

Abstract
Acquired aplastic anemia is an immune-mediated disease characterized by severe defects in stem cell number resulting in hypocellular marrow and peripheral blood cytopenias. Minor paroxysmal nocturnal hemoglobinuria populations and a short telomere length were identified as predictive biomarkers of immunosuppressive therapy responsiveness in aplastic anemia. We enrolled 113 aplastic anemia patients (63 boys and 50 girls) in this study to evaluate their response to immunosuppressive therapy. The paroxysmal nocturnal hemoglobinuria populations and telomere length were detected by flow cytometry. Forty-seven patients (42%) carried a minor paroxysmal nocturnal hemoglobinuria population. The median telomere length of aplastic anemia patients was −0.99 standard deviation (SD) (range −4.01–+3.01 SD). Overall, 60 patients (53%) responded to immunosuppressive therapy after six months. Multivariate logistic regression analysis identified the absence of a paroxysmal nocturnal hemoglobinuria population and a shorter telomere length as independent unfavorable predictors of immunosuppressive therapy response at six months. The cohort was stratified into a group of poor prognosis (paroxysmal nocturnal hemoglobinuria negative and shorter telomere length; 37 patients) and good prognosis (paroxysmal nocturnal hemoglobinuria positive and/or longer telomere length; 76 patients), respectively. The response rates of the poor prognosis and good prognosis groups at six months were 19% and 70%, respectively (P<0.001). The combined absence of a minor paroxysmal nocturnal hemoglobinuria population and a short telomere length is an efficient predictor of poor immunosuppressive therapy response, which should be considered while deciding treatment options: immunosuppressive therapy or first-line hematopoietic stem cell transplantation. The trial was registered in www.umin.ac.jp with number UMIN000017972.
Introduction
Acquired aplastic anemia (AA) is a rare and fatal bone marrow disorder characterized by hypocellular bone marrow and pancytopenia. Clinical and laboratory studies suggest that its pathogenesis involves cytotoxic T cells attacking hematopoietic stem cells.1 Unfortunately, allogeneic bone marrow transplantation is limited by the availability of human leukocyte antigen (HLA)-matched donors. Most AA patients receive immunosuppressive therapy (IST) combining anti-thymocyte globulin (ATG) and cyclosporine A (CyA).
Currently, the hematopoietic response rate of AA patients for IST is 42–74%, with an overall long-term survival rate of approximately 90%.2–4 Approximately one-third of the patients are not expected to respond to IST, and 20–40% of responders anticipated relapsing after initial therapy.2,3 Furthermore, clonal evolution to myelodysplasia is a more serious problem during follow up. Because those patients eventually require hematopoietic stem cell transplantation (HSCT), biological predictors of patient response to IST may prevent adverse events and the cost of unnecessary treatment. Several conventional clinical parameters were proposed as predictors of a favorable prognosis, such as younger age, male gender, shorter interval between diagnosis and therapy, lower white blood cell count (WBC), higher absolute neutrophil count (ANC), higher absolute lymphocyte count (ALC), and higher absolute reticulocyte count (ARC).5–7 However, their prognostic power is insufficient to affect clinical decision-making, and IST remains the first-line therapy for all AA patients lacking an HLA-matched sibling donor.
Paroxysmal nocturnal hemoglobinuria (PNH) is an acquired disorder associated with the episodic intravascular hemolysis of red blood cells. These cells are deficient in cell surface glycophosphatidylinositol (GPI)-anchored proteins.8,9 Flow cytometry analysis indicated that 20–70% of pediatric AA patients possess minor PNH populations at the time of diagnosis.10–12 However, the reliability of this biomarker remains controversial. For example, several studies conducted on adults and/or children with AA reported that the presence of minor PNH populations was associated with a favorable response to IST.10,11,13–16 In contrast, our previous study of pediatric AA patients as well as a retrospective National Institutes of Health (NIH) study that included adults and children did not show differences between AA patients who did or did not respond to IST.7,12 Short telomeres were proposed as a marker of the aging process because they become shorter with each cell division, which reflects cell turnover.17 In AA patients, significant telomere shortening in lymphocytes is presumed secondary to hematopoietic stress.18 Telomere erosion reduces the replication of hematopoietic stem cells and progenitor cells, although whether telomere length (TL) can predict the response to IST remains a subject of debate. An NIH study reported that base-line TL was not associated with the hematologic response in adult AA patients.19 In contrast, two studies of children with AA suggested that TL at the time of diagnosis was significantly associated with the response to IST.10,20 Here, we studied 113 children diagnosed with acquired AA to determine whether a screening strategy combining minor PNH populations and TL would constitute a reliable predictor of response to IST and prognosis.
