

Abstract
Objective: The Cycle of Willis unites the internal carotid and vertebrobasilar system and maintains the stability of blood supply to the brain. This present study aims to analyze the anatomic variations in the anterior part of the Cycle of Willis. Methods: Forty five formalin-preserved human brains (90 cerebral hemispheres) with intact dura mater from Chinese adults were dissected under the surgical microscope. The anterior components of the Circle of Willis were observed and measured. Anatomic variations of this segment were observed and photographed. The data collected in this investigation was statistically analyzed. Results: In approximately 13.3% (6/45) of all cerebral samples, a caliber difference of ≥ 0.5 mm was noted between the left A1 and the right segments. The A2 segments of left and right hemispheres were derived from the contralateral A1 segment in 6.7% (3/45) of the brain specimens. Simple anterior communicating artery (ACoA) was observed in 37.8% (17/45) whereas complex ACoA was noted in 60% (27/45) of cerebral samples. Conclusion: As it demonstrates the anatomic variations of ACAC, all surgical approaches should be performed after angiographic demonstrations. Understanding of these anatomic variations plays a pivotal role in neurovascular procedures.
Keywords: Circle of Willis, anterior circulation, microanatomy, variation
Introduction
The Circle of Willis is a circulatory anastomosis that supplies blood to the brain and surrounding structures. It consists of the following arteries including anterior cerebral, anterior communicating, internal carotid, posterior cerebral and posterior communicating arteries [1]. The anterior portion of the Circle of Willis is composed of the terminal segment of the internal carotid artery (ICA), bilateral anterior cerebral arteries (ACA) and anterior communicating artery (ACoA).
A majority of anatomic variations have been observed in the AcoA section characterized as anatomic complexity and diversity. The ACoA, A1 and A2 segments of ACA and the recurrent artery of Heubner combined with their perforators and other branches are often referred as the anterior communicating artery complex (ACAC). The anatomical variations of ACAC have been proven to be closely associated with formation and prognosis of certain cerebrovascular diseases, such as intracranial aneurysms [2]. In addition, ACoA aneurysms account for 1/4 of all intracranial aneurysms and most frequently exist in the context of A1 vessel asymmetry [3]. Most studies mainly focused upon the imaging characteristics and findings of the Cycle of Willis [2]. Few investigations have been performed in terms of the anatomic outcomes of the ACAC [4-6], whereas the sample size was relatively limited.
Hence, this paper was designed comprehensively to analyze the morphology and anatomic variations of ACAC. In this study, cerebral specimens from 45 Chinese adults were dissected and observed under the microscope, aiming to provide more anatomic evidence for the ACAC variations among individuals.
Materials and methods
Sampling collection
Intact dura mater samples were collected from 45 human cadavers and fixed in 10% buffered formalin (90 cerebral hemispheres) for subsequent anatomic dissection. The cadaveric human bodies were aged 18 years. Arachinoid mater in the fossa was resected carefully to expose the Cycle of Willis. The anterior part of the Cycle of Willis was delicately separated from brain tissues. Length and diameter of the ACAC were measured under surgical microscope. The morphology, distribution and connection of different components were carefully observed and noted by photography. The morphology, structure and number of the blood vessels and their perforators were observed and counted. This study was undertaken by the approval of the ethnics committee of Shanghai JiaoTong University Affiliated Sixth People’s hospital, NO. 2011 (L)-5.
Statistical analysis
SAS6.12 statistical software was employed for statistical analysis. Raw data were statistically processed using Student’s t-test and Fisher’s exact test. P < 0.05 was considered as statistical significance.
