

Abstract
Objective: To estimate the feasibility and safety of single-incision multiport laparoscopy (SIMPL) used in patients who underwent laparoendoscopic single-site surgery (LESS) for gynecologic disease, and the cosmetic outcome and economic benefit compared with multichannel-tipped single port laparoscopy (MSPL). Intervention: We underwent LESS via a single 2.5- to 3.0-cm umbilical incision with the Single-Incision Multiport Laparoscopic Surgery Trocar available on the market, briefly named MSPL. Since January 2014, we improved the procedure and named SIMPL. In SIMPL group, two traditional laparoscopic trocar (diameter=5 mm) and one mini-laparoscopic trocar (diameter =3 mm) were inserted into the peritoneum separately through a single 1.5- to 1.8-cm umbilical transcutaneous incision. Subject demographics and clinical variables were collected and perioperative outcomes analyzed. In addition, the size of umbilicus was measured in all patients prior to the operation and the levels of cosmetic satisfaction were evaluated at 4 weeks after surgery. Measurements and main results: From January 2014 to December 2014, there were 32 patients who underwent SIMPL for ovarian cystectomy. Hospital cost was significantly lower in SIMPL group compared with MSPL group (RMB 10207.0 vs 17973.7 yuan), P<0.001. Compared with MSPL group, the SIMPL group reported significantly higher cosmetic satisfaction at 4 weeks afer surgery (P<0.1). Besides, the SIMPL procedures performed in benign gynecologic surgery were myomectomy (n=8), salpingpoophorectomy (n=2), salpingectomy (n=5), adhesiolysis and fimbrioplasty (n=32), ovarian drilling (n=3), salpingotomy for ectopic pregnancy (n=3). All surgeries were completed successfully without conversion to the traditional laparoscopic approach. Two postoperative complications occurred were delay healing of umbilicus incision after myomectomy. The cosmetic satisfactory rate was 100%. Conclusion: According to our experience, SIMPL is safe and efficient for simple gynecologic operation, with lower cost and better cosmetic results than MSPL. Beyond cosmetic and economic results, further randomized studies are needed to identify a possible benefit.
Keywords: Laparoendoscopic single-site surgery (LESS), multichannel-tipped single port laparoscopy (MSPL), single-incision multiport laparoscopy (SIMPL), benign gynecologic disease
Introduction
Minimally invasive gynecologic surgery is evolving continuously for treating gynecologic diseases. With the minimum postoperative scar concealed within the umbilicus, laparoendoscopic single-site surgery (LESS) has an advantage insofar as cosmetic outcome compared with conventional laparoscopy [1]. However, a meta-analysis of randomized controlled trials provides evidence that LESS can be a feasible and safe approach to effective management of benign and malignant gynecological diseases, but not offer the advantage such as better cosmesis and lesser pain [2]. In current clinical trials, most gynecologists underwent surgery via a single 1.5- to 2.5-cm umbilical incision with a multichannel-tipped single port (MSP) access device [3-5]. Actually, the cosmetic result of LESS is dependent on the size of each particular patient’s umbilicus and the surgeon’s capacity to “hide” the incision. Our measurements show that the average preoperative sizes of umbilicus are smaller than the diameter of MSP. This result may be the distinguishing issue to explain the dissatisfied cosmetic outcome of most LESS [2]. In this study, the gynecological procedures were improved using single-incision multiport laparoscopy (SIMPL) and the aim is to assess the benefits and costs of SIMPL compared with MSPL approaches.
Materials and methods
This was conducted at our department (Obstetrics and Gynecology Hospital of Fudan University, Shanghai, China), which is a retrospective study. All LESS procedures were performed by a senior gynecologic laparoscopist. Considering the surgeon’s learning curve for LESS, we collected the data after about 30 LESS procedures were performed. Of all patients who underwent LESS for these two procedures mentioned later, the clinical data between January 2013 and December 2014 were collected and analyzed. And, we focused on the patients with indications of ovarian cyst enucleation or myomectomy.
Data collection
The details of the following parameters were retrieved for all surgery of interest: the patient basal characteristics (i.e., age, body mass index, the size of umbilicus, number and size of myoma, and type of the largest myoma), the operative time, hemoglobin change, degree of cosmetic satisfaction (assessed by visual analog scale at 1 day and 4 weeks after surgery), hospital stay and hospital cost.
Surgical procedures
Operations were administrated under general anesthesia, with a Trendelenburg position of 25 to 30 degrees, arms along the body, legs slightly apart, a flow rate 6 L/min and intra-abdominal CO2 pressure 14 mmHg. With bidirectional barb, the absorbable suture was used to repair ovary or uterus.