Methods
Study population
We retrospectively studied 113 children (63 boys and 50 girls) diagnosed with acquired AA in Japan between July 2001 and November 2013. Patients were tested for a minor PNH population and the TLs of peripheral blood lymphocytes. Patients with acquired AA were eligible if they met the criteria as follows: age below 18 years, newly diagnosed disease (≤180 days) without specific prior treatment, and moderate to very severe symptoms. Patients were excluded if they had congenital bone marrow failure or paroxysmal nocturnal hemoglobinuria with positive Ham test/sucrose test results. The present study included 44 and 63 patients described by Yoshida et al.12 and Sakaguchi et al.,20 respectively. Written informed consent was obtained from the parents of all patients. This study was approved by the ethics committee of Nagoya University Graduate School of Medicine.
The severity of AA was classified as previously described.21 Forty-nine patients received horse ATG (Lymphoglobulin, Genzyme, Cambridge, MA, USA; 15 mg/kg/day for 5 days), and 64 patients received rabbit ATG (Thymoglobulin, Genzyme, Cambridge, MA, USA; 2.5–3.75 mg/kg/day for 5 days). All patients received CyA (6 mg/kg/day) starting on day 1 for at least 180 days. The dose of CyA was adjusted to maintain trough levels of 100–200 ng/mL.
The response to IST was evaluated according to previously described criteria.22 Patients with complete or partial response at six months after IST were defined as responders, and patients with no response were defined as non-responders. Relapse was defined as a conversion from a partial or complete response to no response and/or the requirement of blood transfusions. Clonal evolution was defined as a new clonal cytogenetic abnormality or characteristic dysplastic or leukemic changes in the bone marrow.
Detection of paroxysmal nocturnal hemoglobinuria populations
A flow cytometry assay was used to detect PNH-type granulocytes and red blood cells (RBCs) as previously described.12 Briefly, 5.0×104 or over CD13+ granulocytes or 2.5×105 glycophorin A+ RBCs were analyzed using a FACSCalibur flow cytometer (Becton Dickinson Biosciences, Mississauga, Canada). The presence of more than 0.005% CD13+CD55−CD59− granulocytes and/or more than 0.010% glycophorin A+CD55−CD59− RBCs was defined as PNH positive (PNH+). Cut-off values were determined using ROC analysis.
Measurement of telomere length
The telomere length of peripheral lymphocytes was measured by flow-fluorescence in situ hybridization (flow-FISH), using a Telomere PNA Kit (DakoCytomation, Glostrup, Denmark)23 according to the manufacturer’s instructions. The data of the AA patients were expressed as “delta relative TL” to compare the TL of patients with age-matched healthy controls as previously described.20 According to ROC analysis, we defined −1.21 SD of age-adjusted controls as the cut-off value. We performed targeted gene sequencing which included the known DC genes for 8 patients with telomere lengths shorter than −2.5 SD.
Target gene sequencing
Target sequencing was performed for 88 IBMFS-associated genes using SureSelect Custom (Agilent technologies, Santa Clara, CA, USA) and HiSeq next-generation sequencer (Illumina, San Diego, CA, USA).24,25 The panel of genes for target sequencing included most of the genes related to dyskeratosis congenita (DC) such as DKC1, TERT, TERC, TINF2, NHP2, NOP10, C16orf57, CTC1, RTEL1, WRAP53, POT1, and TERF2IP.
Statistical analysis
To judge patient responses to IST, receiver operator characteristic (ROC) curves were generated to show the relation between sensitivity and the false-positive rate at different cut-off values of PNH and TL. The cut-off value was established according to the best combination of sensitivity and false-positive rate (1–specificity) according to the ROC curves. Differences in base-line characteristics between responders and non-responders were assessed using Fisher’s exact test for categorical variables and the Mann-Whitney test for continuous variables. The correlations between patients’ co-variates and their response to IST at six months were evaluated using univariate and multivariate logistic regression analysis. The co-variates evaluated were as follows: age, gender, etiology, disease severity, types of ATG, interval from diagnosis to treatment, WBC, ANC, ALC, ARC, platelet count, presence of minor PNH population, and delta relative TL.
