

Abstract
Background: Researches of the relationships between dietary whole grains intake and risk of stroke have produced inconsistent results. We therefore conducted a meta-analysis to summarize the evidence from observed studies regarding the association between whole grain intake and stroke risk. Methods: Pertinent studies were identified by searching Web of Knowledge and PubMed up to May 2015. Random-effect model was used to combine the relative risk (RR) with the corresponding 95% confidence intervals (CI). Publication bias was estimated using Egger’s regression asymmetry test. Results: Six prospective studies involving 1635 stroke cases and 247487 participants were included in this meta-analysis. Pooled results suggested that highest category of whole grain intake versus lowest category was significantly associated with reduced the risk of stroke [summary RR = 0.86, 95% CI = 0.73-0.99, I2 = 0.0%]. Inverse associations were also found in the America population [summary RR = 0.81, 95% CI = 0.67-0.98, I2 = 0.0%] and subgroup analysis of females [summary RR = 0.78, 95% CI = 0.63-0.97, I2 = 0.0%]. No publication bias was found. Conclusion: Our analysis indicated that higher whole grain intake has a protective effect on stroke.
Keywords: Whole grain, stroke, meta-analysis
Introduction
Stroke is a leading cause of mortality and morbidity in the world [1]. The rates of age-adjusted stroke mortality and disability-adjusted life years lost were higher in low-income countries than in middle-income or high-income countries [2]. Improving diet and lifestyle is critical for stroke risk reduction in the general population [3,4]. In particular, a diet rich in whole grain food is highly recommended, because they are rich sources of fiber, K and antioxidant compounds, which through different mechanisms may have protective effects against stroke [5]. Up to date, a number of epidemiologic studies have been published to explore the relationship between whole grain intake and stroke risk. Only one study reported that higher whole grain intake could reduce the risk of stroke [6], while no significant associations were reported in 3 studies [7-9]. Furthermore, two studies found an increased but not significant association between whole grain intake and the risk of stroke [10,11]. Considering the results are not consistent, we conducted a comprehensive meta-analysis to evaluate the evidence from observational studies on whole intake with the risk of stroke.
Methods
Literature search strategies
Studies were identified by a literature search of PubMed and Web of Knowledge through May 2015. The following search strategy was used: ‘whole grain’ or ‘diet’ or ‘lifestyle’ in combined with ‘stroke’. Furthermore, we reviewed citations from the retrieved articles and relevant reviews to identify additional studies. Two researchers searched the related articles and reviewed of all retrieved studies independently. Disagreements between the two researchers were resolved by consensus with a third reviewer.
Eligibility criteria
Our meta-analysis included prospective studies or case-control studies that reported the association between whole grain intake and the risk of stroke. All studies should be written in English. The outcome measure was stroke. The exposure of interest was the intake of whole grain. All included studies provided the relative risk (RR) or hazard ratio (HR) or odds ratio (OR) and the corresponding 95% confidence intervals (CI), or provided enough data to calculate them. If several papers from the same study had been published, we only included the most complete or most recent paper.
Data extraction
The following information was extracted from each study: the first author’s last name, year of publication, study design, sex, geographic locations, number of cases and participants. The RR estimates and 95% CI for whole grain intake and stroke risk were also extracted, and confounding factors adjusted for in the analysis. For studies that reported results from various covariate analyses, we abstracted the estimates based on the model that included the most potential confounders. Otherwise, we abstracted the crude RR estimates. If there was disagreement between the two investigators about eligibility of the data, it was resolved by consensus with a third reviewer.
Statistical analysis
Pooled measure was calculated as the inverse variance-weighted mean of the logarithm of RR with 95% CI, to assess the association between whole grain intake and the risk of stroke. Random-effects model was used to combine study-specific RR (95% CI), which considers both within-study and between-study variation [12]. The I2 was used to assess the between-study heterogeneity, and I2 values of 0, 25, 50 and 75% represent no, low, moderate and high heterogeneity [13], respectively. Subgroup analysis was performed to assess the association between whole grain intake and stroke risk in some subgroup analyses. Publication bias was estimated using Egger’s regression asymmetry test [14]. Sensitivity analysis [15] was conducted to describe how robust the pooled estimator is to removal of individual studies. All the statistical analyses were performed with STATA version 10.0. Two-tailed P < 0.05 was accepted as statistically significant.
