

Abstract
The aim of this study was to investigate the clinical application effects of a novel computer-aided detection (CAD) system based on three-dimensional computed tomography (CT) images on pulmonary nodule. 98 cases with pulmonary nodule (PN) in our hospital from Jun, 2009 to Jun, 2013 were analysed in this study. All cases underwent PN detection both by the simple spiral CT scan and by the computer-aided system based on 3D CT images, respectively. Postoperative pathological results were considered as the “gold standard”, for both two checking methods, the diagnostic accuracies for determining benign and malignant PN were calculated. Under simple spiral CT scan method, 63 cases is malignant, including 50 true positive cases and 13 false positive cases from the “gold standard”; 35 cases is benign, 16 true negative case and 19 false negative cases, the Sensitivity 1 (Se1)=0.725, Specificity1 (Sp1)=0.448, Agreement rate1 (Kappa 1)=0.673, J1 (Youden’s index 1)=0.173, LR(+)1=1.616, LR(-)1=0.499. Kappa 1=0.673 between the 0.4 and 0.75, has a moderate consistency. Underwent computer-aided detection (CAD) based on 3D CT method, 67cases is malignant, including 62 true positive cases and 7 false positive cases; 31 cases is benign, 24 true negative case and 7 false negative cases, Sensitivity 2 (Se2)=0.899, Specificity2 (Sp2)=0.828, Agreement rate (Kappa 2)=0.877, J2 (Youden’s index 2)=0.727, LR(+)2=5.212, LR(-)2=0.123. Kappa 2=0.877 >0.75, has a good consistency. Computer-aided PN detecting system based on 3D CT images has better clinical application value, and can help doctor carry out early diagnosis of lung disease (such as cancer, etc.) through CT images.
Keywords: Pulmonary nodule, diagnosis, computer-assisted, three-dimensional image
Introduction
Recent years, the morbidity and mortality of lung cancer is gradually increasing, and lung cancer has become the leading cause of cancer deaths worldwide [1]. Due to the population aging and increasing smoking, lung cancer has a high frequency in many developing countries, especially in China [2]. Compared to the other kinds of cancers, the biological characteristics of the lung cancer is very complex, its onset time is short, malignancy degree is high, metastasis is fast, difficult to be early diagnosed, so most of patients had developed into advanced stage and lost the chance of surgery because of lack of early screening [3]. Several evidences showed early computed tomography (CT) screening significantly reduces lung cancer mortality [4,5]. Even the CT image features have a good predictability of radiological prognosis for lung cancer [6]. Nowadays, CT technology for diagnosis of lung cancer has developed into a new phase known as computer aided diagnosis (CAD) [7]. Numerous studies have demonstrated [8-10]. CAD systems can be used as a radiologist’s “second eyes”, automatic detect suspicious lung nodules in CT images, so as to reduce the oversight and workload of radiologists in alone reading and diagnostic process, improve the accuracy and efficiency of the early diagnosis of lung diseases such as lung cancer.
But the existing CT lung lesion detection method relies on human intervention, is not high degree of automation, some automatic detection methods need to be further improved on its detection performance. In the aspect of feature quantification, due to the inaccurate lung lesion segmentation and the special characteristics of lesion features, it has limited accuracy on quantitative results. So our hospital and Huazhong University of Science and Technology jointly developed a set of prototype CAD system based on 3D CT images for detecting the pulmonary nodule (PN) [11]. Based on the previous studies [11-13], by computer image processing techniques such as enhancement, segmentation and morphological, as well as artificial intelligence techniques such as feature selection and machine learning, we designed a computer system for effective automatic detection and quantitative analysis, to assist radiologists for early diagnosis of lung cancer and other lung diseases in CT images. Attempts to evaluate the accuracy of our system for distinguishing the benign from malignant lesions, we compared the correspondence between the results by the simple spiral CT scan or by the CAD system based on 3D CT with postoperative pathological results from the same patients with PN.
Methods
General data of patient recruitment
98 cases with PN collected from the Third Affiliated Hospital of Guangxi Medical University from Jun, 2009 to Jun, 2013 were included in this study, including 30 males, 68 females, age from 40 to 72, average 50.8 years old, with 82 cases of solitary pulmonary nodule, 16 cases of multiple nodules; 38 cases in left lungs, 50 cases in right lungs, 10 cases in both lungs; pulmonary nodule diameters are 5~30 mm and the number is less 6. 24 cases have varying degrees of irritation cough, 18 cases have chest pain, 8 cases have hemoptysis, 30 cases are accidentally discovered in health check, 10 cases are found by chest X-ray or CT due to other diseases. This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Guangxi Medical University. Written informed consent was obtained from all participants.