The probabilities of overall survival (OS), failure-free survival (FFS), and transplantation-free survival (TFS), and the development of relapse and clonal evolution were calculated using the Kaplan-Meier method. We censored no response at six months, relapse, clonal evolution, development of PNH, HSCT, and death from FFS. HSCT and death were censored from TFS. All P values are two-sided; P<0·05 was considered statistically significant. Measures of association were expressed as the hazard ratio (HR) with 95% confidence intervals (CI). All statistical analyses were performed using EZR (Saitama Medical Centre, Jichi Medical University), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria).26
Results
Patients’ characteristics and response to IST
Table 1 shows the clinical characteristics and laboratory findings of the AA patients included in this study. Median age when IST was administered was 9.6 years (range 0.9–16.0 years), disease was moderate-to-very severe, and all three categories of disease severity were well represented. The causes of AA in were idiopathic in 99 patients and hepatitis-associated in 14 patients. Salvage allogeneic bone marrow transplantation (BMT) from related and unrelated donors was administered to 38 patients with refractory AA (n=36) and 2 patients with secondary acute myeloid leukaemia (AML)/myelodysplastic syndrome (MDS). The median follow-up period from the onset of IST was 38 months (range 2–134 months).
Table 1.
Clinical characteristics and laboratory findings of patients with aplastic anemia.
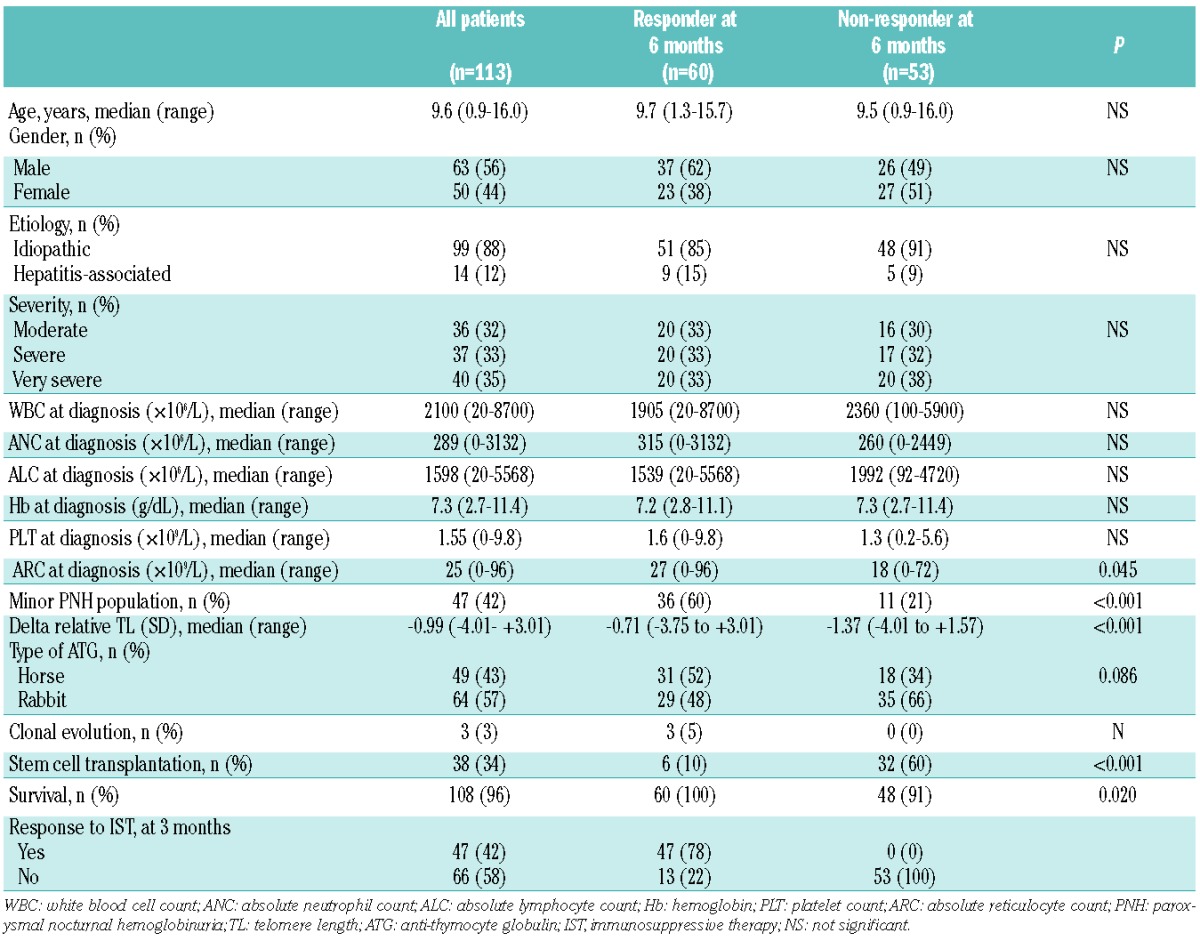
Overall, 60 patients (53%) responded to IST, and 14 and 46 achieved a complete or partial response, respectively, after six months. There was no significant difference between response rates to horse (63%) or rabbit (45%) ATG (P=0.086). There was no difference in base-line values of WBC, ANC, ALC, hemoglobin and platelet count of responders and non-responders. In contrast, significantly more responders were positive for minor PNH populations (P<0.001) and had a longer TL (P<0.001) and higher ARC (P=0.045) compared with non-responders.
