

Abstract
Background
The purpose of this study was to report findings of exploratory arthroscopic assessment performed in conjunction with removal of internal fixation device placed in the initial surgery for rotational ankle fracture.
Methods
A total of 53 patients (33 male, 20 female) who underwent surgery for rotational ankle fracture between November 2002 and February 2008 were retrospectively reviewed. All patients gave consent to the exploratory arthroscopic surgery for the removal of internal fixation devices placed in the initial surgery. Lauge-Hansen classification system of ankle fractures was assessed for all patients. Intra-articular lesions (osteochondral lesion, loose body, and fibrosis) were evaluated via ankle arthroscopy. Comparative analysis was then performed between radiological classification of ankle fracture/patient's symptoms and arthroscopic findings.
Results
Lauge-Hansen classification system of ankle fractures included supination-external rotation type (n = 35), pronation-external rotation type (n = 9), and pronation-abduction type (n = 9). A total of 33 patients exhibited symptoms of pain or discomfort while walking whereas 20 exhibited no symptoms. Arthroscopic findings included abnormal findings around the syndesmosis area (n = 35), intra-articular fibrosis (n = 51), osteochondral lesions of the talus (n = 33), loose bodies (n = 6), synovitis (n = 13), and anterior bony impingement syndrome (n = 3). Intra-articular fibrosis was seen in 31 of symptomatic patients (93.9%). Pain or discomfort with activity caused by soft tissue impingement with meniscus-like intra-articular fibrosis were found in 19 patients. There was statistical significance (p = 0.02) between symptoms (pain and discomfort) and the findings of meniscus-like fibrosis compared to the group without any symptom.
Conclusions
Arthroscopic examination combined with treatment of intra-articular fibrosis arising from ankle fracture surgery may help improve surgical outcomes.
Keywords: Ankle fracture, Arthroscopy, Fibrosis
Arthroscopy of the ankle is a diagnostic and therapeutic procedure for ankle pains. In the past 15 years, clinical experience and the role of arthroscopy has becoming increasingly important.1,2,3) Untreated intra-articular lesion caused by ankle fracture is one of the major factors that hinder the recovery after ankle fracture surgery. Rotational ankle fractures are frequently accompanied by intra-articular damage involving chondral defect, loose body of bone or cartilage, ligament injury, and fibrosis during treatment and rehabilitation. Such damage could lead to impairment to the ankle joint function.4,5)
There are few studies in the literature regarding the evaluation of intra-articular damage accompanied with ankle fractures or the mechanism involved in the functional impairment of the ankle after the occurrence of the fracture. Therefore, the objective of this study was to investigate the causal relationship between intra-articular damage and ankle fracture. For this study, we enrolled patients who had undergone surgery for fracture around the ankle with consent to undergo exploratory arthroscopic surgery with the removal of internal fixation devices. Here we report the results of our study along with a relevant literature review.
METHODS
Material and Methods
A total of 53 patients (33 male, 20 female) who had undergone surgery for rotational ankle fracture between November 2002 and February 2008 with consent to undergo exploratory arthroscopic surgery with the removal of the internal fixation devices were retrospectively reviewed in this study. Computed tomography (CT) scan was performed as routinely preoperative evaluation for all patients. Soft tissue lesion was evaluated on CT scan. Our study was intended for patients without intra-articular lesions. The average follow-up period between the initial fracture surgery and second-look arthroscopy was 12.3 months (range, 1.5 to 56 months). The average age of patients was 40.98 years (range, 13 to 80 years).
All patients underwent surgical treatment (open reduction and internal fixation) for ankle fracture. Using Lauge-Hansen classification system, the fractures of patients were categorized to the following type: supination-external rotation, pronation-external rotation, pronation-abduction, or supination-adduction. In the final evaluation before the removal of the internal fixation devices, patients were included in the symptomatic group if they exhibited pain or foreign-body sensations while walking. Patients were assigned to the asymptomatic group if they did not exhibit pain or foreign-body sensation. Intra-articular lesions such as osteochondral lesions, intra-articular loose body, and articular fibrosis were analyzed via arthroscopy. Chondral lesions were differentiated into four stages while fibrosis was classified into three stages. A comparative analysis was also performed between radiological classification/symptoms and arthroscopic findings.