Results
Comparison of the diameter of the A1 segments between two hemispheres
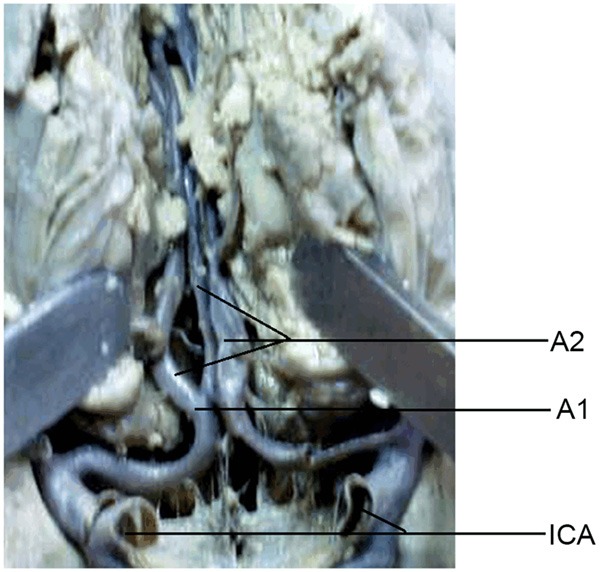
In 13.3% (6/45) brain specimens, the diameter of the A1 segments significantly differed between two hemispheres (P < 0.05). The difference in the outer diameter of blood vessels was greater than 0.5 mm. The diameter of A1 segments between both hemispheres was basically equal (≤ 0.1 mm) in 16 (35.6%). The A1 segment in one side was absent in 1 (2.2%). In the remaining 22 (48.9%), the diameter difference of the A1 segments between both sides was < 0.5 mm. As for the length of the blood vessel, the length of the A1 segment was equal in 20 (44.4%) brain specimens. A difference of 1 mm in length was found in 8 (17.8%), 2 mm in 6 (13.3%) and ≥ 3 mm in 10 (22.2%). The A2 segment of both hemispheres originated from the contralateral A1 segment in 3 (6.7%) (Figure 1).
Figure 1.
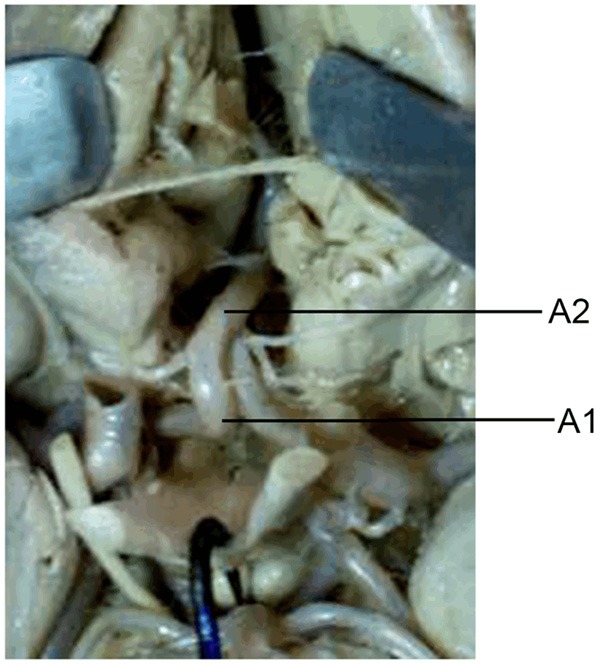
A1 segment from one hemisphere supplying the A2 segment of the contralateral hemisphere bilaterally.
Comparison of perforator number between two hemispheres
The number of perforators of the left A1 segments varied from 4 to 17 (8.82 on average), whereas 3 to 14 (mean 8.18) of the right hemisphere, excluding the recurrent artery of Heubner. The diameter of those perforators ranged between 0.05 and 1.90 mm, 0.05-0.90 mm (mean 0.23 mm) in the left side and 0.05-1.90 mm (mean 0.24) in the right hemisphere with no statistical significance (P > 0.05). In three samples, the ipsilateral frontopolar artery originated from the A1 segment, in one of which, the recurrent artery of Heubner was found to share a common stem with the ipsilateral frontopolar artery.