Prevalence of PNH-type cells
Forty-seven patients (42%) with a minor PNH population were identified upon diagnosis of AA (Table 1). The median percentage of PNH-type granulocytes and RBCs were 0.000% (range 0.000–5.780%) and 0.001% (range 0.000–7.490%), respectively. Online Supplementary Figure S1 shows the proportions of PNH populations. The response rate to IST at six months was significantly higher in PNH+ patients compared with that of PNH− patients (77% vs. 36%, respectively) (P<0.001) (Figure 1A). No significant difference was observed in other clinical variables between these two groups. ROC curve analysis showed that PNH populations were not strong indicators of response to IST with areas under the ROC curves 0.62 (PNH-type granulocytes) and 0.62 (PNH-type erythrocyte) (Online Supplementary Figure S2).
Figure 1.
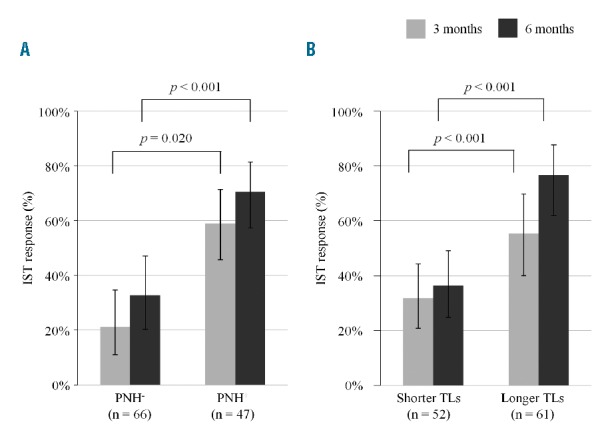
Response rates of immunosuppressive therapy (IST) after three and six months according to (A) minor paroxysmal nocturnal hemoglobinuria (PNH) populations and (B) telomere length (TL). The PNH+ patients showed better responses than the PNH-patients. Patients with normal TLs displayed a significantly higher response rate than those with abnormally shorter TLs.
Telomere length of children with AA
We determined the TL of 113 patients and found that, compared with healthy individuals, patients’ median TL was −0.99 SD (range −4.01–3.01 SD), −0.71 SD (range −3.75–3.01) in responders, and −1.37 SD (range −4.01–1.57) in non-responders (Table 1). Targeted sequencing was performed with the use of bone marrow obtained from the 8 patients with telomere lengths shorter than −2.5 SD compared with those of the healthy cohort. None of them showed clinical features of DC or had detectable germ-line mutations associated with DC. We assigned 52 patients (46%) to the shorter TL group (<−1.21 SD) and the others to the longer TL group. After six months of IST, the response of the longer TL group (71%) was significantly higher compared with that of the shorter TL group (33%) (P<0.001) (Figure 1B). There was no other clinical difference between groups. ROC curve analysis showed that TL was moderate indicators of response to IST with areas under the ROC curves 0.70 (Online Supplementary Figure S2).
Multivariate analysis
Multivariate logistic regression analysis identified lower ARC at diagnosis (OR 3.43; 95%CI: 1.19–9.82; P=0.022), absence of a PNH population (OR 6.50; 95%CI: 2.44–17.30; P<0.001), and a shorter TL (OR 3.61; 95%CI: 1.43–9.11; P=0.007) as independent unfavorable predictors of response to IST at six months (Table 2). Accordingly, the cohort was stratified into poor prognosis [(PNH− and a shorter TL (<−1.21 SD) n=37)] and good prognosis (PNH+ and/or a longer TL, n=76). The response rate at six months of the poor prognosis group was significantly lower (19%) compared with that of the good prognosis group (70%) (P<0.001) (Figure 2). Several parameters reported previously, such as age, gender, interval between diagnosis and therapy, WBC, ANC or ALC, were not independent predictors of the response to IST at six months.