Results
Search results and study characteristics
We searched 123 articles from Pub Med and 167 articles from the Web of Knowledge, and 40 articles were reviewed in full after reviewing the title or abstract. At the end, 6 articles [6-11] involving 1635 stroke cases were used in this meta-analysis. All the included studies were prospective design. The detailed steps of our literature search are shown in Figure 1. The characteristics of these included studies are presented in Table 1. There are 5 studies come from United States and 1 from Finland.
Figure 1.
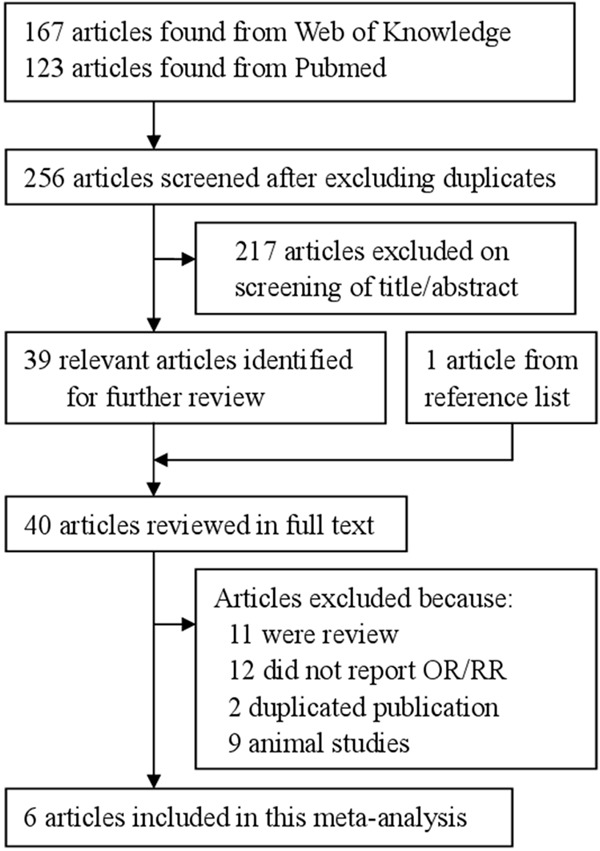
The detailed steps of our literature search.
Table 1.
Characteristics of included studies on whole grain and stroke risk
| Study, year | Ref. | Study name | Country | Participants (cases) | Follow-up (years) | Age (years) | RR (95% CI) for highest versus lowest category | Adjustment for covariates |
|---|---|---|---|---|---|---|---|---|
| Jacobs et al. 1999 | [7] | The Iowa Women’s Health Study | United States | 38740 (1779) | 9 | 55-69 | 0.87 (0.52-1.48) | Adjusted for age, total energy intake, educational attainment, marital status, high blood pressure, diabetes, heart disease, cancer, BMI, waist-to-hip ratio, physical activity, smoking, alcohol intake, vitamin supplements, estrogen replacement therapy use, total fat, saturated fat, intake of fruits and vegetables, intake of red meat, and intake of fish and seafood. |
| Jacobs et al. 2007 | [8] | The Iowa Women’s Health Study | United States | 27312 (2934) | 17 | 55-69 | 0.85 (0.60-1.21) | Adjusted for age, energy intake, BMI, waist-hip ratio, smoking, education, physical activity, estrogen use, multivitamin supplement use, and intakes of alcohol, refined grain, coffee, red meat, fish and seafood, and total fruit and vegetables. |
| Liu et al. 2000 | [6] | The Nurses’ Health Study | United States | 75521 (761) | 12 | 38-63 | 0.69 (0.50-0.98) | Adjusted for age, BMI, cigarette smoking, alcohol intake, parental or family history of myocardial infarction before the age of 60 y, self-reported history of hypertension or hypercholestoremia, menopausal status, protein intake, aspirin use, use of multiple vitamin or vitamin E supplements, vigorous activity. |
| Liu et al. 2003 | [10] | The Physicians’ Health Study | United States | 86190 (1869) | 5.5 | 40-84 | 1.04 (0.65-1.65) | Adjusted for age, cigarette smoking, alcohol intake, physical activity, BMI, history of type 2 diabetes, high cholesterol, and hypertension, and use of multivitamins. |
| Mizrahi et al. 2009 | [11] | The Finnish Mobile Clinic Health Examination Survey | Finland | 3932 (344) | 24 | 40-74 | 1.06 (0.75-1.50) | Adjusted for age, sex, BMI, smoking, physical activity, serum cholesterol level, blood pressure and energy. |
| Steffen et al. 2003 | [9] | The Atherosclerosis Risk in Communities (ARIC) Study | United States | 15792 (535) | 11 | 45-64 | 0.75 (0.46-1.22) | Adjusted for age at baseline, BMI, race, sex, time-dependent energy intake, education, smoking status, pack-years of smoking, physical activity, alcohol intake, and hormone replacement in women. |
Abbreviations: Ref. = reference; BMI = body mass index; CI = confidence interval; RR = relative risk.
