

Sir,
We have read with great interest two papers published in your journal about the usefulness of Treponema pallidum hemagglutination (TPHA) test for the serological diagnosis of syphilis.[1,2]
As well mentioned by the authors, the TPHA test is a treponemal assay for the serological confirmation of syphilis, according to the traditional algorithm. It is not accessible in all laboratories and for this reason patients with positive nontreponemal tests are immediately treated with the specific antibiotic schedule, according to national/local guidelines for avoiding the progression or transmission of the illness.[3] However, if the treponemal tests are available we should follow-up the recommendations made by World Health Organization.[4]
Testing for syphilis is an essential skill for all general physicians, but is often perceived as difficult and confusing, and can be a daunting prospect for doctors in training.[5] In this sense, a key point not mentioned in previously stated papers is that nontreponemal and treponemal test results must be interpreted according to the stage of syphilis suspected or the epidemiological history of the patient. The simple understanding of serological results does not define the current physical condition of the patient. Each combination of possible results by these tests has different interpretations in relation to the individual context of each patient [Table 1].
Table 1.
Possible interpretations according to serological results
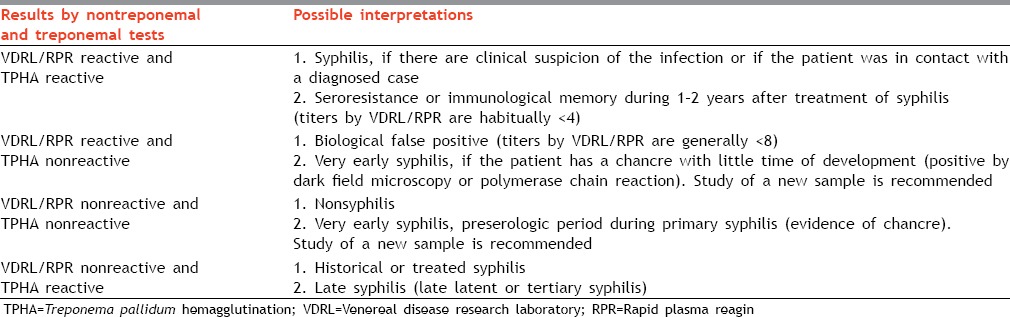
Unfortunately, this information is not always on the analysis submissions and it is vital for the test selection and to conduct certain tests, such as a quantitative nontreponemal assay in sera from patients with nonreactive qualitative results when a clinical suspicion of secondary syphilis is present (due to prozone reaction). Two of our secondary syphilitic patients, diagnosed during 2013, had nonreactive qualitative VDRL/RPR and titers superior to 32 in the quantitative tests, including HIV patients.
We agree with Bala et al recommendation that a confirmatory test such as TPHA should be performed on all sera with a reactive VDRL regardless of its titer[1] as the authors have reported high TPHA positivity (86.8%) in sera with VDRL titres <1:8. Moreover, TPHA is also important for confirming results ≥8 because it is possible to obtain biological false positives (BFP) with these titers in persons with other infectious or noninfectious diseases in which tissue damage occurs.
For example, during 2013 we analyzed 471 sera using VDRL/RPR (Centis, Cuba) and TPHA (Centis, Cuba), 41% (193/471) of them from HIV positive patients. We found reactivity in 52.9% (249/471) of sera suggesting syphilis, 4.2% (20/471) with history of treated syphilis or diagnosis of late syphilis, 15.1% (71/471) of BFP and 27.8% (131/471) without syphilis or in the preserologic period of treponemal infection.
From the sera of BFP, 84.5% (60/71) had titers ≤4 as is expected, 9.9% (7/71) titers of 8, 4.2% (3/71) 16 and 1.4% (1/71) 32. Only HIV status information of these patients was available. The patient with titer of 32 was positive to HIV infection. During 2009 we had another BFP with the same titer in an old woman with hemolytic anemia.
In relation to the use of TPHA for confirming syphilis in pregnant, recognized cause of BFP by nontreponemal tests, we have records of 29.8-37.4% of nonreactive results in gravid with results inferior to 8 by RPR/VDRL and unusually, titers from 8 to 64.
These examples demonstrate the fact that TPHA is essential for the diagnosis of syphilis, irrespective of the VDRL/RPR titer, but the physicians should always consider all other factors such as sexual behavior, medical history, previous treatment history of syphilis, etc. The TPHA is a simple and useful tool for the serological diagnosis of syphilis in both low- and high-prevalence populations.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Bala M, Toor A, Malhotra M, Kakran M, Muralidhar S, Ramesh V. Evaluation of the usefulness of Treponema pallidum hemagglutination test in the diagnosis of syphilis in weak reactive Venereal Disease Research Laboratory sera. Indian J Sex Transm Dis. 2012;33:102–6. doi: 10.4103/2589-0557.102117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Archana BR, Prasad SR, Beena PM, Okade R. Making serological diagnosis of syphilis more accurate. Indian J Sex Transm Dis. 2014;35:70–1. doi: 10.4103/2589-0557.132407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Angue Y, Yauieb A, Mola G, Duke T, Amoa AB. Syphilis serology testing: A comparative study of abbot determine, Rapid Plasma Reagin (RPR) card test and Venereal Disease Research Laboratory (VDRL) methods. P N G Med J. 2005;48:168–73. [PubMed] [Google Scholar]
- 4.Larsen SA, Steiner BM, Rudolph AH. Laboratory diagnosis and interpretation of tests for syphilis. Clin Microbiol Rev. 1995;8:1–21. doi: 10.1128/cmr.8.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ahmed N, French P. Interpretation of syphilis serology. Br J Hosp Med (Lond) 2013;74:C104–7. doi: 10.12968/hmed.2013.74.sup7.c104. [DOI] [PubMed] [Google Scholar]