Table 2.
Univariate and multivariate analysis for unfavorable response to IST.
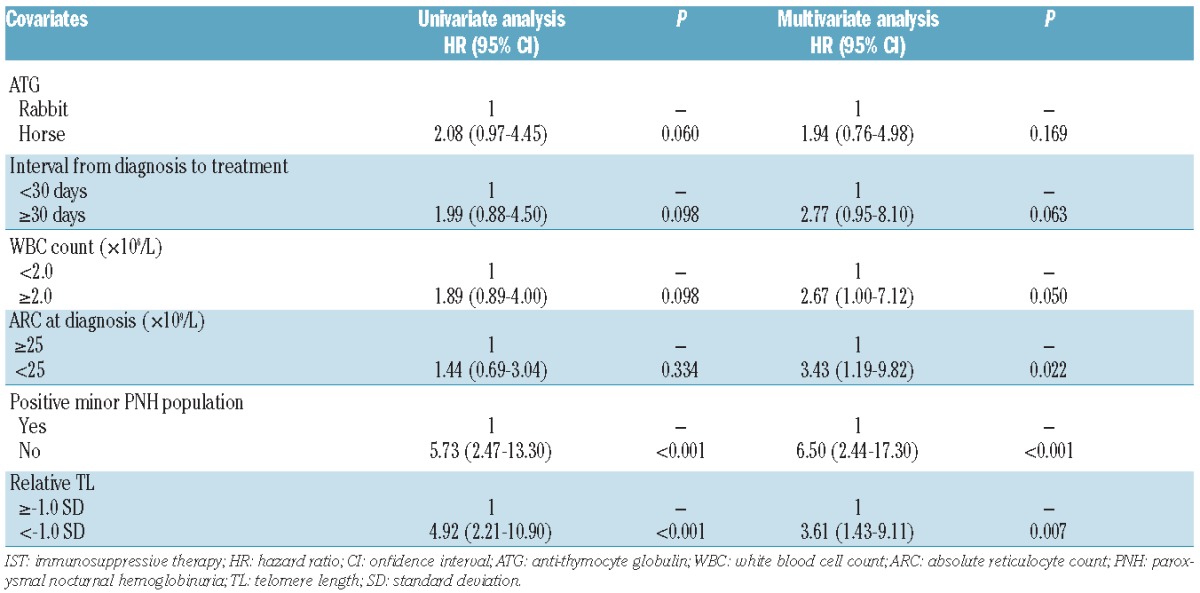
Figure 2.
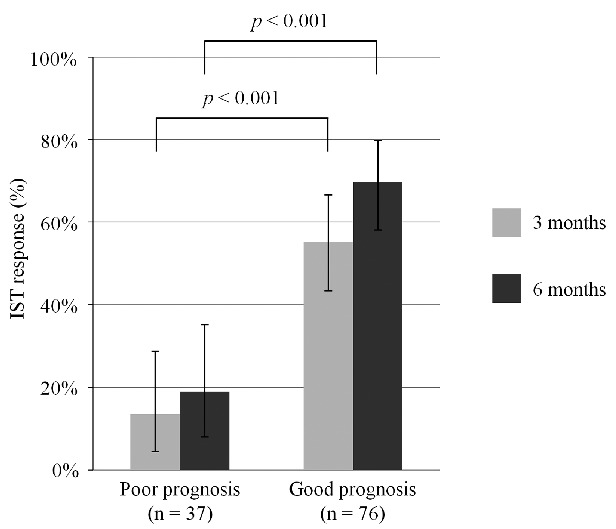
Response rates of immunosuppressive therapy (IST) at three and six months according to predicting stratification. Risk stratification based on minor paroxysmal nocturnal hemoglobinuria (PNH) populations and telomere length (TL) clearly showed worst responses in the unfavorable group than in the favorable group.
Clonal evolution and survival
Among the 60 responders, 10 patients experienced relapse, and their 5-year relapse rate was 15% (95%CI: 3–25%). Clonal evolution appeared in 3 patients after IST with the following characteristics: trisomy 8 (n=1), MDS (n=1), and AML (n=1). Clinical PNH developed in 3 patients who had minor PNH populations at the time of diagnosis. During follow up, 5 non-responders (4%) died. The causes of death were BMT-related complications (n=3), bacteremia (n=1) and intracranial hemorrhage (n=1).