Highest whole grain intake vs. lowest intake analysis
For whole grain intake and stroke risk, data from 6 prospective studies were used including 1635 stroke cases. Only one of the included studies reported an inverse association of whole intake with the risk of stroke, while no significant association was reported in 5 studies. Our pooled results suggested that highest category of whole grain intake versus lowest category was significantly associated with reduced the risk of stroke [summary RR = 0.86, 95% CI = 0.73-0.99, I2 = 0.0%] (Figure 2).
Figure 2.
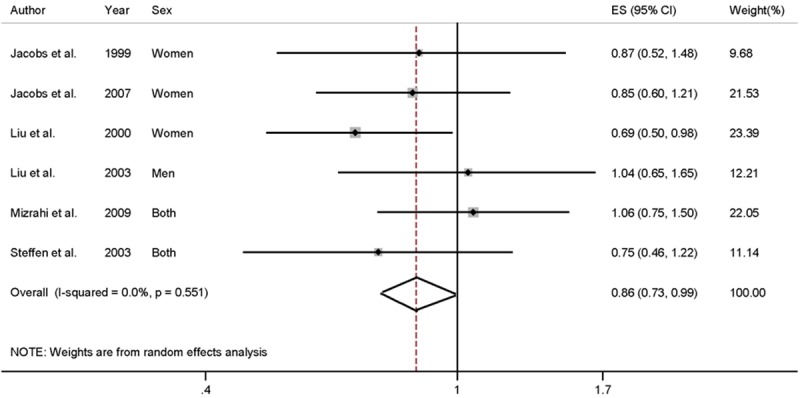
The forest plot between highest versus lowest categories of whole grain intake and stroke risk.
For the stratified analysis by geographic locations, we only combined the results for American, while 1 study was come from Finland. The association was significant in the America population [summary RR = 0.81, 95% CI = 0.67-0.98, I2 = 0.0%]. In subgroup analyses for follow-up duration (< 10 years or ≥ 10 years), inverse association of whole grain intake with the risk of stroke was only found in the duration of ≥ 10 years [summary RR = 0.84, 95% CI = 0.69-0.99, I2 = 7.7%], but not in the duration of < 10 years [summary RR = 0.96, 95% CI = 0.68-1.36, I2 = 0.0%]. When we conducted the subgroup analysis by sex, significant association was only significant in the females [summary RR = 0.78, 95% CI = 0.63-0.97, I2 = 0.0%], but not in the males.
Sensitivity analysis and publication bias
Sensitivity analysis showed that no individual study had excessive influence on the association of whole grain intake and stroke risk (Figure 3). Egger’s test (P = 0.836) showed no evidence of significant publication bias between whole grain intake and the risk of stroke was found.
Figure 3.
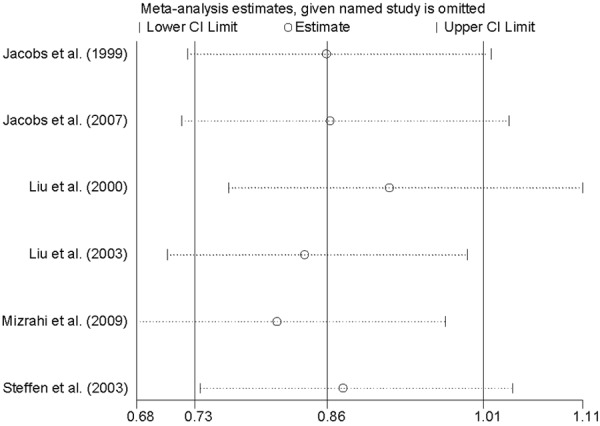
Analysis of influence of individual study on the association between whole grain intake and stroke risk. Open circle, the pooled RR, given named study is omitted. Horizontal lines represent the 95% CIs.
Discussion
Findings from this meta-analysis indicated that highest category of whole grain intake versus lowest category was significantly associated with the reduced risk of stroke. Inverse association was also found in American, but not in the other populations. The associations were also significant in the group of follow-up duration ≥ 10 years and females.