The device was removed at the end of the surgical procedures, then the umbilical incision was closed in some layers, including peritoneum, anadesma, subcutaneous tissue, and subcuticular layer, using reabsorbable sutures.
Multichannel-tipped single port laparoscopy (MSPL)
The Single-Incision Multiport Laparoscopic Surgery Trocar (Innovex Medical Co.,Ltd.) was administrated for MSPL. This special trocar was placed at the umbilical level, or more laterally. Located within or underneath the umbilicus, a skin incision about 2.5 to 3 cm was performed (Figure 1). Then, after that rectus sheath and peritoneum were incised vertically for 3 to 4 cm, this special trocar with 4 dedicated trocars (1 for flexible laparoscope and 3 as working ports) was set up. Flexible and straight laparoscopic instruments were used as needed.
Figure 1.

MSPL Trocar (Innovex Medical C0., Ltd.).
Single-incision multiport laparoscopy (SIMPL)
In SIMPL group, three trocars were inserted into the peritoneum separately through a single 1.5- to 1.8-cm umbilical transcutaneous incision (Figure 2), namely two traditional laparoscopic trocar (1 for flexible camera and another as mainly working port) and one mini-laparoscopic 3-mm trocar as ancillary working port. By use of triangle arrangement and curved or articulating laparoscopic instrument, the surgeons performed the operation without hand collision externally. Besides, the flexible instrument allowed for recreation of triangulation at the procedure, which is the basic surgical technique including traction-countertraction and intricate dissection. In myomectomy procedure, after striping myoma and suturing the uterus wound, the two working trocars were replaced by a 10-mm trocar for myoma retrieval by a disintegrator. The similar procedures were done in ovarian cystectomy, while the difference was specimen retrieved by the endoscopic bag.
Figure 2.

Single-Incision Multiport for SIMPL.
Data analysis
Group differences were tested using the Independent-Sample T test; and the Mann-Whitney U Test was used to test the variables that were not normally distributed. A P-value of less than 0.05 was considered significant statistically.
Results
The relative comparative data of ovarian cystectomy in the MSPL and SIMPL group respectively are reported in Table 1. From the MSPL group (n=11) and the SIMPL group (n=32), the characteristics of the patients were as follow: age, 25.4 years versus 28.6 years (non-significant [NS]); body mass index, 22.0 versus 21.9 kg/m2 (NS); and preoperative size of umbilicus, vertical diameter, 15.69 versus 14.78 cm (NS); horizontal diameter, 11.33 versus 10.37 cm (NS); depth, 10.69 versus 9.68 cm (NS). The two groups were similar for indications. The pathologic diagnoses were confirmed as mature cystic teratoma (n=6 and 13), endometriosis (n=3 and 12), mucinous cystadenoma (n=1 and 4), serous cystadenoma (n=1 and 3) in the MSPL group and the SIMPL group separately. Hospital cost was significantly lower in SIMPL group compared with MSPL group (RMB 10207.0 vs 17973.7 yuan), P<0.001. The SIMPL group reported significantly higher cosmetic satisfaction (100%) compared with MSPL group (63.6%) at 4 weeks after surgery. No intraoperative and postoperative complications were reported in both 2 groups.
Table 1.
Patient characteristics and outcomes in ovarian cystectomy: MSPL versus SIMPL
| Characteristics | MSPL (n=11) | SIMPL (n=32) | |
|---|---|---|---|
| Age, mean (SD), y | 25.4 (5.5) | 28.6 (56.1) | t: 0.140 |
| Body mass index, mean (SD), kg/m2 | 22.0 (2.0) | 21.9 (1.7) | t: 0.894 |
| Preoperative size of umbilicus, mean (SD), cm | |||
| Vertical diameter | 15.69 (2.19) | 14.78 (2.42) | t: 0.280 |
| Horizontal diameter | 11.33 (2.75) | 10.37 (2.28) | t: 0.259 |
| Depth | 10.69 (2.80) | 9.68 (2.91) | t: 0.323 |
| Indications: Suspicious ovarian mass (pathologic diagnoses) | 11 | 32 | |
| Mature cystic teratoma | 6 (54.5%) | 13 (40.6%) | |
| Endometriosis | 3 (27.3%) | 12 (37.5%) | |
| Mucinous cystadenoma | 1 (9.1%) | 4 (12.5%) | |
| Serous cystadenoma | 1 (9.1%) | 3 (9.4%) | |
| Operative time, Mean (SD), min | 60 (26) | 62 (29) | t: 0.786 |
| Operative time, Median (extremes), min | 50 (35-115) | 54 (20-140) | |
| Operation failures | 0/11 | 0/32 | |
| Hospital stay, Median (extremes), night | 3.27 (3-4) | 3.4 (2-7) | U: 0.612 |
| Hospital cost, Mean (SD), RMB yuan | 17973.7 (1343.4) | 10207.0 (1060.9) | t: <10^-4 |
| Hemoglobin change, Mean (SD), g/L | 12.1 (4.6) | 7.7 (7.1) | t: 0.064 |
| Intraoperative complications | 0/11 | 0/32 | |
| Late postoperative complications | 0/11 | 0/32 | |
| Cosmetic satisfaction rate | 63.6% (7/11) | 100% (32/32) |
t, Independent-Samples T Test. U, Mann-Whitney U Test.
