

Abstract
Posteromedial ankle impingement is a rare clinical entity. It usually follows an inversion injury, with compression of the posterior tibiotalar ligament between the medial malleolus and talus. This can be treated by posterior ankle endoscopy through the posteromedial and posterolateral portals. The flexor hallucis longus tendon can be examined for any tenosynovitis or tendinopathy. The posteromedial corner of the ankle joint is reached with the instruments staying on the lateral side of the flexor hallucis longus tendon. The inflamed synovium, scar tissue, and fibrillated cartilage are debrided.
Posterior ankle pain can be due to soft-tissue pathologies (e.g., Achilles tendinopathy, retrocalcaneal bursitis, and flexor hallucis longus [FHL] tenosynovitis), bony or osteochondral pathologies (e.g., stress fractures, osteochondritis dissecans, and tarsal coalition), and neurovascular causes (e.g., sural nerve entrapment and tarsal tunnel syndrome).1 The deep location of the hindfoot components makes not only direct access and treatment difficult but also the differential diagnosis challenging for posterior ankle pain.1 Posterior ankle impingement is an important cause of posterior ankle pain. Depending on the anatomic location and the structures involved, this impingement can be divided into posterior, posterolateral, and posteromedial ankle impingement syndromes. Posteromedial ankle impingement is an uncommon disease in which a severe injury involves the deep posterior fibers of the medial deltoid ligament.2 We describe an endoscopic approach to deal with posteromedial ankle impingement.
Technique
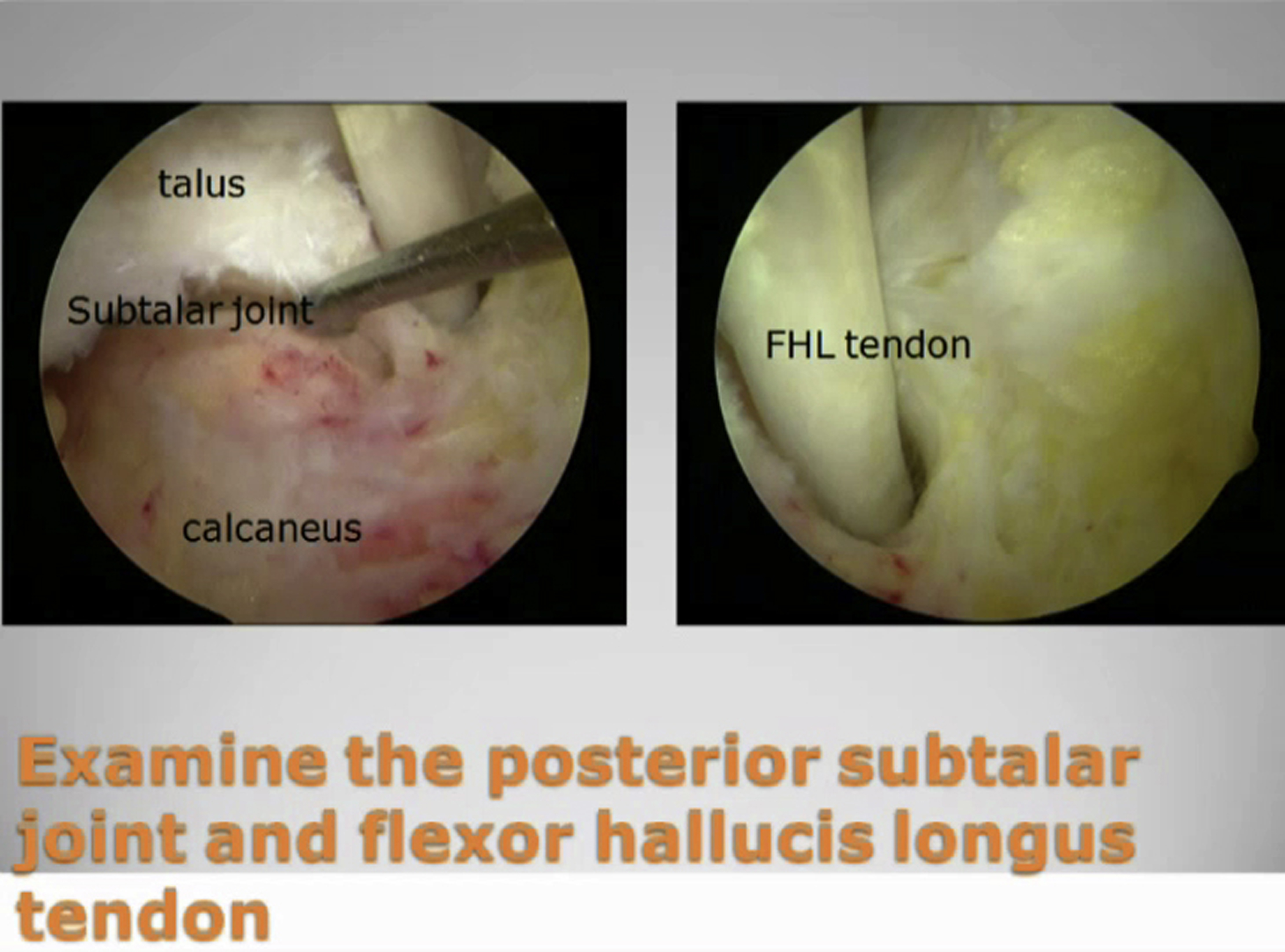
