

Multiple myeloma (MM) is a hematologic cancer caused by malignant plasma cells in the bone marrow. A characteristic feature of this cancer is the destruction of bone, which affects nearly all myeloma patients. The osteolytic bone disease is caused by an increased number and activity of osteoclasts, combined with a reduced number and dysfunction of osteoblasts.1
Growth differentiation factor 15 (GDF15) is a member of the transforming growth factor-beta family that has been shown to play a role in several types of cancer, inflammation, cardiovascular disease and many other pathologies.2 Stromal cells in the bone marrow of MM patients overexpress GDF15,3,4 and high levels of GDF15 in the circulation of myeloma patients are associated with a poor prognosis.4,5 Moreover, GDF15 was recently shown to enhance the tumor-initiating and self-renewal potential of malignant plasma cells, as well as conferring drug resistance.4,5
The effects of GDF15 on bone cells are unclear. One study demonstrated an important role for GDF15 in bone remodeling during hypoxia.6 In particular, GDF15 produced by osteocytes promoted osteoclast differentiation both in vitro and in vivo.6 Moreover, GDF15 was shown to promote osteoclast formation in prostate cancer metastasizing to bone.7 In contrast, another study showed that GDF15 inhibited osteoclast formation in vitro.8 These studies were, however, performed on mouse bone marrow mononuclear cells or murine macrophage-like cell lines, and how GDF15 affects human osteoclast differentiation is not reported. Moreover, little is known on how GDF15 affects osteoblast differentiation. Hence, we wanted to characterize the effect of GDF15 on the differentiation of human osteoclasts and osteoblasts and to measure GDF15 in serum from a well-characterized cohort of myeloma patients to see whether high GDF15 levels are associated with osteolytic bone disease.
GDF15 was measured by a multiplex assay (The MILLIPLEX MAP Human Cancer/Metastasis Biomarker Panel 1, Millipore Corporation, Billerica, MA, USA) in serum samples obtained at diagnosis from 138 myeloma patients and 58 age- and sex-matched healthy controls. Out of 21 tested cytokines, 12 were differently expressed in patients compared with controls (for the full list and details on multiple testing correction, see Online Supplementary Data).9 The patients’ samples were collected for the Nordic Myeloma Study Group during a randomized, phase 3 clinical trial which compared the effect of two different doses of pamidronate on bone. The bone disease was, therefore, particularly well characterized in this study.10, 11
We found that the concentration of GDF15 was significantly higher in serum obtained from myeloma patients (median 1.08 ng/mL; range, 0.17–28.08) than from healthy controls (median 0.46 ng/mL; range, 0.02–1.68; independent samples Kruskal-Wallis test P≤0.0001, corrected for multiple comparisons, P≤0.02) (Figure 1A). Moreover, the level of serum GDF15 was higher in patients with more advanced osteolytic bone disease (>3 osteolytic lesions, n=51, median 1.44 ng/mL; range, 0.30–6.78) than in patients without osteolytic lesions (n=16, median 0.84 ng/mL; range, 0.22–10.84) at inclusion (P<0.05, Dunn multiple comparison test) (Figure 1B), supporting the concept that GDF15 might play a role in myeloma bone disease. The difference in serum GDF15 levels between myeloma patients with limited bone disease (≤3 osteolytic lesions, n=51, median 1.07 ng/mL; range, 0.17–7.01) and myeloma patients with no bone disease, and the difference between myeloma patients with osteoporosis but no lesions (n=14, median 1.01 ng/mL; range, 0.36–4.26) and myeloma patients with no bone disease were not statistically significant. Skeletal-related events (defined as pathological fractures, radiotherapy or surgery to bone, new vertebral compression, symptomatic new or progressive osteolytic lesions and hypercalcemia) were evaluated every third month.10 For patients with serum GDF15 levels equal to or less than the median serum GDF15 level (GDF15 ≤1.08 ng/mL, n=65), the time to skeletal-related events was not reached, while estimated time from inclusion to skeletal-related events in the group of patients with serum GDF15 >1.08 ng/mL was 35 months (n= 59). This difference was not, however, statistically significant (P=0.08 log-rank test, Figure 1C). The median time from inclusion to skeletal-related events for the whole group of patients with recorded skeletal status was 42 months (n=124). In line with what has been reported previously5 we found that low serum GDF15 concentration was associated with better overall survival: the median survival of patients who had a serum GDF15 ≤1.08 ng/mL (n=69) was estimated to be 82 months, while the median survival for patients with GDF15 levels above 1.08 ng/mL was estimated to be 35 months (P=0.002, log-rank test) (Figure 1D). The overall median survival for the 138 myeloma patients was estimated to be 59 months. An increase in serum GDF15 levels of 1 ng/mL led to an increased risk of death of 1.187 (univariate Cox regression, P<0.001).