Variation characteristics of the ACAC
Variation characteristics of the ACAC can be mainly summarized as follows: First, the A1 segment in the right hemisphere was absent in one brain specimen, where the A2 segment of both sides merely originated from the A1 segment in the left side. A saccular aneurysm as noted in the case of bifurcation (Figure 2). Second, the trifurcation of ACAC with a diameter difference of ≥ 0.5 mm in the A1 segment was found in six brain specimens, 4 of which showed larger vessel diameter in the left side, where 2 had longer vascular diameter in the right (Figure 3).
Figure 2.
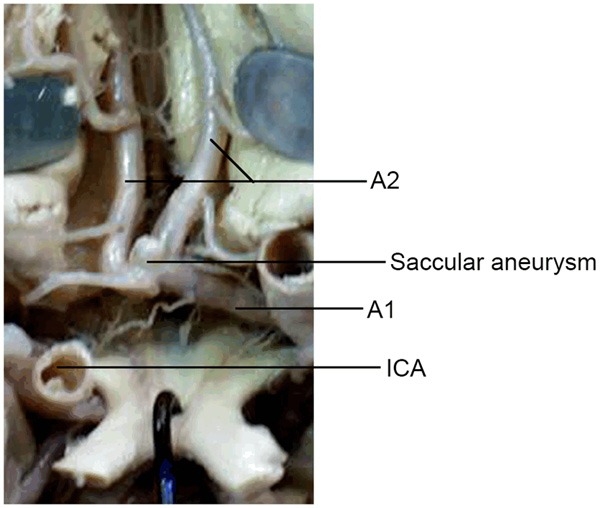
Saccular aneurysm at the bifurcation.
Figure 3.
Trifurcation of the ACA.
Comparison of length and diameter of ACoA between two hemispheres
In this experiment, the single-branch ACoA was found in 17 (37.8%) brain specimens, double-branch ACoA in 25 (55.6%), and triple-branch ACoA in three cases (4.4%). The ACoA was absent in one (2.2%) brain specimen. The length of ACoA ranged from 0 to 9.5 mm (mean 3.34 mm) and the diameter of the ACoA 0.2 to 3.9 mm (mean 1.22 mm). In six brain specimens, the diameter difference of A1 segments between two sides was greater than 0.5 mm, and the diameter of the ACoA ranged from 1.7 and 3.9 mm (2.44 ± 0.80 mm). The perforators arising from the ACoA supplied the optic chiasm, the anterior part of hypothalamus, anterior perforated substance, corpus callosum, prefrontal cortex and cingulate gyrus. The number of these perforators varied between 0 and 5 (mean 2.20) and the diameter between 0.08 and 1.80 mm (mean 0.29 mm). The variation characteristics of the ACoA can be summarized as follows: First, ACoAs were integrated by communicating branches in certain samples. Second, the “Y”-shaped ACoA was found in 8 (17.8%) and fenestrated type of ACoA in 6 (13.3%) (Figure 4). Third, the median artery of the corpus callosum was found in one brain specimen (Figure 5), which supplied cingulate gyrus, splenium of corpus callosum and paracental lobe. Fourth, a triplication of the A2 segment appeared in one brain specimen with double ACoAs (Figure 6). The diameter of the proximal branch of the ACoA was 1.8 mm and 0.4 mm for the distal branch. The diameter of this triple A2 segments was 2.2 mm in the left, 1.5 mm in the median and 2.4 mm in the right. All of these A2 segments coursed upward and backward above the corpus callosum and distributed branches to supply the corpus callosum, the orbital surface and median surface of frontal lobe, and the paracentral lobules of both sides.