The classification of chondral lesions was based on the staging system for osteochondral lesions of the talus proposed by Berndt and Harty.6) The first stage was a small area of compression in the subchondral bone. The second stage was partially detached osteochondral fragment. The third stage was completely detached with non-displaced osteochondral fragment. The fourth stage was detached with displaced osteochondral fragment. The classification of intra-articular fibrosis was based on the staging system presented by Utsugi et al.3) Stage B0 denoted no fibrosis. Stage B1 was for mild fibrosis presenting no evidence of impingement. Stage B2 denoted extensive fibrosis with impingement (either soft tissue impingement or bony impingement).
Arthroscopy Technique
All patients had undergone the removal of internal fixation devices as well as arthroscopy. Exploratory arthroscopic surgery was performed by the same surgeon. Patients were administered with either general anesthesia or spinal anesthesia. A surgical tourniquet was applied onto proximal thigh in supine position. Conventional orthopedic surgical preparations were made before the procedure.
First, the internal fixation device was removed and the knee joint was extended. The posterior portion of the ankle joint was supported using a small surgical drape to preemptively prevent the talus from becoming translated anteriorly. An anteromedial portal was created on the medial side of the anterior tibialis tendon around the ankle joint. The portal was used to examine the anterior, medial, and the lateral side of the ankle joint with a 2.7-mm, 30° arthroscope (EZ-3, Smith & Nephew, Memphis, TN, USA). An anterolateral portal was then created at the lateral side of the peroneus tertius tendon. At this point, the light of the arthroscope was used to examine the superficial peroneal nerve's location in the anteromedial portal to prevent damage. For two cases where the posterior side of the ankle was difficult to examine via anteromedial or anterolateral portals, a posterolateral portal was used. During the procedure, the joint space was outstretched to ease the procedure through manual traction. With respect to the treatment of lesions observed during exploratory arthroscopy, articular debridement was performed for intra-articular fibrosis and synovitis while transmalleolar multiple drilling or microfracture was performed for osteochondral lesions. Arthroscopic removal was performed for intra-articular loose bodies.
Findings related to distal tibio-fibular syndesmotic abnormality were defined as fibrous scarring, hyperplasia, or ligament laxity by examining anterior and posterior tibiofibular ligament. For statistical analysis, results were verified using chi-square test. SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) was used for analysis. Statistical significance was considered when p-value was less than 0.05.
RESULTS
According to the Lauge-Hansen classification system for the fractures, there were 35 cases of supination-external rotation type, nine cases of pronation-external rotation type, and nine cases of pronation-abduction type. There was no case of supination-adduction or pronation-dorsiflexion. During the final evaluation prior to the removal of internal fixation devices, 33 patients reported symptoms of pain or discomfort while performing physical activities while 20 patients reported no symptoms.
Arthroscopic findings revealed 33 cases of distal tibiofibular syndesmotic abnormalities, 51 cases of intra-articular fibrosis (26 cases of local fibrosis, 25 cases of diffuse fibrosis, and 21 cases of meniscus-like fibrosis, regardless of extensiveness), 33 cases of osteochondral lesions, 6 cases of intra-articular loose bodies, 13 cases of systemic synovitis, and 3 cases of anterior bony impingement syndrome (Table 1).
