. [DOI] [PubMed] [Google Scholar]
- 106.Singh P, Mukhopadhyay P, Bhatt B, Patel T, Kiss A, Gupta R, Bhat S, Erickson RA. Endoscopic ultrasound versus CT scan for detection of the metastases to the liver: results of a prospective comparative study. J Clin Gastroenterol. 2009;43:367–373. doi: 10.1097/MCG.0b013e318167b8cc. [DOI] [PubMed] [Google Scholar]