Previous study had reported that whole grain intake has a protective effect against coronary heart disease [16]. A meta-analysis suggested that an increment of three servings daily of whole grains could reduce the risk of colorectal cancer [17]. Furthermore, whole grain intake had an inverse association with type 2 diabetes risk [18]. Several potential mechanisms for the observed association have been proposed. Whole-grain foods contain fiber, vitamins, minerals, and other phytochemicals that are removed during the refining process [19-22]. Many of these compounds can support the antioxidant defense and thereby reduce the damaging effects of chronic inflammation via several mechanisms [23,24]. It has been suggested that these molecules also can mount an antioxidant defense in animal cells (after intake by the animal) by inducing gene expression of similar genes for antioxidant and detoxification enzymes [25]. Thus, we think it is plausible that whole grain intake may reduce the risk of stroke.
A major strength of this study was the large number of cases and participants included from prospective studies, allowing a much greater possibility of reaching reasonable conclusions and conducting subgroup analysis. And prospective studies do not suffer from recall bias and are anticipated to be less likely to have selection bias relative to case-control studies. Second, no evidence of between-study heterogeneity and no publication bias were found, indicating that our results are stable. However, some limitations in this meta-analysis should be concerned. First, although we extracted the RR that reflected the greatest degree of control for potential confounders, the extent to which they were adjusted and the possibility that the observed association was due to unmeasured or residual confounding should be considered. Second, for the subgroups of geographic locations, five of the six included studies come from American. And the association was significant in the America pipulation for whole grain intake and the risk of stroke. There is only one study come from Finland. So, we did not combine the results for other contries. Due to this limitation, the results are applicable to the America population, but cannot be extended to populations elsewhere. More studies originating in other countries are required to investigate the association between whole grain intake and stroke risk. Finally, for the subgroup analysis of follow-up duration, we found a significant association in the follow-up duration ≥ 10 years, but not in the < 10 years. Therefore, further studies should be ≥ 10 years to assess the association between whole grain intake and the risk of stroke.
In summary, results from this meta-analysis suggested that higher intake of whole might have a protective effect on stroke.
Disclosure of conflict of interest
None.
References
- 1.Goldstein LB, Bushnell CD, Adams RJ, Appel LJ, Braun LT, Chaturvedi S, Creager MA, Culebras A, Eckel RH, Hart RG, Hinchey JA, Howard VJ, Jauch EC, Levine SR, Meschia JF, Moore WS, Nixon JV, Pearson TA American Heart Association Stroke Council; Council on Cardiovascular Nursing; Council on Epidemiology and Prevention; Council for High Blood Pressure Research; Council on Peripheral Vascular Disease, and Interdisciplinary Council on Quality of Care and Outcomes Research. Guidelines for the primary prevention of stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:517–84. doi: 10.1161/STR.0b013e3181fcb238. [DOI] [PubMed] [Google Scholar]
- 2.Sharma S, Cruickshank JK, Green DM, Vik S, Tome A, Kolonel LN. Impact of diet on mortality from stroke: results from the U. S. multiethnic cohort study. J Am Coll Nutr. 2013;32:151–9. doi: 10.1080/07315724.2013.791798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Larsson SC, Virtamo J, Wolk A. Total and specific fruit and vegetable consumption and risk of stroke: a prospective study. Atherosclerosis. 2013;2:147–52. doi: 10.1016/j.atherosclerosis.2012.12.022. [DOI] [PubMed] [Google Scholar]
- 4.Chan R, Chan D, Woo J. The association of a priori and a posterior dietary patterns with the risk of incident stroke in Chinese older people in Hong Kong. J Nutr Health Aging. 2013;17:866–74. doi: 10.1007/s12603-013-0334-y. [DOI] [PubMed] [Google Scholar]
- 5.Khaw KT, Barrett-Connor E. Dietary potassium and stroke-associated mortality. A 12-year prospective population study. N Engl J Med. 1987;316:235–40. doi: 10.1056/NEJM198701293160502. [DOI] [PubMed] [Google Scholar]
