

Abstract
Diffuse normolipemic plane xanthoma (DNPX) was first described by Altman and Winkelmann in 1962. It is a rare and non-inherited form of xanthomatosis. Clinically, the dermatosis is characterized by the presence of symmetric yellowish-orange plaques that favor the neck, upper trunk, flexural folds and periorbital region. It has been recognized to be associated with hematological diseases, especially with multiple myeloma and monoclonal gammopathy. We present a patient with diffuse plane xanthoma, normal lipid level, and monoclonal gammopathy.
Keywords: xanthoma, plane xanthoma, diffuse normolipemic plane xanthoma, multiple myeloma, lymphoproliferative disorder, monoclonal gammopathy, paraproteinemia
Case report
An 85-year-old man presented with an 8-month history of slowly increasing diffuse yellow skin lesions on the torso and upper arms. He had been unaware of the discoloration until his internist noted it and referred him to dermatology. The patient had been followed by a hematologist for paraproteinemia that had not been treated.
The examination showed well-demarcated yellow patches and plaques covering large portions of his upper trunk with some islands of sparing (Figure 1, 2). The dermoscopic evaluation showed a reticular pattern of yellow amorphous homogeneous structures with overlying branched and linear vessels (Figure 3). A skin biopsy showed scattered foamy histiocytes within the reticular dermis, which were consistent with a plane xanthoma (Figures 4, 5, 6). A complete blood count, comprehensive metabolic panel, fasting lipid panel were within normal range. The serum protein electrophoresis showed elevated IgG at 3780. There was an M-band present in the gamma region.
Figure 1.

Clinical view shows well-demarcated yellow patches and plaques covering large portions of the upper chest and shoulder with some islands of sparing. [Copyright: ©2015 Cohen et al.]
Figure 2.

Well-demarcated yellow plaques on the upper back. [Copyright: ©2015 Cohen et al.]
Figure 3.

Dermoscopic view shows a reticular pattern of yellow amorphous uniformed granules with overlying vascular structures. [Copyright: ©2015 Cohen et al.]
Figures. 4, 5, 6.
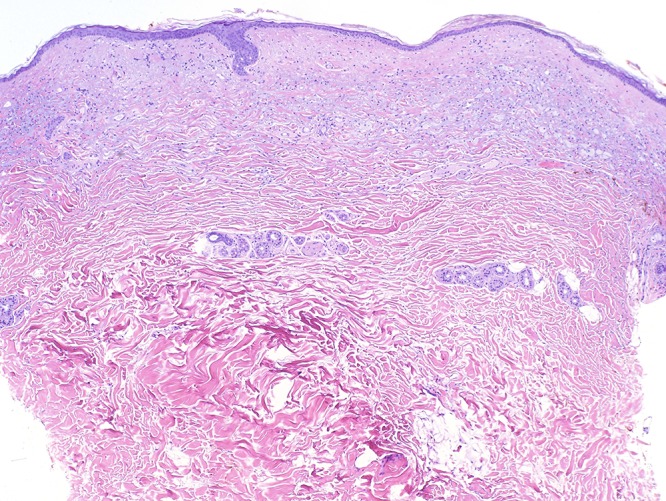
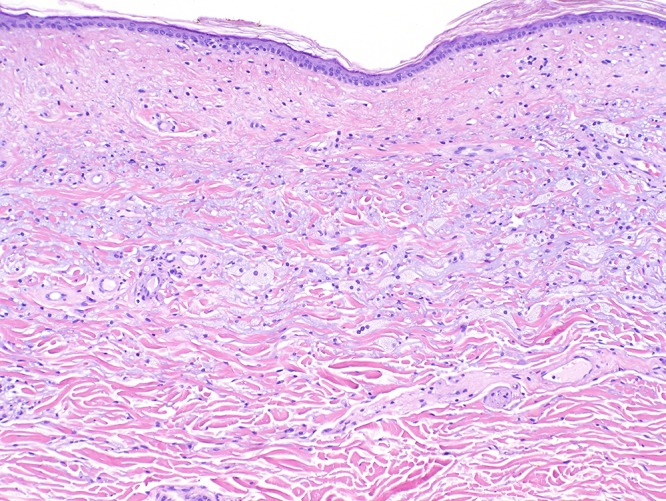
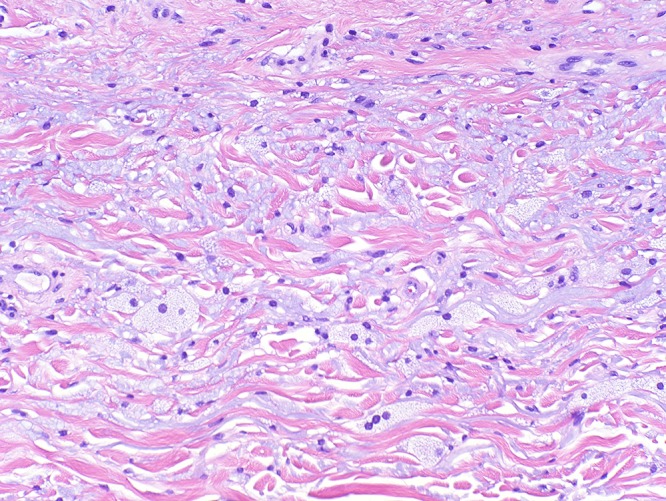
Histology views show scattered foamy histiocytes within the papillary dermis with a normal overlying epidermis, which were consistent with a plane xanthoma. [Copyright: ©2015 Cohen et al.]
Discussion