Operative time, procedure failures, hospital stay or cost, hemoglobin change, intraoperative and postoperative complications, and cosmetic satisfaction rate for SIMPL in benign gynecologic surgery are reported in Table 2. There was no case conversion from SIMPL to conventional multiport laparoscopy, no intraoperative complications occurred. We detected 2 cases that delay wound healing in the umbilical incision, in the SIMPL myomectomy group. The cosmetic satisfaction rate was 100%.
Table 2.
Perioperative outcomes for SIMPL in benign Gynecological surgery
| Myomectomy (n=8) | Ovarian cystectomy (n=32) | salpingpoophorectomy (n=2) | Salpingectomy (n=5) | Adhesiolysis and fimbrioplasty (n=32) | ovarian drilling (n=3) | salpingotomy for ectopic pregnancy (n=3) | |
|---|---|---|---|---|---|---|---|
| Operative time, min | |||||||
| Mean (SD) | 105 (38) | 62 (29) | 33 (16) | 41 (14) | 46 (23) | 34 (14) | 36 (6) |
| Median (extremes) | 96 (52-162) | 54 (20-140) | 33 (21-45) | 47 (20-55) | 38 (20-100) | 35 (20-47) | 38 (24-39) |
| Additional port (2-mm) | 0/8 | 0/32 | 0/2 | 0/5 | 32/32 | 0/3 | 0/6 |
| Hospital stay, Median (extremes), night | 3.7 (3-6) | 3.4 (2-7) | 2.5 (2-3) | 3.0 (2-3) | 3.0 (2-5) | 3.0 (2-3) | 4.0 (4-5) |
| Hospital cost, Mean (SD), RMB yuan | 10797.6 (797.9) | 10207.0 (1060.9) | 9160.0 (233.3) | 11475.0 (1592.0) | 11156.2 (1618.9) | 10532.3 (1313.6) | 9924.7 (135.7) |
| Hemoglobin change, Mean (SD), g/L | 11.5 (11.2) | 7.7 (7.1) | 12.0 (4.2) | 8.0 (4.8) | 5.2 (7.4) | 6.0 (5.2) | 9.3 (3.3) |
| Intraoperative complications | 0/8 | 0/32 | 0/2 | 0/5 | 0/32 | 0/3 | 0/6 |
| Postoperative complications | 2/8* | 0/32 | 0/2 | 0/5 | 0/32 | 0/3 | 0/6 |
| Cosmetic satisfaction rate | 100% | 100% | 100% | 100% | 100% | 100% | 100% |
| Tumor size, cm | |||||||
| Mean (SD) | 5.6 (2.1) | 5.7 (1.9) | 5.5 (0.7) | 3.4 (0.5) | NA | 4.0 (0) | 3.8 (0.9) |
| Median (extremes) | 5.6 (2-8) | 5.5 (2-10) | 5.5 (5-6) | 3.0 (3-4) | NA | 4.0 (4-4) | 4.0 (3-6) |
delay healing of umbilicus incision.
NA: not available.
Discussion
Our statistical statement show that the hospital cost was significantly lower for cystectomy surgery performed by SIMPL compared with MSPL. Obviously, the economic advantage of SIMPL should owe to avoid using of the Single-Incision Multiport Laparoscopic Surgery Trocar (Innovex Medical C0., Ltd.) which is one-off and will cost about 7000 to 8000 RMB in China.
Meanwhile, the MSP device requires a bigger incision and always leaves a visible scar (Figure 3), namely the postoperative cosmetic results were not satisfied as SIMPL surgery (Figure 4), and it took the surgeon more time to conceal the umbilicus incision.
Figure 3.

Postoperative Scar of MSPL.
Figure 4.

Postoperative Scar of SIMPL.