Table 1. The Results of Arthroscopic Assessment of Intra-Articular Pathologies in Entire Patients.
| Arthroscopic finding | No. of patients |
|---|---|
| Syndesmosis injury | 33 |
| Focal fibrosis | 26 |
| Diffuse fibrosis | 25 |
| Meniscus-like fibrosis | 21 |
| Osteochondral lesion | 33 |
| Loose body | 6 |
| Synovitis | 13 |
| Anterior impingement syndrome | 3 |
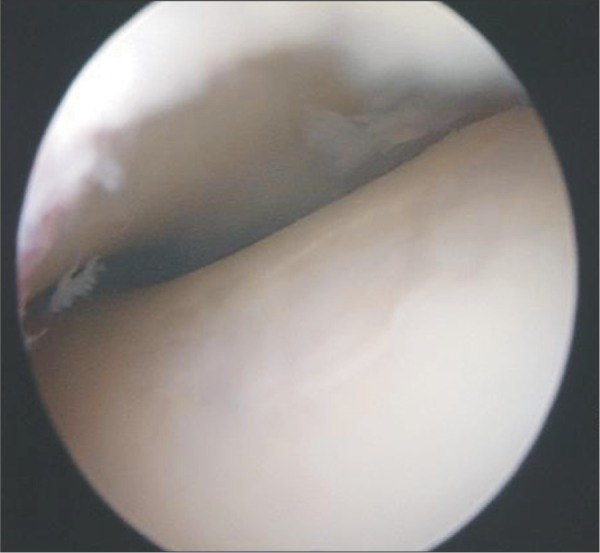
Of the 33 symptomatic patients, 21 had distal tibiofibular syndesmotic abnormalities, 31 had fibrosis (16 cases of local fibrosis, 15 cases of diffuse fibrosis, and 19 cases of meniscus-like fibrosis, regardless of extensiveness), 22 had osteochondral lesions, five had intra-articular loose bodies, 8 had synovitis, and 3 had anterior bony impingement syndrome. Of the 20 asymptomatic patients, 12 had distal tibiofibular syndesmotic abnormalities, 20 had fibrosis (10 cases of local fibrosis, 10 cases of diffuse fibrosis, and two cases of meniscus-like fibrosis, regardless of extensiveness), 11 had osteochondral lesions, one had intra-articular loose bodies, and five had synovitis (Fig. 1). No case showed anterior bony impingement syndrome. There was no statistical significance between symptoms and osteochondral lesions, synovitis, loose bodies, or Utsugi et al.3)'s B1, B2 stage fibrosis. There was only statistical significance (p = 0.02) between symptoms and the findings of meniscus-like fibrosis (Fig. 2). Among the 21 patients with meniscus-like fibrosis, 16 showed fibrosis in the anterolateral side of the tibiotalar joint.
Fig. 1. Results of arthroscopic assessment of symptomatic and asymptomatic patients.

Fig. 2. (A) A meniscus-like fibrotic scar tissue is seen in the anterolateral area of the tibiotalar joint. (B) A cord-like fibrotic scar tissue is seen in the anterolateral area of the tibiotalar joint. It can cause some impingement symptoms such as pain or discomfort with activities.

When the fracture classification system and intra-articular lesions were compared and analyzed, a high incidence of intra-articular lesions was observed in supination-external rotation fracture and pronation-external rotation fracture. However, the results were not statistically significant (Fig. 3). According to the arthroscopic findings, the presence of external rotation fracture was related to increased frequency of intra-articular lesions and poor prognosis. However, the aforementioned observation failed to show statistical significance (Fig. 4).
Fig. 3. Arthroscopic findings and fracture types. SER: supination external rotation, PER: pronation external rotation, PA: pronation-abduction injury.

Fig. 4. Arthroscopic findings according to the stage of supination external rotation (SER) injury (A), pronation external rotation (PER) injury (B), and pronation-abduction (PA) injury (C).