The patient is in the prone position with application of a thigh tourniquet to provide a bloodless surgical field. Posterior ankle endoscopy is performed through the posteromedial and posterolateral portals on the sides of the Achilles tendon just above the posterior calcaneal tubercle.3, 4, 5 A 4.0-mm 30° arthroscope is used for this procedure (Dyonics Smith & Nephew, Andover, MA). The FHL tendon is the key anatomic landmark. With the arthroscope in the posteromedial portal, an arthroscopic shaver (Dyonics Smith & Nephew) is inserted directly anteriorly through the posterolateral portal. In this manner, the shaver will reach the space between the FHL tendon and the peroneal tendons. This is a safe zone in which to start arthroscopic debridement. Once the tendon becomes visible on the medial side of the shaver, it can be confirmed to be the FHL tendon by the presence of muscle fibers at the ankle level, and the tendon will move with passive motion of the hallux. The tendon is examined for any tendinopathic change and tenosynovitis. The inflamed synovium around the FHL tendon, if present, is resected. The portals are switched, with the arthroscopic shaver inserted through the posteromedial portal. The shaver and the arthroscope stay on the lateral side of the FHL tendon, and the FHL tendon is pushed medially by the shaver to expose the posteromedial ankle. The ankle should be kept in a plantar-flexed position to relax the neurovascular bundle at the tarsal tunnel. This can reduce the risk of impingement of the bundle by the shaft of the shaver. Posterior capsulotomy of the posterior subtalar joint is performed, and the posterior aspect of the joint is examined. Release of the intermalleolar ligament and posterior capsulotomy of the ankle joint are performed, and the posterior ankle is examined. Chronic synovitis and fibrosis at the posteromedial ankle and the posteromedial ankle gutter are debrided. The cartilage at the posteromedial aspect of the talus is usually fibrillated because of the impingement. Curettage of the fibrillated cartilage is performed (Video 1). Postoperatively, the patient is advised to perform ankle mobilization exercises and weight-bearing walking.