Figure 1.
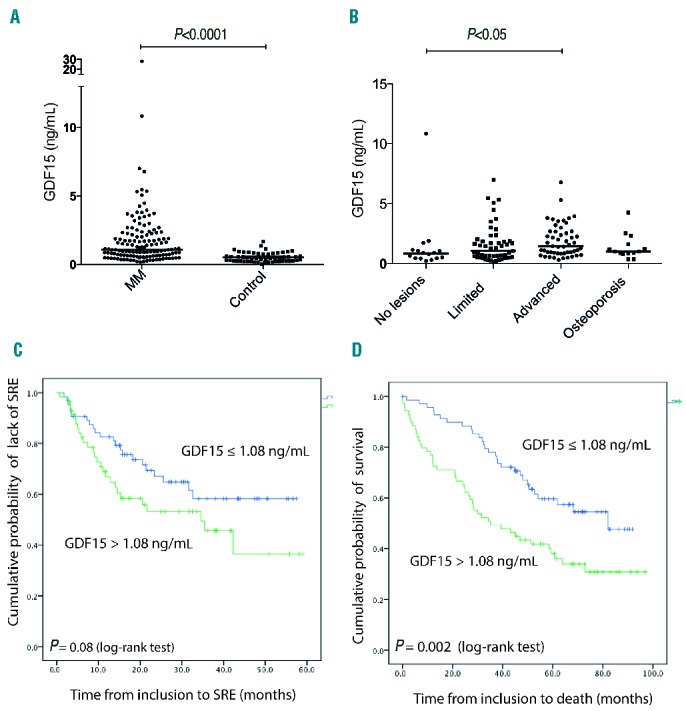
GDF15 serum levels in myeloma patients at the time of diagnosis are higher in patients with osteolytic lesions. (A) GDF15 was measured in serum samples from MM patients (n=138) and healthy controls (n=58). Differences between groups were analyzed by the Kruskal-Wallis test and bars indicate median values. (B) Bone disease status at inclusion was available for 132 of the myeloma patients, and the patients were divided into groups based on degree of bone destruction: limited, ≤3 osteolytic lesions (n=51), advanced, >3 osteolytic lesions (n=51) and diffuse osteoporosis, without lesions (n=14). Serum GDF15 levels in these groups were compared with serum GDF15 levels in patients without bone disease (n=16) using the Dunn multiple comparison test. Bars indicate median values. (C) Kaplan-Meier plot of the appearance of skeletal-related events (SRE) in myeloma patients with serum GDF15 ≤1.08 ng/mL or GDF15 >1.08 ng/mL. (D) Kaplan-Meier plot of survival in myeloma patients with serum GDF15 ≤1.08 ng/mL or GDF15 >1.08 ng/mL.
Importantly, levels of serum GDF15 correlated with levels of markers for osteoclast activity, carboxy-terminal crosslinked telopeptide of type I collagen (CTX1) (Spearman rho 0.40, P≤0.001) and carboxy-terminal crosslinked telopeptide of type I collagen generated by matrix metalloproteinases (ICTP) (Spearman rho 0.63, P≤0.001), supporting an association between high GDF15 levels and increased osteoclast activation. In contrast, serum GDF15 concentration did not correlate with markers of osteoblast activity, bone-specific alkaline phosphatase (rho −0.06, P=0.52) or amino-terminal propeptide of procollagen (PINP) (rho 0.15, P=0.07).