DISCUSSION
Improvement in clinical outcomes cannot always be expected after surgical treatment of ankle fractures.4,5) Postoperative pain and discomfort caused by intra-articular lesions might be usually overlooked during the initial surgery. Osteochondral lesions of the talus are commonly observed in rotational ankle fractures. These lesions can lead to undesirable clinical results even after treatment for the fracture.3,7,8)
Takao et al.9) have reported that 73.2% of patients who underwent simultaneous open reduction internal fixation and exploratory arthroscopic surgery had chondral lesions. Utsugi et al.3) have found chondral lesions in 33% of patients who have undergone exploratory arthroscopic surgery at an average of 12.4 months after the initial fracture. The low incidence of chondral lesions suggests that chondral lesions might have been recovered during the evaluation period. However, Thomas et al.2) have found osteochondral lesions in 90% of patients who had chronic ankle pain with ankle fractures via arthroscopy. In our study, osteochondral lesions were observed in 60.3% of patients. Considering that the evaluation period up to arthroscopy was long, more chondral lesions existing in the initial fracture period might have healed after surgery. Utsugi et al.3) have pointed out that the incidence of chondral lesions at the time of initial surgery cannot be verified as a limitation of their study. Therefore, we cannot conclude that there is a definitive decrease in the number of lesions during the healing period of ankle fracture after surgery. Instead, a comparative study needs to be conducted to address this issue. In this study, we observed natural healing of detached osteochondral fragment of the talus (Fig. 5). When conducting a precise comparative study in the future, the presence of chondral lesions should be verified via arthroscopy at the time of the initial ankle fracture surgery.
Fig. 5. Healed osteochondral lesion in the mid-lateral area of the talar dome.
In our study, a high incidence of osteochondral lesions was found, although there was no statistical significance. Most ankle injuries were accompanied by adduction, abduction, and rotation of talus with weight-bearing. It has been reported that impingement of talus on adjacent structures can easily cause chondral lesions and even lead to degenerative arthritic disorder.10,11)
Intra-articular fibrosis is caused by trauma or healing process after ankle fracture surgery. It is one of the major causes of ankle joint dysfunction.2) Utsugi et al.3) have classified fibrosis into B0 stage (no fibrosis), B1 stage (mild fibrosis without evidence of impingement), and B2 stage (diffuse fibrosis with impingement). In fact, articular impingement caused by extensive fibrosis of ankle joint can lead to continuous pain after initial ankle fracture.12,13,14) Therefore, extensive fibrosis might have caused intra-articular impingement that caused pain and limitation to the range of motion, rather than stage B1 or B2 of intra-articular fibrosis presented by Utsugi et al.3) There was significant (p = 0.02) difference between symptoms while walking and meniscus-line or cord-like fibrosis in our study patients. Therefore, it seems necessary to have an additional classification of intra-articular fibrosis according the shape of fibrosis formation. In addition, of the 21 patients with meniscus-like or cord-like fibrosis, 16 were found to have fibrosis in the anterolateral aspect of the tibiotalar joint. Therefore, this area was carefully examined when performing the exploratory arthroscopic surgery.
Ankle impingement is defined as entrapment of an anatomic structure that leads to pain and decreased range of motion of the ankle. It can be classified as soft tissue impingement or bony impingement. Soft tissue impingement usually results from scarring and fibrosis associated with synovial, capsular, or ligamentous injury. Soft tissue impingement most often occurs in the anterolateral gutter, the medial ankle, or the region of syndesmosis. Bony impingement can result from spur formation along the anterior margin of the distal tibia and talus or as a result of a prominent posterolateral talar process (the os trigonum).15)
In intra-articular fibrosis, most cases of fibrosis are found to be located on the anterior aspect of the ankle joint. An almost negligible incidence of fibrosis has been reported on the posterior side. In our study, no articular fibrosis was observed on the posterior aspect of the ankle. There are several reasons to explain why intra-articular fibrosis progresses more easily on the anterior side than on the posterior side. First, the anterior side is narrower than the posterior side in the ankle joint. Second, pressure is concentrated more on the anterior side than on the posterior side during weight-bearing, leading to increased stress and damage to the anterior side. Third, the plantar flexion of the ankle has generally greater range of motion than the dorsiflexion of the ankle.