Discussion
Ankle impingement results from repetitive subclinical trauma due to overuse injuries; ankle impingement, in the subacute or chronic situation, leads to entrapment of anatomic structures, resulting in pain and decreased range of motion of the ankle. It can be classified as either soft tissue or osseous.6, 7 It is characterized by painful limitation of full ankle movement.6 The structures involved in posteromedial ankle impingement include the posteromedial tibiotalar capsule and posterior fibers of the tibiotalar ligament. Their location between the talus and medial malleolus predisposes to the entrapment during supination. The subsequent fibrosis and thickening of the injured posterior tibiotalar ligament and posteromedial capsule cause impingement between the medial wall of the talus and posterior margin of the medial malleolus, resulting in formation of collagenous and fibrous meniscoid lesions and synovitis at the posteromedial ankle.6, 8, 9, 10, 11, 12 The ankle usually shows deep soft-tissue induration and localized tenderness; pain is evocable by palpating the medial retromalleolar area while moving the ankle.2 Posteromedial tenderness on inversion with the ankle in plantar flexion is an important sign to differentiate the ankle pain originating from the tibialis posterior tendon.6, 11
Magnetic resonance imaging has been shown to be an effective investigation in ankle impingement syndromes,6, 7 but it cannot replace careful clinical examination (Fig 1). Sometimes, the exact diagnosis of posterior ankle pain cannot be determined, and posterior ankle endoscopy is an effective diagnostic and therapeutic tool. Detailed examination of the possible causes of posterior ankle pain should be performed during endoscopy (Table 1). Thorough endoscopic debridement can usually relieve the symptoms.1, 2 Posterior ankle endoscopy appears to cause less morbidity than open ankle surgery and facilitates a quick recovery.3, 4 The major potential complication is injury to the tibial neurovascular bundle during debridement of the posteromedial ankle. It has been suggested that keeping the instruments lateral to the FHL tendon can protect the neurovascular bundle; however, the FHL tendon can be pushed medially by the instruments and compress the neurovascular bundle. It may be helpful to keep the ankle in a plantar-flexed position during debridement because this can relax the neurovascular bundle.13 Medial shifting of the FHL tendon may be minimized by instrumentation through the posterolateral portal and visualization through the posteromedial portal. However, this was not shown in the illustrated case, and further cadaveric study is needed to clarify this point. In conclusion, posterior ankle endoscopy is an effective diagnostic and therapeutic tool for posteromedial ankle impingement syndrome.
Fig 1.

Magnetic resonance imaging in the illustrated case showed tenosynovitis of the flexor hallucis longus at the posteromedial aspect of the ankle, whereas intraoperative findings showed synovitis and scarring at the posteromedial ankle instead of flexor hallucis longus tenosynovitis.
Table 1.
Tips for Arthroscopic Management of Posteromedial Ankle Impingement
| Detailed examination of the possible causes of posterior ankle pain should be performed during posterior ankle endoscopy. |
| The arthroscope and shaver should stay lateral to the flexor hallucis longus tendon. |
| The ankle should be in a plantar-flexed position during debridement of the posteromedial ankle. |
Footnotes
The author reports that he has no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Posterior ankle endoscopy was performed with a 4.0-mm 30° arthroscope. The flexor hallucis longus (FHL) tendon was normal without tenosynovitis. The posterior aspect of the posterior subtalar joint was found to be normal. Posterior capsulotomy of the ankle joint was performed, and the FHL tendon was retracted medially to expose the posteromedial aspect of the ankle joint. The distal tibiofibular syndesmosis was intact. There was a patch of chronic synovitis at the posteromedial ankle, with fibrosis at the posteromedial ankle gutter. The cartilage at the posteromedial aspect of the talus was fibrillated. Arthroscopic synovectomy, debridement of the fibrous tissue, and curettage of the fibrillated cartilage were performed. All the instruments were kept on the lateral side of the FHL tendon.