No significant difference was observed between the poor prognosis and good prognosis groups in the probability of 5-year cumulative incidence of relapse [0% (95%CI: 0–0%) vs. 16% (95%CI: 4–27%); P=0.392] and clonal evolution [5% (95%CI: 0–13%) vs. 3% (95%CI: 0–8%); P=0.847] (Figure 3). Five-year TFS and FFS were significantly lower in the poor prognosis group compared with those in the good prognosis group [TFS 48% (95%CI: 29–64%) vs. 72% (95%CI: 59–82%); P=0.003; FFS 22% (95%CI: 9–38%) vs. 52% (95%CI: 39–64%); P<0.001] (Figure 4). However, no difference was observed in 5-year OS between groups [poor prognosis 97% (95%CI: 82–100%) vs. good prognosis 96% (96%CI: 88–99%); P=0.660), possibly because of effective salvage BMT (Figure 4).
Figure 3.

Cumulative incidence after immunosuppressive therapy (IST) in the good prognosis group and the poor prognosis group. (A) Probability of relapse. (B) Probability of clonal evolution.
Figure 4.

Prognosis after immunosuppressive therapy (IST) in the good prognosis and the poor prognosis group. (A) Overall survival. (B) Failure-free survival. (C) Transplantation-free survival.
Discussion
In the present study, PNH+ and longer TL were identified as independent predictors of a favorable response to IST of pediatric AA patients. We designed a simple predicting model based on these markers. The good prognosis group includes patients with PNH+ and/or longer TL, and the poor prognosis group includes patients with PNH-and shorter TL. In the poor prognosis group, only 7 of the 37 patients (19%) responded to IST at six months. Recently, the outcomes of unrelated or mismatched-related donor transplantation for treating AA patients has improved significantly, and an OS in the range of 70–80% is anticipated for selected patients.27,28 In particular, the best results are achieved for young patients with disease duration of less than one year.29 Indeed, the EBMT group reported that up-front matched or mismatched unrelated donor HSCT has similar outcome to matched sibling donor HSCT in idiopathic severe AA of childhood and adolescence.30 Therefore, despite the risk of complications, unrelated or mismatched related donor transplantation may be considered front-line therapy for young patients in the poor prognosis group lacking HLA-matched sibling donors.
The presence of minor PNH populations at the time of AA diagnosis was suggested as a marker of a good hematologic response to IST in studies of adult patients13–16 and in a recent study of children with AA.10 However, our previous study of children contradicts these findings.12 In the current study, we detected a statistically significant effect of the presence of a PNH population on the response to IST. We presume that the discrepancies between studies may be explained by the higher, more sensitive cut-off levels of PNH populations defined by the ROC curve. The evaluation of PNH populations according to relatively low cut-off levels led to concerns about the unreliability of the correlation. Nevertheless, several studies demonstrate that the low prevalence of an increased number of PNH-type cells predict a response to IST.10,14,15 Furthermore, the present study included more AA patients and shows conclusively a correlation between an increase in the proportion of PNH-type cells and a favorable response to IST.
The blood cells of some AA patients have significantly shorter telomeres compared with those of healthy individuals.18,31 Recently, an NIH study found that a short TL, which was unrelated to the response to IST, was associated with the risk of relapse, clonal evolution, and poor OS.19 In contrast, our study of 64 pediatric AA patients identified a prognostic role of lymphocyte TL in the response to IST.20 Here, we analyzed a larger number of patients with newly diagnosed AA and reproduced the association between TL and response to IST. Furthermore, TL was not related to the risk of relapse, clonal evolution, and OS. These conflicting results may be explained by the differences between the present and the NIH study,19 including the methods of TL measurements and patients’ characteristics. For example, the NIH study19 assessed the total leukocyte TL using a quantitative polymerase chain reaction assay, whereas our study measured lymphocyte TL using flow-FISH, which enabled us to measure median TL in subpopulations of blood cells. Considering the possible involvement of T lymphocytes in this disease, the difference in the target-cell population may cause a significant difference. The patients in the current study were much younger compared with those in the NIH study (mean ages 9 vs. 35 years, respectively).19 Age is an important factor for the interpretation of TL. Because telomeres shorten with age, the difference in TL between patients and healthy individuals may become smaller in adults than in children. Recently, Tutelman et al. reported that children with AA who failed to respond to IST had very short granulocyte telomeres for their age.10 However, their study included only 14 patients and there was no statistical analysis.