Image collection
Conventional X-ray examinations are applied for all cases, after the lesions were found, baseline and follow up CT of the thorax for each patient were acquired within 15 min of each other, and using the same CT scanner and imaging protocol, this enables testing extracted image features for stability. Unenhanced and dynamic contrast-enhanced thoracic CT images were acquired using the GE Brightspeed Elite spiral CT scanners with 120 kvp tube voltage and image slices thickness of 1.25 mm were reconstructed using the same lung convolution kernel without overlap [6].
Image analysis
Collected image datum are input into a post-processing workstation for reading and are analysed by two deputy chief radiologists until a consensus diagnosis is reached after a discussion. The observation of the reading focus on the lung nodule distribution, shape, internal structure, bronchial symptoms, vacuole sign, etc., the radiologists judge the marker one by one and make a qualitative diagnosis.
And then CAD system based on the three-dimensional CT image is used for further checking the collected image, preliminary make diagnosis on benign and malignant lesions. The details of analysis method have been described in Min et al. [11], Wang et al. [12] and Yu et al. [13]. The system starts with automatically detection of candidate nodules/masses from CT images, and extracts 21 features, including location, shape, size and density characteristics, so as to preliminarily judge the benign and malignant lesions (Figures 1, 2). According to the results of the detection and quantification of lung nodules and trachea, the system intelligently generates a diagnostic report. Based on the report, two radiologists through a discuss judge the signs and make a common qualitative diagnosis.
Figure 1.
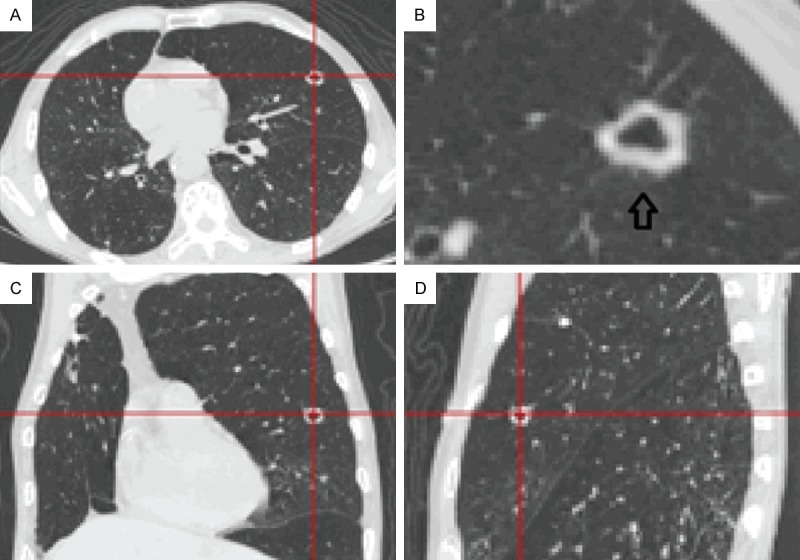
Lung nodule/mass detection and feature quantification subsystem. First automatic detection of lung nodules using multi scale selective enhancement filter based on Hessian matrix eigenvalues and automatic lung nodule detection algorithm based on Fisher linear classifie.
Figure 2.
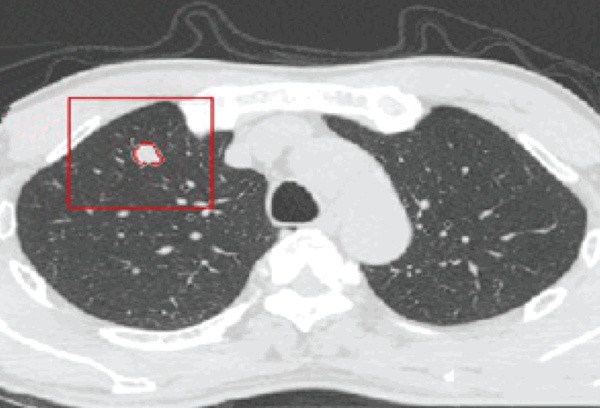
Lung nodule/mass segmentation. Automatic segmentation of lung nodules using the three-dimensional image segmentation algorithm based on the level set and dynamic programming with multi-directional integration approach, while allowing physicians to modify the automatic segmentation results. Using the results of segmentation, the system can extract and quantify the lobulation and spiculation features for candidate nodules, and quantify other morphological and density features, and then the system intelligently generates a diagnostic report.