Our studies have indicated the feasibility and safety of SIMPL and MSPL, but a potential bias may exist in our results. Absolutely, in consideration of patient cosmetic requirement, we increasingly tend to select younger patients without previous surgeries to perform LESS. So, adhesiolysis of severe pelvic adhesion did not occur in out procedures, neither intraoperative complications were encountered. On the other hand, patients suspected to suffer malignant gynecological diseases were excluded. So, there was no case conversion from LESS to conventional surgery because of pathologic diagnosed malignant tumor during the operation. It may be possible to consider the safety and benefit in another randomized controlled large sample analysis. As reported, laparoendoscopic single-site surgery radical hysterectomy (LESS-RH) and pelvic lymphadenectomy (PLND) are feasible and safe for select patients with stage I cervical cancer, but the operation time was not mentioned [6]. And another article reported the first case of LESS for endometrial cancer in China, using a single multiple-channel port (Tri-port) inserted through a 2.5 cm upper umbilicus incision. The duration of the LESS procedure was 4.0 h, and the establishment of the operative access took 1.0 h [7].
We also suggest that several tricks and tips, which can contribute to the easier procedure, should be used for SIMPL.
During the procedure, maintenance of pneumoperitoneum is one of the challenges of LESS. Surgeons attempted to overcome the difficulties. As reported, a surgical glove over an Alexis Wound Retractor was applied by Lee, Y.Y. et al. The holes were cut on the glove fingers, through which any desired laparoscopic port was placed [8]. Takeda, A. et al. reported their experience with isobaric (gasless) transumbilical LESS surgery for adnexal tumors. The key point was the transumbilical wound retraction system combined with the subcutaneous abdominal wall-lift method contributed to create a wide and flexible orifice during instrumentation [9,10]. Kim, W.C. et al used a homemade wound retractor and surgical glove as the single-port device, their initial experience for treatment of adnexal tumors was feasible and safe [11]. Our creative adaptation was the use of a transformed endotracheal tube as necessary (Figure 5). The balloon part of the tube was cut down then put onto the conventional 5-mm trocar as an external element (Figure 6). The balloon could be adjusted by Inflating or deflating to maintain the pneumoperitoneum.
Figure 5.

Endotracheal Tube.
Figure 6.
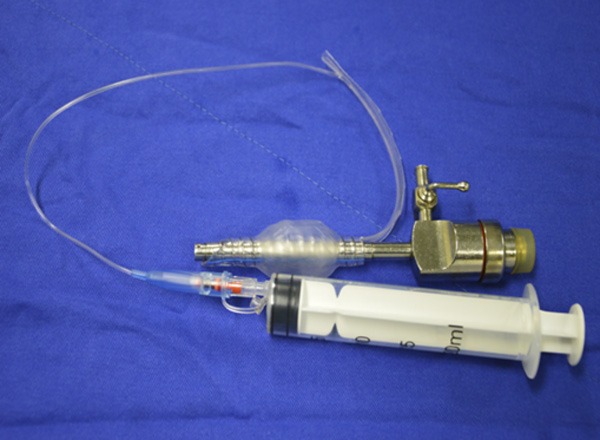
The balloon part of the endotracheal tube as an external element.
In addition, the knot-tying process for intracorporeal suturing during LESS is a major limiting step and a key determinant of the popularity of LESS. In myomectomy procedure, using of absorbable sutures with barbs solved the problem. According to our experience of both LESS and conventional laparoscopy, uterine wound closure was recommended to carry out twice, the first full-thickness continuous suture, the second seromuscular inverting suture patterns. Retrorse barbs ensured the tension without knot. But in fimbrioplasty, the suture with barbs was not suitable. For balancing operation time and cosmetic outcome, a 2-mm additional port was needed, which made suture and knot-tying process in LESS as easy as conventional laparoscopy, the detail will be discussed in another article.
Our procedure provided another option to prevent hand collision and recreat triangulation which is necessary in the operation. Two operating apparatus underwent surgery by up-and-down or left-and-right motion just like Chinese chopsticks. Our experience indicated that one traditional straight instrument and another flexional apparatus could make the operation easier and faster than two curved laparoscopic equipment. The surgeon adjusted only one articulating instrument in the procedure, which may shorten the operation time and learning curve.