The arthroscopic findings regarding the ankle fractures lead to the conclusion that ankle fractures are predominantly supination-external rotation type and pronation-external rotation type. There was no significant difference between the two types.
Synovitis and anterior bony impingement syndrome was not significantly associated with patient-reported symptoms. The incidence of such lesions was considered as a result of influence of various factors over a long period of time during the healing process.
In general, magnetic resonance imaging (MRI) is preferred over CT for the assessment of intra-articular lesion including talar dome chondral and osteochondral lesions. However, CT and bone scan may be also helpful in the detection and characterization of intra-articular lesions in the ankle to demonstrate their position and extent, including the status of the chondral surface, demonstrating any associated chondral delamination, assessing the integrity of the subchondral plate, and assessing cancellous subchondral bone for bone marrow edema like signal, sclerosis, cystic change, or the presence of an unstable osteochondral fragment.16) Taking cost and effectiveness into consideration, we could not use bone scan and MRI routinely in all ankle fracture patients. This is one of the critical limitation of our study. To identify preoperative articular lesion, we need to use intraoperative arthroscopic exam at time of ankle fracture surgery in the future.
Ambiguous symptoms observed in the ankle are primarily caused by soft-tissue damage. It is difficult to identify such damage via simple radiography.17) MRI is typically performed. However, limitations still exist, such as the interference of internal fixation devices and cost-effectiveness perspective.2) Therefore, arthroscopy has been increasingly used recently. Arthroscopy can be performed to diagnose and treat continuous pain resulting from ankle injuries. Many studies have reported that it can identify more lesions than radiological evaluations in ankle joint.2,18,19)
In order to improve the postoperative outcomes of ankle fracture patients, exploratory arthroscopic surgery should be used in conjunction with initial ankle fracture surgery by removing hemorrhage and injured tissues in the intra-articular region in addition to radiological evaluation. It will also facilitate the identification of intra-articular lesions and decrease articular fibrosis. In addition, arthroscopy will be very useful for the evaluation and treatment of symptoms even after a long postoperative evaluation period in ankle fracture surgery. However, severe edema, capsular rupture, and open fracture due to extensive damage will require caution when performing the exploratory arthroscopic surgery.
In conclusion, overlooked intra-articular lesion after ankle fracture surgery is one of the main factors that impede favorable surgical outcome. Arthroscopic surgery is a useful method that can be used to simultaneously evaluate and treat ankle symptoms. Intraoperative arthroscopic examination and treatment for identified intra-articular lesions should be undertaken simultaneously to improve the outcome for symptomatic patients who have undergone surgery for ankle fracture.
Footnotes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Jaivin JS, Ferkel RD. Arthroscopy of the foot and ankle. Clin Sports Med. 1994;13(4):761–783. [PubMed] [Google Scholar]
- 2.Thomas B, Yeo JM, Slater GL. Chronic pain after ankle fracture: an arthroscopic assessment case series. Foot Ankle Int. 2005;26(12):1012–1016. doi: 10.1177/107110070502601202. [DOI] [PubMed] [Google Scholar]