Surgery and pathological results
All the patients took the surgical treatment. The lung tissue containing tumor is wedge resectioned or simply the tumor is resection with small incisions and is sent for intraoperative frozen biopsy. For the rapid pathologically diagnosed malignant lesions, perform the standard lobectomy and lymph node dissection, or pulmonary wedge resection, depending on the lung function. For the benign lesions, perform the lung residual surface suture and terminate the surgery. And to the bilateral lesions, tumor biopsy is only performed on one side. Post-operative pathologic results, made by two chief pathologists with a agreement, are used as the gold standard for the last diagnostic results.
Statistical analysis
The postoperative pathological examination results are taken as the “gold standard” for comparing the accuracies of determining benign and malignant pulmonary nodules between the two imaging examination, the values of Youden’s index (J) and likelihood ratio (LR), including positive likelihood ratio (LR+) and negative likelihood ratio (LR-), are used to evaluate the accuracies, respectively, higher J and LR+ value, or lower LR- value means better accuracy compared with the “gold standard”. The agreement rate is to illustrate the consistency test for each diagnosis (Kappa test). Kappa ≥0.75 is considered as a good consistency; 0.4 ≤ Kappa <0.75 as a moderate consistency; Kappa <0.4 as a bad consistency.
Results
98 cases with PN were diagnosed by simple spiral CT scan results, CAD based on 3D CT results, post operative pathology in order for distinguishing the malignant and benign.
Pathological findings
The pathologic result showed 69 malignant cases (including 42 cases of squamous cell carcinoma, 20 cases of adenocarcinoma, 7 cases of alveolar cell carcinoma) and 29 benign cases (15 cases of tuberculosis ball, 9 cases of inflammatory mass and 5 cases of hamartoma) in this group.
The accuracy and consistency of simple spiral CT scan
Under this method, 63 cases is malignant, including 50 true positive cases and 13 false positive cases from the “gold standard”; 35 cases is benign, 16 true negative case and 19 false negative cases (Table 1), the Sensitivity 1 (Se1)=0.725, Specificity1 (Sp1)=0.448, Agreement rate1 (Kappa 1)=0.673, J1 (Youden’s index 1)=0.173, LR(+)1=1.616, LR(-)1=0.499. Kappa 1=0.673 between the 0.4 and 0.75, means a moderate consistency.
Table 1.
Diagnosis results of post operative pathology and simple spiral CT scan
| Pathologic results (number) | Simple spiral CT scan results (number) | Total | |
|---|---|---|---|
|
| |||
| Malignant | benign | ||
| Malignant | 50 | 19 | 69 |
| Benign | 13 | 16 | 29 |
| Total | 63 | 35 | 98 |
Note: Sensitivity (Se)=0.725, Specificity (Sp)=0.448, Agreement rate (Kappa)=0.673, J (Youden’s index)=0.173, LR(+)=1.616, LR(-)=0.499.
The accuracy and consistency of CAD based on 3D CT
Underwent this method, 67cases is malignant, including 62 true positive cases and 7 false positive cases; 31 cases is benign, 24 true negative case and 7 false negative cases (Table 2), Sensitivity 2 (Se2)=0.899, Specificity 2 (Sp2)=0.828, Agreement rate (Kappa 2)=0.877, J2 (Youden’s index 2)=0.727, LR(+)2=5.212, LR(-)2=0.123. Kappa 2=0.877 >0.75, means a good consistency.
Table 2.
Diagnosis results of post operative pathology and CAD based on 3D CT
| Pathologic results (number) | CAD based on 3D CT results (number) | Total | |
|---|---|---|---|
|
| |||
| Malignant | Benign | ||
| Malignant | 62 | 7 | 69 |
| Benign | 5 | 24 | 29 |
| Total | 67 | 31 | 98 |
Note: Sensitivity (Se)=0.899, Specificity (Sp)=0.828, Agreement rate (Kappa)=0.877, J (Youden’s index)=0.727, LR(+)=5.212, LR(-)=0.123.