To evaluate the effect of GDF15 on osteoclast differentiation in vitro we differentiated osteoclasts from peripheral blood mononuclear cells (n=3) or from purchased pre-osteoclasts (Lonza Inc., Allendale, NJ, USA; n=2). The cells were cultured in osteoclast medium [a-MEM with human serum (20%), macrophage colony-stimulating factor (M-CSF; 30 ng/mL) and receptor activator of NF-κB ligand (RANKL; 50 ng/mL)] for up to 14 days with or without GDF15 and thereafter stained for tartrate resistant acid phosphatase (TRAP). We found that GDF15 dose-dependently increased the number of multinucleated TRAP-positive cells differentiated from peripheral blood mononuclear cells (Figure 2A,B). When we used pre-osteoclasts as precursor cells, however, the optimal concentration was in the lower range (2–20 ng/mL) while higher concentrations had no effect (Online Supplementary Figure S1). GDF15 could not promote osteoclast differentiation in the absence of RANKL (data not shown), and the effect of GDF15 was inhibited by osteoprotegerin, suggesting that GDF15 acts cooperatively with RANKL. Hence, our results support previous studies showing an osteoclast-promoting effect of GDF15.6,7
Figure 2.

GDF15 promotes osteoclastogenesis and inhibits osteoblastogenesis in vitro. (A) Peripheral blood monocytes were treated with macrophage colony-stimulating factor (M-CSF) (30 ng/mL) and left to differentiate in the presence of RANKL (50 ng/mL) with or without osteoprotegerin (OPG 200 ng/mL) and various concentrations of GDF15 as indicated. On day 14 TRAP-positive multinucleated cells were counted. Error bars = SEM of triplicate wells. The figure shows one representative experiment out of three. (B) Representative images of TRAP-stained osteoclasts. (C) Alkaline phosphatase (ALP) activity/μg DNA was determined in human bone marrow-derived mesenchymal stem cells (hMSC) differentiated in osteogenic medium containing L-ascorbic acid (50 mM), dexamethasone (10−8 M) and β-glycerophosphate (10 mM) for 7 days. Error bars = SEM of triplicate wells. (D) hMSC were differentiatied for 17 days in osteogenic media and stained with alizarin red-S (ARS) to quantify degree of mineralization. Error bars = SEM of duplicate experiments. (E) mRNA expression of RUNX2, (F) COL1A1 and (G) BGLAP in hMSC at day 7 after differentiation. Bars represent mean of triplicate experiments, error bars represent maximal relative quantity. The figure shows one representative experiment of three.
To investigate whether GDF15 influences osteoblast differentiation in vitro we cultured human bone marrow-derived mesenchymal stem cells (Lonza Inc., Allendale, NJ, USA) (n=3) in osteogenic medium containing L-ascorbic acid (50 mM), dexamethasone (10−8M) and β-glycerophosphate (10 mM) in the presence or absence of GDF15 for up to 17 days. Alkaline phosphatase activity is considered an early marker of osteoblast differentiation, and was quantified after 7 days as described previously.12 In all donors, GDF15 dose-dependently inhibited alkaline phosphatase-activity (Figure 2C). Moreover, late differentiation, as evaluated by the cells’ ability to mineralize matrix, was reduced in the presence of GDF15 (Figure 2D,E). Supporting reduced differentiation in the presence of GDF15, mRNA levels of osteoblast markers RUNX2, type I collagen (COL1A1) and osteocalcin (bone gamma-carboxyglutamic acid-containing protein, BGLAP) were decreased upon GDF15 treatment (Figure 2F–H).
GDF15 influenced in vitro differentiation of osteoclasts and osteoblasts at concentrations ranging from 5–100 ng/mL, while the median concentration of GDF15 in serum obtained from myeloma patients was 1.08 ng/mL (Figure 1A). To compare levels of GDF15 in bone marrow plasma with levels in blood serum we measured GDF15 by the multiplex assay (Millipore) in a set of paired bone-marrow plasma and serum samples obtained from myeloma patients (n=16) (Online Supplementary Figure S2). In accordance with previously published data,5 there was a strong correlation between bone marrow plasma levels and serum levels (Spearman rho = 0.97, P<0.0001), which implies that levels of GDF15 in serum reflect levels of GDF15 in bone marrow. In our set of samples levels in bone marrow plasma appeared approximately 25% lower than levels in serum (Online Supplementary Figure S2). However, this was not observed in a previous study.5 Unprocessed GDF15 is stored in extracellular matrix,13 and might be activated/released locally. Hence, future studies should address the relationship between circulating levels of GDF15 and levels locally in the bone marrow, and whether GDF15 in concentrations found locally in myeloma bone marrow influence bone homeostasis in vivo. Importantly, levels of GDF15 in bone marrow plasma from myeloma patients were elevated compared with levels in bone marrow plasma from healthy persons,5 suggesting that cells in myeloma bone marrow are exposed to higher concentrations of GDF15 than cells in a healthy bone marrow.