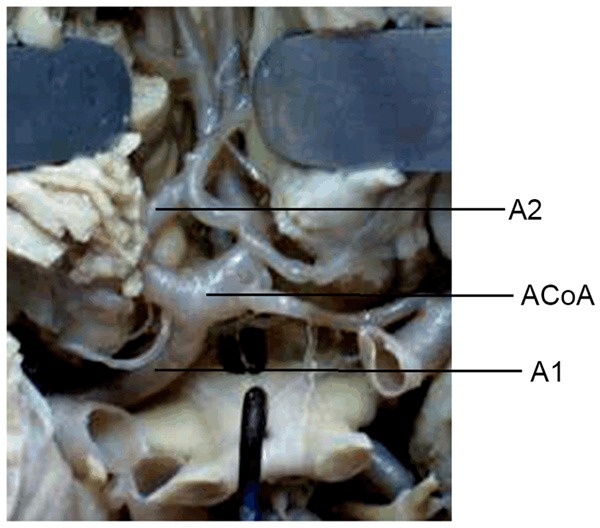
Figure 4.
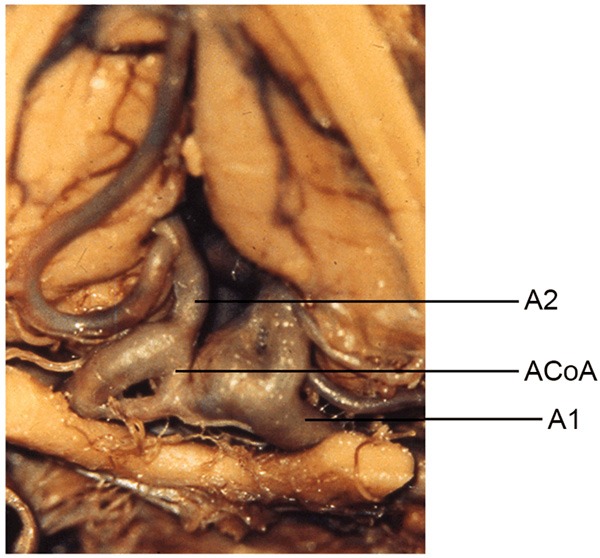
Fenestrated type of AcoA.
Figure 5.
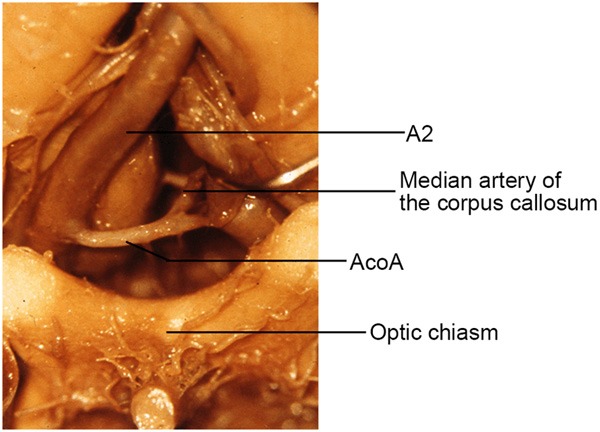
Median artery of the corpus callosum.
Figure 6.
Triplication of the postcommunical ACA.
In total, 128 recurrent arteries of Heubner were counted in 90 cerebral hemispheres, from which, single-branch recurrent arteries of Heubner were present in 55 (61.1%), two-branch, or those delivering two from one common branch, in 29 (32.2%) and three-branches in 5 (5.6%). Besides, the recurrent artery of Heubner was found to be absent in one (1.1%) hemisphere. The diameter of these recurrent arteries of Heubner ranged from 0.05 to 1.20 mm (mean 0.64 mm) and 12 to 56 mm in length (mean 30.41 mm). Of those 128 recurrent arteries of Heubner, 60 (46.88%) originated from the A1-A2 junction, 3 mm from the AcoA and merely 9 (7.03%) originated from the A1 segment. The number, diameter, length, and the original point between two hemispheres yielded no statistical difference (all P > 0.05).