Compare the accuracy and consistency of two imaging examinations
Given from the above data, Agreement rate (Kappa 1)=0.673 <Agreement rate (Kappa 2)=0.877, shows that the consistency of CAD based on 3D CT is better than the simple spiral CT scan; J1 (Youden’s index 1)=0.173 <J2 (Youden’s index 2)=0.727, LR(+)1=1.616 <LR(+)2=5.212, LR(-)1=0.499 >LR(-)2=0.123, this three pair data have a strong evidence that the accuracy of CAD based on 3D CT is more better than the simple spiral CT scan.
Discussion
A pulmonary nodule (PN) usually has a higher radio-density than other normal lung parenchyma, appearing white on the images. Lung nodules may imply a malignant lesion. Early diagnosis of lung cancer is vital for success of therapy. CT is considered to be the most accurate imaging modality for nodule detection. With CT screening, most of lung cancer could be detected (60-100%) in stage I [14]. However, hundreds of data per examination makes a difficult analysis, leading to oversight some nodules by the radiologist. Now CT technology for diagnosis of PN has gone into a new age known as computer-aided detection (CAD). Different type of automated CAD systems become helpful to radiologists for detection and diagnose of PN from CT slices [8,9,15-18]. Armato et al. [19] found that with an automated lung nodule detection method, a large percent (84%) of missed cancers in a database of low-dose CT scans were detected correctly. Some researchers are still looking for new method to improve the accuracy of CDA system. Suzuki et al. [20] use of a multi-MTANN reduced the false-positive rate of the CAD for lung nodule detection on chest radiographs.
The PN identification and segmentation is a key step in this system. Due to the varieties of PN, many segmentation methods have been explored [13]. In the present, we worked together with Huazhong University of Science and Technology designing a computer system for effective automatic detection and quantitative analysis, to assist radiologists for early diagnosis of lung cancer and other lung diseases in CT images. The system uses multi scale selective enhancement filter based on Hessian matrix eigenvalues and automatic lung nodule detection algorithm based on Fisher linear classifier for segmenting lung nodules on three dimensional (3D) computed tomographic images, to improve the performance of computer-aided diagnosis (CAD) systems. In this study, we collected the clinical patients data to evaluate its applied value in practice, the data showed that our CAD prototype system based on 3D CT has a better accuracy than simple spiral CT scan on distinguishing the malignant and benign PN, J2 (Youden’s index 2)=0.727 >J1 (Youden’s index 1)=0.173, LR(+)2=5.212 >LR(+)1=1.616, LR(-)2=0.123 <LR(-)1=0.499, and Kappa 2 value is 0.877 >0.75, has a good consistency compared with Kappa 1=0.673 between the 0.4 and 0.75, a moderate consistency with the pathologic results. Therefore, the CAD prototype system based on three-dimensional CT images has better clinical value than simple spiral CT scan and can be used to assist physicians in early diagnosis of lung cancer and other lung diseases from CT images.
Conclusion
Computer-aided PN detecting system based on 3D CT images has better clinical application value, and can help doctor carry out early diagnosis of lung disease (such as cancer, etc.) through CT images.
Acknowledgements
Foundation item: Guangxi Scientific and Technological Development Projects (No. 081600418).
Disclosure of conflict of interest
None.