Diffuse normolipemic plane xanthoma (DNPX) was first described by Altman and Winkelmann in 1962 [1]. It is an uncommon subtype of non-Langerhans histiocytosis [15]. DNPX is characterized by xanthelasma palpebrarum; diffuse plane xanthoma of the head, neck, trunk, and extremities; and normal plasma lipid levels [2,4]. Xanthelasma typically appears first, followed by involvement of the lateral parts of the neck and upper trunk [1]. Clinically, the dermatosis is characterized by the presence of symmetric yellowish-orange plaques that favor the neck, upper trunk, flexural folds and periorbital region [1,2]. Histologically, foam cells (macrophages that have engulfed lipid droplets) and variable numbers of Touton giant cells, lymphocytes, and foamy histiocytes can be seen [3].
While not all cutaneous xanthomas are associated with systemic diseases, DNPX has been associated with systemic diseases, particularly multiple myeloma and monoclonal gammopathy [2,3]. However, other malignant hematological or lymphoproliferative disorders associated with DNPX include acute monoblastic leukemia, chronic myelomonocytic leukemia, chronic myloid leukemia, chronic lymphatic leukemia, non-Hodgkin’s lymphoma, adult T-cell lymphoma/leukemia, Sezary syndrome, Waldenstrom’s macroglobulinemia, cryoglobulineimia and Castleman’s disease [2,3,5–12].
The pathogenesis of DNPX has not been fully elucidated, however, in gammopathy-associated DNPX, monoclonal IgG is thought to bind to circulating LDL, rendering the antibody– LDL complex more susceptible to phagocytosis by macrophages [13]. DNPX can precede such disorders by several years; therefore close follow-up with periodic laboratory tests for myeloproliferative disorders should be performed [4].
There are currently several treatment options available. In patients with limited involvement, the individual lesions can be excised. Other options include chemabrasion, derm-abrasion, and ablative laser therapy. The erbium:YAG laser has been used successfully to treat facial xanthomas in one patient [14].
In this patient, currently there are no associated systemic symptoms. His hematologist was informed of the diagnosis. The patient will be evaluated for potential underlying malignancies. Moreover, this case shows that dermatological lesions can be the first manifestation of important hematological diseases and so physicians should be familiarized with this rare entity.
Footnotes
Funding: None.
Competing interests: The authors have no conflicts of interest to disclose.