Our study is limited by the use of two different types of ATG, because horse ATG was withdrawn from the Japanese market and replaced by rabbit ATG in 2008. Another limitation arises from the relatively heterogeneous study population. Our cohort included 32% patients with moderate AA who were treated with early intervention of IST, because published data indicated that the high incidence of disease progression in moderate AA patients with supportive care alone.32 Furthermore, 36 patients received IST late (>30 days), because most presented initially with mild pancytopenia, and they subsequently progressed to severe or very severe AA.
In conclusion, the current study reveals that PNH and TL are predictors of patient responses to IST and combining PNH and TL increased the ability to predict a poor response to IST. Thus, PNH− patients with shorter TL were less likely to respond to IST. Our findings suggest that using these two markers will increase the efficacy of IST and reduce reliance on more promising options, including first-line HSCT.
Acknowledgments
We acknowledge Yoshie Miura for technical assistance.
Footnotes
The online version of this article has a Supplementary Appendix.
Funding
This study was funded by the Ministry of Health and Welfare of Japan (H23-012).
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Young NS, Calado RT, Scheinberg P. Current concepts in the pathophysiology and treatment of aplastic anemia. Blood. 2006;108(8):2509–2519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jeong DC, Chung NG, Cho B, et al. Long-term outcome after immunosuppressive therapy with horse or rabbit antithymocyte globulin and cyclosporine for severe aplastic anemia in children. Haematologica. 2014;99(4):664–671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Scheinberg P, Wu CO, Nunez O, Young NS. Long-term outcome of pediatric patients with severe aplastic anemia treated with antithymocyte globulin and cyclosporine. J Pediatr. 2008;153(6):814–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Locasciulli A, Oneto R, Bacigalupo A, et al. Outcome of patients with acquired aplastic anemia given first line bone marrow transplantation or immunosuppressive treatment in the last decade: a report from the European Group for Blood and Marrow Transplantation (EBMT). Haematologica. 2007;92(1):11–18. [DOI] [PubMed] [Google Scholar]
- 5.Yoshida N, Yagasaki H, Hama A, et al. Predicting response to immunosuppressive therapy in childhood aplastic anemia. Haematologica. 2011;96(5):771–774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chang MH, Kim KH, Kim HS, et al. Predictors of response to immunosuppressive therapy with antithymocyte globulin and cyclosporine and prognostic factors for survival in patients with severe aplastic anemia. Eur J Haematol. 2010;84(2):154–159. [DOI] [PubMed] [Google Scholar]
- 7.Scheinberg P, Wu CO, Nunez O, Young NS. Predicting response to immunosuppressive therapy and survival in severe aplastic anaemia. Br J Haematol. 2009;144(2):206–216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Miyata T, Yamada N, Iida Y, et al. Abnormalities of PIG-A transcripts in granulocytes from patients with paroxysmal nocturnal hemoglobinuria. N Engl J Med. 1994;330(4):249–255. [DOI] [PubMed] [Google Scholar]
- 9.Miyata T, Takeda J, Iida Y, et al. The cloning of PIG-A, a component in the early step of GPI-anchor biosynthesis. Science. 1993;259(5099):1318–1320. [DOI] [PubMed] [Google Scholar]
- 10.Tutelman PR, Aubert G, Milner RA, et al. Paroxysmal nocturnal haemoglobinuria phenotype cells and leucocyte subset telomere length in childhood acquired aplastic anaemia. Br J Haematol. 2014;164(5):717–721. [DOI] [PubMed] [Google Scholar]
- 11.Kulagin A, Lisukov I, Ivanova M, et al. Prognostic value of paroxysmal nocturnal haemoglobinuria clone presence in aplastic anaemia patients treated with combined immunosuppression: results of two-centre prospective study. Br J Haematol. 2014;164(4):546–554. [DOI] [PubMed] [Google Scholar]
- 12.Yoshida N, Yagasaki H, Takahashi Y, et al. Clinical impact of HLA-DR15, a minor population of paroxysmal nocturnal haemoglobinuria-type cells, and an aplastic anaemia-associated autoantibody in children with acquired aplastic anaemia. Br J Haematol. 2008;142(3):427–435. [DOI] [PubMed] [Google Scholar]