References
- 1.Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. doi: 10.3322/caac.20138. [DOI] [PubMed] [Google Scholar]
- 2.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 3.Reddy C, Chilla D, Boltax J. Lung cancer screening: a review of available data and current guidelines. Hosp Pract (1995) 2011;39:107–12. doi: 10.3810/hp.2011.10.929. [DOI] [PubMed] [Google Scholar]
- 4.National Lung Screening Trial Research Team. Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, Fagerstrom RM, Gareen IF, Gatsonis C, Marcus PM, Sicks JD. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365:395–409. doi: 10.1056/NEJMoa1102873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Prosch H, Schaefer-Prokop C. Screening for lung cancer. Curr Opin Oncol. 2014;26:131–137. doi: 10.1097/CCO.0000000000000055. [DOI] [PubMed] [Google Scholar]
- 6.Balagurunathan Y, Kumar V, Gu Y, Kim J, Wang H, Liu Y, Goldgof DB, Hall LO, Korn R, Zhao B, Schwartz LH, Basu S, Eschrich S, Gatenby RA, Gillies RJ. Test-retest reproducibility analysis of lung CT image features. J Digit Imaging. 2014;27:805–823. doi: 10.1007/s10278-014-9716-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Iqbal S, Iqbal K, Arif F, Shaukat A, Khanum A. Potential lung nodules identification for characterization by variable multistep threshold and shape indices from CT images. Comput Math Methods Med. 2014;2014:241647. doi: 10.1155/2014/241647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gu Y, Kumar V, Hall LO, Goldgof DB, Li CY, Korn R, Bendtsen C, Velazquez ER, Dekker A, Aerts H, Lambin P, Li X, Tian J, Gatenby RA, Gillies RJ. Automated delineation of lung tumors from CT images using a single click ensemble segmentation approach. Pattern Recognit. 2013;46:692–702. doi: 10.1016/j.patcog.2012.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cascio D, Magro R, Fauci F, Iacomi M, Raso G. Automatic detection of lung nodules in CT datasets based on stable 3D mass-spring models. Comput Biol Med. 2012;42:1098–1109. doi: 10.1016/j.compbiomed.2012.09.002. [DOI] [PubMed] [Google Scholar]
- 10.Messay T, Hardie RC, Rogers SK. A new computationally efficient CAD system for pulmonary nodule detection in CT imagery. Med Image Anal. 2010;14:390–406. doi: 10.1016/j.media.2010.02.004. [DOI] [PubMed] [Google Scholar]
- 11.Min ZF, Jin RC, Song EM, Liu H, Wang XT, Hung CC. 3-D segmentation of lung nodules in CT images based on improved level set method. Information. 2011;14:1411–1418. [Google Scholar]
- 12.Wang Q, Song E, Jin R, Han P, Wang X, Zhou Y, Zeng J. Segmentation of lung nodules in computed tomography images using dynamic programming and multidirection fusion techniques. Acad Radiol. 2009;16:678–688. doi: 10.1016/j.acra.2008.12.019. [DOI] [PubMed] [Google Scholar]
- 13.Yu ML, Song EM, Jin RC, Liu H, Ma GZ, Hung CC. Automatic segmentation of lung nodules based on intensity-guided active contours. International Workshop on Graphics and Vision 2013, IWGV 2013; May 8-11. Tokyo, Japan. [Google Scholar]
- 14.Pastorino U. Lung cancer screening. Br J Cancer. 2010;102:1681–1686. doi: 10.1038/sj.bjc.6605660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.El-Baz A, Elnakib A, Abou El-Ghar M, Gimel’ farb G, Falk R, Farag A. Automatic detection of 2D and 3D lung nodules in chest spiral CT scans. Int J Biomed Imaging. 2013;2013:517632. doi: 10.1155/2013/517632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yanagawa M, Tanaka Y, Kusumoto M, Watanabe S, Tsuchiya R, Honda O, Sumikawa H, Inoue A, Inoue M, Okumura M, Tomiyama N, Johkoh T. Automated assessment of malignant degree of small peripheral adenocarcinomas using volumetric CT data: correlation with pathologic prognostic factors. Lung Cancer. 2010;70:286–294. doi: 10.1016/j.lungcan.2010.03.009. [DOI] [PubMed] [Google Scholar]
- 17.Lee Y, Hara T, Fujita H, Itoh S, Ishigaki T. Automated detection of pulmonary nodules in helical CT images based on an improved template-matching technique. IEEE Trans Med Imaging. 2001;20:595–604. doi: 10.1109/42.932744. [DOI] [PubMed] [Google Scholar]
- 18.Tan M, Deklerck R, Jansen B, Bister M, Cornelis J. A novel computer-aided lung nodule detection system for CT images. Med Phys. 2011;38:5630–5645. doi: 10.1118/1.3633941. [DOI] [PubMed] [Google Scholar]
- 19.Armato SG 3rd, Li F, Giger ML, MacMahon H, Sone S, Doi K. Lung cancer: performance of automated lung nodule detection applied to cancers missed in a CT screening program. Radiology. 2002;225:685–92. doi: 10.1148/radiol.2253011376. [DOI] [PubMed] [Google Scholar]
- 20.Suzuki K, Shiraishi J, Abe H, MacMahon H, Doi K. False-positive reduction in computer-aided diagnostic scheme for detecting nodules in chest radiographs by means of massive training artificial neural network. Acad Radiol. 2005;12:191–201. doi: 10.1016/j.acra.2004.11.017. [DOI] [PubMed] [Google Scholar]