Discussion
The minimally invasive anatomy of the ACAs presented with dramatic diversities. In general, the post-communicating portion (A2 segment) of the ACA originates from the pre-communicating portion (A1 segment) in the same hemisphere. However, the A2 segment in one hemisphere originated from the contralateral A1 segment in the other hemisphere in three cases in this study. Furthermore, 1 cerebral specimen was found to have only one A1 segment, in which the A2 segments in both hemispheres equally originated from the A1 segment in the left hemisphere, yielding a cystic aneurysm at the bifurcation. The formation of this cystic aneurysm probably resulted from the hemodynamic changes due to hypoplasia of the A1 segment which led to variations of elastic fibre in the ACoA vessel walls [7-9]. Similarly, aneurysms frequently occur in such cases in which the A1 segment in one hemisphere is considerably large whereas small or absent in the other part, suggesting significant diversity in vessel calibres in both hemispheres [4]. All this evidence has demonstrated that ACAs and ACoAs are the predilection sites of the aneurysms, which is consistent with the characteristics of the microanatomical variation of the anterior circulation of the Cycle of Willis.
The ACoAs can be categorized into two types according the morphology: the simple and complex types. The simple ACoAs contains only one ACoA connecting to bilateral ACAs and the complex ACoAs either includes ≥ 2 ACoAs or morphologically anomalous to fenestrated, netlike, looped or bridged shapes. In this study, simple ACoAs were present in 17 brain specimens (37.8%), suggesting that the calibres of ACoAs were positively correlated with the difference in calibres of the A1 segments in both hemispheres. In 6 specimens, the morphology of A1 segment significantly differed between two hemispheres, in which the average calibre of ACoAs was 2.44 mm, almost twice as large as that of the ACoAs with respect to all specimens. Rhoton’s report indicates that approximately 50% of the brains showed a calibre difference of ≥ 0.5 mm between the right and left A1 segments with an average calibre of the ACoA was 2.5 mm, probably because more collateral circulations flowed across the ACoA in the case of disproportionately developed A1 segments, yielding significant variations in the ACoA with a wider calibre. Therefore, distinct variations of the ACoAs were constantly present in the specimens with significant calibre difference in A1 segments between both hemispheres. Normally the median artery supplying corpus callosum originates from the AcoA [6]. The incidence of the median artery of the corpus callosum was reported to be 3.7% by Nathal and 6.6% by Marinkovic. The distal ACA, which featured larger size and more extensive supplying area, was inclined to forming triplication with the A2 segments in both hemispheres. In present study, only one brain specimen (2.2%) with triplication of the distal ACA was found, which is consistent with the findings of Gomes and Nathal [5]. Such variations tend to make the judgement of anatomy and the DSA (Digital Subtraction Angiography) of ACA more challenging. Therefore, neurosurgeons should pay more attention to differentiating this artery and preserving this area as carefully as possible intraoperatively.
The recurrent artery of Heubner is unique among arteries in that it doubles back on its parent ACA. Besides, it primarily originates from the lateral margin of the ACA, and enters the anterior perforated substance. In 1930, Critchley observed that this artery may originate from A1 segment, A2 segment, ACoA, ICA (Intracranial Artery) bifurcation site, or MCA (Middle Cerebral Artery). In 1976, Perlmutter and Rhoton found that 78% of the recurrent artery was derived from the A2 segment, 14% from the A1 segment, and the remaining 8% at the ACoA level. Through their study on 60 cerebral hemispheres, Gomes et al deduced its origin to be proximal to the ACoA in 34 cases (57% of the total), and distal to the ACoA only in 5 cases (8%). In our study, on 90 cerebral hemispheres, it was found that the recurrent artery of Heubner originated from the A2 segment in 46.1% of the total cerebral hemispheres, 46.88% from the level of the ACoA and only 7.03% from the A1 segment [5]. In addition, the recurrent artery of Heubner could also originate from the accessory MCA, the olfactory artery, or the orbitofrontal artery in very few cases. In our study, the recurrent artery of Heubner originated from the common trunk with the orbitofrontal artery in one brain specimen. The origin of the recurrent artery of Heubner remains significantly diversified, which causes inconvenience for the surgeons to estimate its origin without the aid of detailed preoperative radiological tools, thus increasing the probability of preoperative injury. Furthermore, the recurrent arteries could cohere to, circle around, or give out branches to insert the aneurysms, which might cause a misleading phenomenon that the aneurysms give out the branches. Therefore, neurosurgeons should be able to differentiate and preserve the recurrent artery of Heubner carefully during the microanatomic treatment of the aneurysms located in the ACoA, the A1 segment, the beginning of the MCA and the terminal of the ICA.