- 13.Afable MG, 2nd, Shaik M, Sugimoto Y, et al. Efficacy of rabbit anti-thymocyte globulin in severe aplastic anemia. Haematologica. 2011;96(9):1269–1275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sugimori C, Chuhjo T, Feng X, et al. Minor population of CD55-CD59- blood cells predicts response to immunosuppressive therapy and prognosis in patients with aplastic anemia. Blood. 2006;107(4):1308–1314. [DOI] [PubMed] [Google Scholar]
- 15.Wang H, Chuhjo T, Yamazaki H, et al. Relative increase of granulocytes with a paroxysmal nocturnal haemoglobinuria phenotype in aplastic anaemia patients: the high prevalence at diagnosis. Eur J Haematol. 2001;66(3):200–205. [DOI] [PubMed] [Google Scholar]
- 16.Maciejewski JP, Rivera C, Kook H, et al. Relationship between bone marrow failure syndromes and the presence of glycophosphatidyl inositol-anchored protein-deficient clones. Br J Haematol. 2001; 115(4):1015–1022. [DOI] [PubMed] [Google Scholar]
- 17.Mather KA, Jorm AF, Parslow RA, Christensen H. Is telomere length a biomarker of aging? J Gerontol A Biol Sci Med Sci. 2011;66(2):202–213. [DOI] [PubMed] [Google Scholar]
- 18.Brummendorf TH, Maciejewski JP, Mak J, et al. Telomere length in leukocyte subpopulations of patients with aplastic anemia. Blood. 2001;97(4):895–900. [DOI] [PubMed] [Google Scholar]
- 19.Scheinberg P, Cooper JN, Sloand EM, et al. Association of telomere length of peripheral blood leukocytes with hematopoietic relapse, malignant transformation, and survival in severe aplastic anemia. JAMA. 2010;304(12):1358–1364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sakaguchi H, Nishio N, Hama A, et al. Peripheral blood lymphocyte telomere length as a predictor of response to immunosuppressive therapy in childhood aplastic anemia. Haematologica. 2014;99(8):1312–1316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Camitta BM, Thomas ED, Nathan DG, et al. A prospective study of androgens and bone marrow transplantation for treatment of severe aplastic anemia. Blood. 1979;53(3):504–514. [PubMed] [Google Scholar]
- 22.Kojima S, Hibi S, Kosaka Y, et al. Immunosuppressive therapy using antithymocyte globulin, cyclosporine, and danazol with or without human granulocyte colony-stimulating factor in children with acquired aplastic anemia. Blood. 2000;96(6):2049–2054. [PubMed] [Google Scholar]
- 23.Baerlocher GM, Vulto I, de Jong G, Lansdorp PM. Flow cytometry and FISH to measure the average length of telomeres (flow FISH). Nat Protoc. 2006;1(5):2365–2376. [DOI] [PubMed] [Google Scholar]
- 24.Haferlach T, Nagata Y, Grossmann V, et al. Landscape of genetic lesions in 944 patients with myelodysplastic syndromes. Leukemia. 2014;28(2):241–247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kunishima S, Okuno Y, Yoshida K, et al. ACTN1 mutations cause congenital macrothrombocytopenia. Am J Hum Genet. 2013;92(3):431–438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bacigalupo A, Marsh JC. Unrelated donor search and unrelated donor transplantation in the adult aplastic anaemia patient aged 18–40 years without an HLA-identical sibling and failing immunosuppression. Bone Marrow Transplant. 2013;48(2):198–200. [DOI] [PubMed] [Google Scholar]
- 28.Viollier R, Socie G, Tichelli A, et al. Recent improvement in outcome of unrelated donor transplantation for aplastic anemia. Bone Marrow Transplant. 2008;41(1):45–50. [DOI] [PubMed] [Google Scholar]
- 29.Bacigalupo A, Oneto R, Bruno B, et al. Current results of bone marrow transplantation in patients with acquired severe aplastic anemia. Report of the European Group for Blood and Marrow transplantation. On behalf of the Working Party on Severe Aplastic Anemia of the European Group for Blood and Marrow Transplantation. Acta Haematol. 2000; 103(1):19–25. [DOI] [PubMed] [Google Scholar]
- 30.Dufour C, Pillon M, Carraro E, et al. Similar Outcome of Upfront Unrelated and Matched Sibling Donor Hematopoietic Stem Cell Transplantation in Idiopathic Anlastic Anaemia of Childhood and Adolescence: A Cohort Controlled Study on Behalf of the UK Paediatric BMT WP, of the PD WP and of the SAA WP of the EBMT. Blood. 2014;124(21). [Google Scholar]
- 31.Ball SE, Gibson FM, Rizzo S, et al. Progressive telomere shortening in aplastic anemia. Blood. 1998;91(10):3582–3592. [PubMed] [Google Scholar]
- 32.Nishio N, Yagasaki H, Takahashi Y, et al. Natural history of transfusion-independent non-severe aplastic anemia in children. Int J Hematol 2009;89(4):409–413. [DOI] [PubMed] [Google Scholar]