In conclusion, serum GDF15 levels are elevated in myeloma patients with advanced osteolytic bone disease compared to the levels in patients with no lesions, and correlate with serum markers for osteoclast activity. We found that GDF15 increases osteoclast differentiation and at the same time inhibits osteoblast differentiation in vitro. Hence, GDF15 might play a role in uncoupling bone formation and resorption in multiple myeloma. Our results presented here and recent reports by others4,5 suggest that GDF15 may be of interest as a target for treatment of multiple myeloma.
Acknowledgments
We thank Berit Størdal for excellent technical assistance.
Footnotes
Funding: the work was supported by the Norwegian Cancer Society (project ID 450930), the K.G. Jebsen Foundation and the Cancer Foundation at St Olavs Hospital.
The online version of this letter has a Supplementary Appendix.
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Yaccoby S. Advances in the understanding of myeloma bone disease and tumour growth. Br J Haematol. 2010;149(3):311–321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Unsicker K, Spittau B, Krieglstein K. The multiple facets of the TGF-beta family cytokine growth/differentiation factor-15/macrophage inhibitory cytokine-1. Cytokine Growth Factor Rev. 2013;24(4):373–384. [DOI] [PubMed] [Google Scholar]
- 3.Corre J, Mahtouk K, Attal M, et al. Bone marrow mesenchymal stem cells are abnormal in multiple myeloma. Leukemia. 2007;21(5):1079–1088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tanno T, Lim Y, Wang Q, et al. Growth differentiating factor 15 enhances the tumor-initiating and self-renewal potential of multiple myeloma cells. Blood. 2014;123(5):725–733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Corre J, Labat E, Espagnolle N, et al. Bioactivity and prognostic significance of growth differentiation factor GDF15 secreted by bone marrow mesenchymal stem cells in multiple myeloma. Cancer Res. 2012;72(6):1395–1406. [DOI] [PubMed] [Google Scholar]
- 6.Hinoi E, Ochi H, Takarada T, et al. Positive regulation of osteoclastic differentiation by growth differentiation factor 15 upregulated in osteocytic cells under hypoxia. J Bone Miner Res. 2012;27(4):938–949. [DOI] [PubMed] [Google Scholar]
- 7.Wakchoure S, Swain TM, Hentunen TA, et al. Expression of macrophage inhibitory cytokine-1 in prostate cancer bone metastases induces osteoclast activation and weight loss. Prostate. 2009;69(6):652–661. [DOI] [PubMed] [Google Scholar]
- 8.Vanhara P, Lincova E, Kozubik A, Jurdic P, Soucek K, Smarda J. Growth/differentiation factor-15 inhibits differentiation into osteoclasts–a novel factor involved in control of osteoclast differentiation. Differentiation. 2009;78(4):213–222. [DOI] [PubMed] [Google Scholar]
- 9.Olsen OE, Wader KF, Misund K, et al. Bone morphogenetic protein-9 suppresses growth of myeloma cells by signaling through ALK2 but is inhibited by endoglin. Blood Cancer J. 2014;4:e196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gimsing P, Carlson K, Turesson I, et al. Effect of pamidronate 30 mg versus 90 mg on physical function in patients with newly diagnosed multiple myeloma (Nordic Myeloma Study Group): a double-blind, randomised controlled trial. Lancet Oncol. 2010;11(10):973–982. [DOI] [PubMed] [Google Scholar]
- 11.Mylin AK, Abildgaard N, Johansen JS, et al. Serum YKL-40: a new independent prognostic marker for skeletal complications in patients with multiple myeloma. Leuk Lymphoma. 2015;1–10. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 12.Standal T, Abildgaard N, Fagerli UM, et al. HGF inhibits BMP-induced osteoblastogenesis: possible implications for the bone disease of multiple myeloma. Blood. 2007;109(7):3024–3030. [DOI] [PubMed] [Google Scholar]
- 13.Bauskin AR, Brown DA, Junankar S, et al. The propeptide mediates formation of stromal stores of PROMIC-1: role in determining prostate cancer outcome. Cancer Res. 2005;65(6):2330–2336. [DOI] [PubMed] [Google Scholar]