Conclusion
Taken together, extensive anatomic variations exist in the anterior portion of the Circle of Willis. The anterior part of the circle of Willis is a frequent site where aneurysm forms. Therefore, successful and efficient interventional therapy or surgical procedures should be performed based upon the thorough understanding of the microanatomical variation characteristics of ACAC.
Disclosure of conflict of interest
None.
References
- 1.Tarulli E, Sneade M, Clarke A, Molyneux AJ, Fox AJ. Effects of circle of willis anatomic variations on angiographic and clinical outcomes of coiled anterior communicating artery aneurysms. AJNR Am J Neuroradiol. 2014;35:1551–1555. doi: 10.3174/ajnr.A3991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Waaijer A, van Leeuwen MS, van der Worp HB, Verhagen HJ, Mali WP, Velthuis BK. Anatomic variations in the circle of Willis in patients with symptomatic carotid artery stenosis assessed with multidetector row CT angiography. Cerebrovasc Dis. 2007;23:267–274. doi: 10.1159/000098326. [DOI] [PubMed] [Google Scholar]
- 3.He J, Liu H, Huang B, Chi C. Investigation of morphology and anatomic variations of circle of Willis and measurement of diameter of cerebral arteries by 3D-TOF angiography. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2007;24:39–44. [PubMed] [Google Scholar]
- 4.Tao X, Yu XJ, Bhattarai B, Li TH, Jin H, Wei GW, Ming JS, Ren W, Jiong C. Microsurgical anatomy of the anterior communicating artery complex in adult Chinese heads. Surg Neurol. 2006;65:155–161. doi: 10.1016/j.surneu.2005.05.027. discussion 161. [DOI] [PubMed] [Google Scholar]
- 5.Gomes FB, Dujovny M, Umansky F, Berman SK, Diaz FG, Ausman JI, Mirchandani HG, Ray WJ. Microanatomy of the anterior cerebral artery. Surg Neurol. 1986;26:129–141. doi: 10.1016/0090-3019(86)90365-4. [DOI] [PubMed] [Google Scholar]
- 6.Kahilogullari G, Comert A, Arslan M, Esmer AF, Tuccar E, Elhan A, Tubbs RS, Ugur HC. Callosal branches of the anterior cerebral artery: an anatomical report. Clin Anat. 2008;21:383–388. doi: 10.1002/ca.20647. [DOI] [PubMed] [Google Scholar]
- 7.Meng H, Wang Z, Hoi Y, Gao L, Metaxa E, Swartz DD, Kolega J. Complex hemodynamics at the apex of an arterial bifurcation induces vascular remodeling resembling cerebral aneurysm initiation. Stroke. 2007;38:1924–1931. doi: 10.1161/STROKEAHA.106.481234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Valencia AA, Guzman AM, Finol EA, Amon CH. Blood flow dynamics in saccular aneurysm models of the basilar artery. J Biomech Eng. 2006;128:516–526. doi: 10.1115/1.2205377. [DOI] [PubMed] [Google Scholar]
- 9.Perlmutter D, Rhoton AL Jr. Microsurgical anatomy of the anterior cerebral-anterior communicating-recurrent artery complex. J Neurosurg. 1976;45:259–272. doi: 10.3171/jns.1976.45.3.0259. [DOI] [PubMed] [Google Scholar]