{kind=link}
References
- 1.Ogut T., Ayhan E., Irgit K., Sarikaya A.I. Endoscopic treatment of posterior ankle pain. Knee Surg Sports Traumatol Arthrosc. 2011;19:1355–1361. doi: 10.1007/s00167-011-1428-x. [DOI] [PubMed] [Google Scholar]
- 2.Gasparetto F., Collo G., Pisanu G. Posterior ankle and subtalar arthroscopy: Indications, technique, and results. Curr Rev Musculoskelet Med. 2012;5:164–170. doi: 10.1007/s12178-012-9118-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.van Dijk C.N., de Leeuw P.A.J., Scholten P.E. Hindfoot endoscopy for posterior ankle impingement. Surgical technique. J Bone Joint Surg Am. 2009;91:287–298. doi: 10.2106/JBJS.I.00445. (suppl 2, pt 2) [DOI] [PubMed] [Google Scholar]
- 4.Scholten P.E., Sierevelt I.N., van Dijk C.N. Hindfoot endoscopy for posterior ankle impingement. J Bone Joint Surg Am. 2008;90:2665–2672. doi: 10.2106/JBJS.F.00188. [DOI] [PubMed] [Google Scholar]
- 5.van Dijk C.N., Scholten P.E., Krips R.A. 2-portal endoscopic approach for diagnosis and treatment of posterior ankle pathology. Arthroscopy. 2000;16:871–876. doi: 10.1053/jars.2000.19430. [DOI] [PubMed] [Google Scholar]
- 6.Datir A., Connell D. Imaging of impingement lesions in the ankle. Top Magn Reson Imaging. 2010;21:15–23. doi: 10.1097/RMR.0b013e31820ef46b. [DOI] [PubMed] [Google Scholar]
- 7.Russo A., Zappia M., Reginelli A. Ankle impingement: A review of multimodality imaging approach. Musculoskelet Surg. 2013;97:S161–S168. doi: 10.1007/s12306-013-0286-8. (suppl 2) [DOI] [PubMed] [Google Scholar]
- 8.Messiou C., Robinson P., O’Connor P.J., Grainger A. Subacute posteromedial impingement of the ankle in athletes: MR imaging evaluation and ultrasound-guided therapy. Skeletal Radiol. 2006;35:88–94. doi: 10.1007/s00256-005-0049-1. [DOI] [PubMed] [Google Scholar]
- 9.Giannini S., Buda R., Mosca M., Parma A., Di Caprio F. Posterior ankle impingement. Foot Ankle Int. 2013;34:459–465. doi: 10.1177/1071100713477609. [DOI] [PubMed] [Google Scholar]
- 10.Koulouris G., Connell D., Schneider T., Edwards W. Posterior tibiotalar ligament injury resulting in posteromedial impingement. Foot Ankle Int. 2003;24:575–583. doi: 10.1177/107110070302400802. [DOI] [PubMed] [Google Scholar]
- 11.Paterson R.S., Brown J.N. The posteromedial impingement lesion of the ankle. A series of six cases. Am J Sports Med. 2001;29:550–557. doi: 10.1177/03635465010290050501. [DOI] [PubMed] [Google Scholar]
- 12.Liu S.H., Mirzayan R. Posteromedial ankle impingement. Arthroscopy. 1993;9:709–711. doi: 10.1016/s0749-8063(05)80514-6. [DOI] [PubMed] [Google Scholar]
- 13.Lui T.H. Lateral plantar nerve neuropraxia after FHL tendoscopy: Case report and anatomic evaluation. Foot Ankle Int. 2010;31:828–831. doi: 10.3113/FAI.2010.0828. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Posterior ankle endoscopy was performed with a 4.0-mm 30° arthroscope. The flexor hallucis longus (FHL) tendon was normal without tenosynovitis. The posterior aspect of the posterior subtalar joint was found to be normal. Posterior capsulotomy of the ankle joint was performed, and the FHL tendon was retracted medially to expose the posteromedial aspect of the ankle joint. The distal tibiofibular syndesmosis was intact. There was a patch of chronic synovitis at the posteromedial ankle, with fibrosis at the posteromedial ankle gutter. The cartilage at the posteromedial aspect of the talus was fibrillated. Arthroscopic synovectomy, debridement of the fibrous tissue, and curettage of the fibrillated cartilage were performed. All the instruments were kept on the lateral side of the FHL tendon.