- 3.Utsugi K, Sakai H, Hiraoka H, Yashiki M, Mogi H. Intra-articular fibrous tissue formation following ankle fracture: the significance of arthroscopic debridement of fibrous tissue. Arthroscopy. 2007;23(1):89–93. doi: 10.1016/j.arthro.2006.07.055. [DOI] [PubMed] [Google Scholar]
- 4.Beris AE, Kabbani KT, Xenakis TA, Mitsionis G, Soucacos PK, Soucacos PN. Surgical treatment of malleolar fractures: a review of 144 patients. Clin Orthop Relat Res. 1997;(341):90–98. [PubMed] [Google Scholar]
- 5.Day GA, Swanson CE, Hulcombe BG. Operative treatment of ankle fractures: a minimum ten-year follow-up. Foot Ankle Int. 2001;22(2):102–106. doi: 10.1177/107110070102200204. [DOI] [PubMed] [Google Scholar]
- 6.Berndt AL, Harty M. Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am. 1959;41(6):988–1020. [PubMed] [Google Scholar]
- 7.Ferkel RD, Scranton PE., Jr Arthroscopy of the ankle and foot. J Bone Joint Surg Am. 1993;75(8):1233–1242. doi: 10.2106/00004623-199308000-00016. [DOI] [PubMed] [Google Scholar]
- 8.Hintermann B, Regazzoni P, Lampert C, Stutz G, Gachter A. Arhroscopic findings in acute fractures of the ankle. J Bone Joint Surg Br. 2000;82(3):345–351. doi: 10.1302/0301-620x.82b3.10064. [DOI] [PubMed] [Google Scholar]
- 9.Takao M, Uchio Y, Naito K, Fukazawa I, Kakimaru T, Ochi M. Diagnosis and treatment of combined intra-articular disorders in acute distal fibular fractures. J Trauma. 2004;57(6):1303–1307. doi: 10.1097/01.ta.0000114062.42369.88. [DOI] [PubMed] [Google Scholar]
- 10.Bonnin M, Bouysset M. Arthroscopy of the ankle: analysis of results and indications on a series of 75 cases. Foot Ankle Int. 1999;20(11):744–751. doi: 10.1177/107110079902001113. [DOI] [PubMed] [Google Scholar]
- 11.van Dijk CN, Bossuyt PM, Marti RK. Medial ankle pain after lateral ligament rupture. J Bone Joint Surg Br. 1996;78(4):562–567. [PubMed] [Google Scholar]
- 12.Gulish HA, Sullivan RJ, Aronow M. Arthroscopic treatment of soft-tissue impingement lesions of the ankle in adolescents. Foot Ankle Int. 2005;26(3):204–207. doi: 10.1177/107110070502600304. [DOI] [PubMed] [Google Scholar]
- 13.Henderson I, La Valette D. Ankle impingement: combined anterior and posterior impingement syndrome of the ankle. Foot Ankle Int. 2004;25(9):632–638. doi: 10.1177/107110070402500907. [DOI] [PubMed] [Google Scholar]
- 14.Lee JW, Suh JS, Huh YM, Moon ES, Kim SJ. Soft tissue impingement syndrome of the ankle: diagnostic efficacy of MRI and clinical results after arthroscopic treatment. Foot Ankle Int. 2004;25(12):896–902. doi: 10.1177/107110070402501209. [DOI] [PubMed] [Google Scholar]
- 15.Russo A, Zappia M, Reginelli A, et al. Ankle impingement: a review of multimodality imaging approach. Musculoskelet Surg. 2013;97(Suppl 2):S161–S168. doi: 10.1007/s12306-013-0286-8. [DOI] [PubMed] [Google Scholar]
- 16.Linklater JM. Imaging of talar dome chondral and osteochondral lesions. Top Magn Reson Imaging. 2010;21(1):3–13. doi: 10.1097/RMR.0b013e31820ef1c2. [DOI] [PubMed] [Google Scholar]
- 17.Loren GJ, Ferkel RD. Arthroscopic assessment of occult intra-articular injury in acute ankle fractures. Arthroscopy. 2002;18(4):412–421. doi: 10.1053/jars.2002.32317. [DOI] [PubMed] [Google Scholar]
- 18.Martin DF, Baker CL, Curl WW, Andrews JR, Robie DB, Haas AF. Operative ankle arthroscopy: long-term followup. Am J Sports Med. 1989;17(1):16–23. doi: 10.1177/036354658901700103. [DOI] [PubMed] [Google Scholar]
- 19.Ogilvie-Harris DJ, Gilbart MK, Chorney K. Chronic pain following ankle sprains in athletes: the role of arthroscopic surgery. Arthroscopy. 1997;13(5):564–574. doi: 10.1016/s0749-8063(97)90181-x. [DOI] [PubMed] [Google Scholar]