All authors have contributed significantly to this publication.
References
- 1.Altman J, Winkelmann RK. Diffuse normolipemic plane xanthoma. Arch Dermatol. 1962;85:633–40. doi: 10.1001/archderm.1962.01590050063012. [DOI] [PubMed] [Google Scholar]
- 2.Lynch PJ, Winkelmann RK. Generalized plane xanthoma and systemic disease. Arch Dermatol. 1966;93:639–46. [PubMed] [Google Scholar]
- 3.Marcoval J, Moreno A, Bordas X, et al. Diffuse plane xanthoma: clinicopathologic study of 8 cases. J Am Acad Dermatol. 1998;39:439–42. doi: 10.1016/s0190-9622(98)70321-4. [DOI] [PubMed] [Google Scholar]
- 4.Loo DS, Kang S. Diffuse normolipidemic plane xanthomas with monoclonal gammopathy presenting as urticarial plaques. J Am Acad Dermatol. 1996;35:829–32. doi: 10.1016/s0190-9622(96)90095-x. [DOI] [PubMed] [Google Scholar]
- 5.Hu CH, Winkelmann RK. Unusual normolipemic cutaneous xanthomatosis: a comparison of two cases illustrating the differential diagnosis. Acta Dermato-Venereol. 1977;57:421–9. [PubMed] [Google Scholar]
- 6.Groszek E, Abrams JJ, Grundy SM. Normolipidemic planar xanthomatosis associated with benign monoclonal gammopathy. Metabolism. 1981;30:927–35. doi: 10.1016/0026-0495(81)90073-1. [DOI] [PubMed] [Google Scholar]
- 7.Jones RR, Baughan ASJ, Cream JJ, et al. Complement abnormalities in diffuse plane xanthomatosis with paraproteinmia. Br J Dermatol. 1979;101:711–6. doi: 10.1111/j.1365-2133.1979.tb05652.x. [DOI] [PubMed] [Google Scholar]
- 8.Jordon RE, McDuffie FC, Good RA, et al. Diffuse normolipidemic plane xanthomatosis: an abnormal complement component profile. Clin Exp Immunol. 1974;18:407–15. [PMC free article] [PubMed] [Google Scholar]
- 9.Kodama H, Nakagawa S, Tanioku K. Plane xanthomatosis with antilipoprotein autoantibody. Arch Dermatol. 1972;105:722–7. [PubMed] [Google Scholar]
- 10.Wilson DE, Flowers CM, Hershgold EJ, et al. Multiple myeloma, cryoglobulinemia and xanthomatosis: distinct clinical and biochemical syndromes in two patients. Am J Med. 1975;59:721–9. doi: 10.1016/0002-9343(75)90233-8. [DOI] [PubMed] [Google Scholar]
- 11.Waldorf HA, Duncan LM, Fitzpatrick TB. Circumscribed areas of yellow pigmentation on the arms of a 67 year old man. Fitzpatrick’s J Clinic Dermatol. 1994;2:27–9. [Google Scholar]
- 12.Kim KJ, LEE DP, Suh HS, et al. Diffuse plane xanthomas in a patient with chronic myeloid leukemia. J Dermatol. 2004;31:503–5. doi: 10.1111/j.1346-8138.2004.tb00543.x. [DOI] [PubMed] [Google Scholar]
- 13.Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology. 3rd ed. New York: Saunders; 2012. [Google Scholar]
- 14.Lorenz S, Hohenleutner S, Hohenleutner U, et al. Treatment of diffuse plane xanthoma of the face with the Erbium: Yag Laser. Arch Dermatol. 2001;137:1413–5. doi: 10.1001/archderm.137.11.1413. [DOI] [PubMed] [Google Scholar]
- 15.Burgesser MV, Calafat P, Diller A. Diffuse plane xanthomatosis associated with haematologic disorder and solid tumor. Findings of an autopsy. Rev Fac Cien Med Univ Nac Cordoba. 2011;68:65–9. [PubMed] [Google Scholar]