- 6.Liu S, Manson JE, Stampfer MJ, Rexrode KM, Hu FB, Rimm EB, Willett WC. Whole grain consumption and risk of ischemic stroke in women: A prospective study. JAMA. 2000;284:1534–40. doi: 10.1001/jama.284.12.1534. [DOI] [PubMed] [Google Scholar]
- 7.Jacobs DR Jr, Meyer KA, Kushi LH, Folsom AR. Is whole grain intake associated with reduced total and cause-specific death rates in older women? The Iowa Women’s Health Study. Am J Public Health. 1999;89:322–9. doi: 10.2105/ajph.89.3.322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jacobs DR Jr, Andersen LF, Blomhoff R. Whole-grain consumption is associated with a reduced risk of noncardiovascular, noncancer death attributed to inflammatory diseases in the Iowa Women’s Health Study. Am J Clin Nutr. 2007;85:1606–14. doi: 10.1093/ajcn/85.6.1606. [DOI] [PubMed] [Google Scholar]
- 9.Steffen LM, Jacobs DR Jr, Stevens J, Shahar E, Carithers T, Folsom AR. Associations of whole-grain, refined-grain, and fruit and vegetable consumption with risks of all-cause mortality and incident coronary artery disease and ischemic stroke: the Atherosclerosis Risk in Communities (ARIC) Study. Am J Clin Nutr. 2003;78:383–90. doi: 10.1093/ajcn/78.3.383. [DOI] [PubMed] [Google Scholar]
- 10.Liu S, Sesso HD, Manson JE, Willett WC, Buring JE. Is intake of breakfast cereals related to total and cause-specific mortality in men? Am J Clin Nutr. 2003;77:594–9. doi: 10.1093/ajcn/77.3.594. [DOI] [PubMed] [Google Scholar]
- 11.Mizrahi A, Knekt P, Montonen J, Laaksonen MA, Heliovaara M, Jarvinen R. Plant foods and the risk of cerebrovascular diseases: a potential protection of fruit consumption. Br J Nutr. 2009;102:1075–83. doi: 10.1017/S0007114509359097. [DOI] [PubMed] [Google Scholar]
- 12.DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled clinical trials. 1986;7:177–88. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 13.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tobias A. Assessing the in fluence of a single study in the meta-analysis estimate. Stata Tech Bull. 1999;47:15–7. [Google Scholar]
- 16.Tang G, Wang D, Long J, Yang F, Si L. Meta-analysis of the association between whole grain intake and coronary heart disease risk. Am J Cardiol. 2015;115:625–9. doi: 10.1016/j.amjcard.2014.12.015. [DOI] [PubMed] [Google Scholar]
- 17.Aune D, Chan DS, Lau R, Vieira R, Greenwood DC, Kampman E, Norat T. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ. 2011;343:d6617. doi: 10.1136/bmj.d6617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Aune D, Norat T, Romundstad P, Vatten LJ. Whole grain and refined grain consumption and the risk of type 2 diabetes: a systematic review and dose-response meta-analysis of cohort studies. Eur J Epidemiol. 2013;28:845–58. doi: 10.1007/s10654-013-9852-5. [DOI] [PubMed] [Google Scholar]
- 19.Adom KK, Liu RH. Antioxidant activity of grains. J Agric Food Chem. 2002;50:6182–7. doi: 10.1021/jf0205099. [DOI] [PubMed] [Google Scholar]
- 20.Adom KK, Sorrells ME, Liu RH. Phytochemicals and antioxidant activity of milled fractions of different wheat varieties. J Agric Food Chem. 2005;53:2297–306. doi: 10.1021/jf048456d. [DOI] [PubMed] [Google Scholar]
- 21.Halvorsen BL, Holte K, Myhrstad MC, Barikmo I, Hvattum E, Remberg SF, Wold AB, Haffner K, Baugerod H, Andersen LF, Moskaug O, Jacobs DR Jr, Blomhoff R. A systematic screening of total antioxidants in dietary plants. J Nutr. 2002;132:461–71. doi: 10.1093/jn/132.3.461. [DOI] [PubMed] [Google Scholar]
- 22.Blomhoff R. Dietary antioxidants and cardiovascular disease. Curr Opin In Lipidol. 2005;16:47–54. doi: 10.1097/00041433-200502000-00009. [DOI] [PubMed] [Google Scholar]
- 23.Dragland S, Senoo H, Wake K, Holte K, Blomhoff R. Several culinary and medicinal herbs are important sources of dietary antioxidants. J Nutr. 2003;133:1286–90. doi: 10.1093/jn/133.5.1286. [DOI] [PubMed] [Google Scholar]
- 24.Halvorsen BL, Carlsen MH, Phillips KM, Bohn SK, Holte K, Jacobs DR Jr, Blomhoff R. Content of redox-active compounds (ie, antioxidants) in foods consumed in the United States. Am J Clin Nutr. 2006;84:95–135. doi: 10.1093/ajcn/84.1.95. [DOI] [PubMed] [Google Scholar]
- 25.Lamming DW, Wood JG, Sinclair DA. Small molecules that regulate lifespan: evidence for xenohormesis. Mol Microbiol. 2004;53:1003–9. doi: 10.1111/j.1365-2958.2004.04209.x. [DOI] [PubMed] [Google Scholar]