Conclusion
Single-incision multiport laparoscopy (SIMPL) is a feasible, safe technique administrated for numerous gynecologic surgeries, such as myomectomy, cystectomy, salping-oophorectomy, salpingectomy, salpingotomy for ectopic pregnancy, adhesiolysis, fimbrioplasty for infertility and ovarian drilling procedure. SIMPL seems have more advantage in cosmetic and economic outcomes compared with MSPL in cystectomy. For surgeons, SIMPL provides another option to undergoing LESS procedure in gynecology. Proper instrument, satisfactory maintenance of pneumoperitoneum, recreation of triangulation and collision avoidance of hand may play role in the satisfying surgical procedures. In the future, the available instrument and development of the technique will allow an increasingly various patient population to apply LESS.
Disclosure of conflict of interest
None.
References
- 1.Yeung PP Jr, Bolden CR, Westreich D, Sobolewski C. Patient preferences of cosmesis for abdominal incisions in gynecologic surgery. J Minim Invasive Gynecol. 2013;20:79–84. doi: 10.1016/j.jmig.2012.09.008. [DOI] [PubMed] [Google Scholar]
- 2.Song T, Kim ML, Jung YW, Yoon BS, Joo WD, Seong SJ. Laparoendoscopic single-site versus conventional laparoscopic gynecologic surgery: a metaanalysis of randomized controlled trials. Am J Obstet Gynecol. 2013;209:317–319. doi: 10.1016/j.ajog.2013.07.004. [DOI] [PubMed] [Google Scholar]
- 3.Fader AN, Rojas-Espaillat L, Ibeanu O, Grumbine FC, Escobar PF. Laparoendoscopic single-site surgery (LESS) in gynecology: a multi-institutional evaluation. Am J Obstet Gynecol. 2010;203:501–506. doi: 10.1016/j.ajog.2010.06.028. [DOI] [PubMed] [Google Scholar]
- 4.Bedaiwy MA, Farghaly T, Hurd W, Liu J, Mansour G, Fader AN, Escobar P. Laparoendoscopic single-site surgery for management of ovarian endometriomas. JSLS. 2014;18:191–196. doi: 10.4293/108680813X13794522666284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Takeda A, Imoto S, Mori M, Nakano T, Nakamura H. Isobaric laparoendoscopic singlesite surgery with wound retractor for adnexal tumors: a single center experience with the initial 100 cases. Eur J Obstet Gynecol Reprod Biol. 2011;157:190–196. doi: 10.1016/j.ejogrb.2011.02.018. [DOI] [PubMed] [Google Scholar]
- 6.Boruta DM, Fagotti A, Bradford LS, Escobar PF, Scambia G, Kushnir CL, Michener CM, Fader AN. Laparoendoscopic single-site radical hysterectomy with pelvic lymphadenectomy: initial multi-institutional experience for treatment of invasive cervical cancer. J Minim Invasive Gynecol. 2014;21:394–398. doi: 10.1016/j.jmig.2013.10.005. [DOI] [PubMed] [Google Scholar]
- 7.Liu MB, Cai HH. Laparoendoscopic singlesite surgery for gynecologic malignancy: the first report in China. Nan Fang Yi Ke Da Xue Xue Bao. 2011;31:1619–1621. [PubMed] [Google Scholar]
- 8.Yang YS, Oh KY, Hur MH, Kim SY, Yim HS. Laparoendoscopic Single-Site Surgery Using Conventional Laparoscopic Instruments and Glove Port Technique in Gynecology: A Single Surgeon’s Experience. J Minim Invasive Gynecol. 2015;22:87–93. doi: 10.1016/j.jmig.2014.07.013. [DOI] [PubMed] [Google Scholar]
- 9.Takeda A, Imoto S, Mori M, Nakano T, Nakamura H. Wound retraction system for isobaric laparoendoscopic single-site surgery to treat adnexal tumors: pilot study. J Minim Invasive Gynecol. 2010;17:626–630. doi: 10.1016/j.jmig.2010.02.003. [DOI] [PubMed] [Google Scholar]
- 10.Takeda A, Imoto S, Mori M, Nakano T, Nakamura H. Isobaric laparoendoscopic singlesite surgery with wound retractor for adnexal tumors: a single center experience with the initial 100 cases. Eur J Obstet Gynecol Reprod Biol. 2011;157:190–196. doi: 10.1016/j.ejogrb.2011.02.018. [DOI] [PubMed] [Google Scholar]
- 11.Kim WC, Lee JE, Kwon YS, Koo YJ, Lee IH, Lim KT. Laparoendoscopic single-site surgery (LESS) for adnexal tumors: one surgeon’s initial experience over a one-year period. Eur J Obstet Gynecol Reprod Biol. 2011;158:265–268. doi: 10.1016/j.ejogrb.2011.04.020. [DOI] [PubMed] [Google Scholar]