

Abstract
Some anterior chambers do not readily shallow because of insufficient posterior pressure and/or very deep anterior chamber anatomy, which can make unscrolling descemet membrane endothelial keratoplasty (DMEK) tissue more challenging with an unmodified tap technique. We present a hands-free method for augmenting posterior pressure by temporarily tucking cellulose sponges under the blades of the eyelid speculum. The sponges transfer some of the eyelid speculum’s weight onto the bulbar surface posterior to the iris, thereby indenting the sclera and causing the iris diaphragm to bulge further forward. This hands-free technique can transform a potentially challenging DMEK case into a more straightforward one by facilitating both a shallow anterior chamber and a bimanual unscrolling technique. However, it only works in bicameral eyes with a vitreous body (e.g., an eye with penetrating keratoplasty, vitreous syneresis, and axial myopia) and will not work in unicameral eyes after vitrectomy (e.g., an eye with an Anterior Chamber Intraocular Lens (ACIOL)).
Keywords: Cellulose sponge, chamber depth, DMEK, posterior pressure, tap technique
Descemet membrane endothelial keratoplasty (DMEK) is rapidly becoming the procedure of choice among corneal transplant surgeons.[1] Alternative surgical techniques have emerged,[2,3,4] but a chamber-shallowing, endothelium-out, no-touch tapping technique, first described by Yoeruek in 2013,[5] and subsequently popularized by others[6] remains the most popular surgical approach for routine cases.[7]
A prerequisite to successful execution of the no-touch tapping technique is an optimally shallow anterior chamber. A shallow anterior chamber prevents recoil of the tissue into a scroll as fluid currents induced by tapping the corneal surface unfurl the tissue. In an optimally shallow chamber, the iris plane bulges anteriorly towards the cornea due to posterior pressure, which in turn renders the anterior surface of the DMEK scroll immediately subjacent to and in partial contact with the overlying posterior surface of the cornea; the DMEK scroll’s posterior surface sits on the iris plane. The iris and overlying cornea’s mechanism of action for preventing re-scrolling of the DMEK tissue is by exerting frictional forces that counteract the tissue’s intrinsic recoil forces. Tapping the cornea in the setting of an optimally shallow anterior chamber results in a DMEK scroll progressively unfurling without re-scrolling. In a chamber that is too shallow or nearly absent, there is excessive contact between the iris, DMEK scroll, and overlying cornea such that the frictional forces exerted on the scroll pin the leaflets into a stationary position. Tapping the cornea in the setting of a flat anterior chamber does not result in any movement of the scroll’s leaflets. By contrast, in a chamber that is too deep, there is insufficient contact between the iris, DMEK scroll, and overlying cornea such that the recoil forces of the scroll are unopposed. Tapping the cornea in the setting of a deep anterior chamber results in unfurling movements of the scroll that are immediately followed by recoiling movements, resulting in a DMEK tissue that begins to open but does not remain open. Titrating the anterior chamber to the optimal shallowness – and avoiding a flat or deep anterior chamber – rests with the surgeon’s judgment and continual attention as he adds and removes fluid during the unscrolling process.
However, the propensity of an anterior chamber to shallow sufficiently will always hinge on the eye’s posterior pressure or lack thereof. In the presence of some comorbidities, chamber shallowing can be difficult, if not impossible. For example, eyes that are post-vitrectomy lack the posterior pressure necessary to achieve sufficient and durable chamber shallowing.[8] However, even eyes with intact vitreous bodies can be difficult to shallow in certain conditions, such as axial myopia, vitreous syneresis, penetrating keratoplasty, and glaucoma shunts. In such circumstances, experienced surgeons have described how to augment the eye’s posterior pressure by indenting the bulbar surface with a finger or surgical instrument.[5] But because one hand is tasked with executing two movements at once, this approach requires an assistant or modification of one’s preferred two-cannula technique (such as the highly effective Dirisamer technique).
We describe a hands-free method for augmenting posterior pressure, when needed, by placing self-retained cellulose sponges between the bulbar surface and the eyelid speculum.
Technique
Before injecting the DMEK allograft into the eye, the surgeon tests the anterior chamber’s propensity to shallow by releasing fluid from an incision. If the iris readily bulges anteriorly and the cornea remains convex, the surgeon re-inflates the chamber and proceeds with his standard DMEK technique (i.e., tissue injection, bimanual tapping, etc.). An iris that does not bulge anteriorly enough and/or a cornea that becomes creased or concave in shape [Fig. 1] are intraoperative signs of insufficient posterior pressure. In the presence of these signs, the surgeon re-inflates the anterior chamber to normal pressure (to reduce the duration of hypotony) and executes our hands-free method for augmenting posterior pressure.
Figure 1.
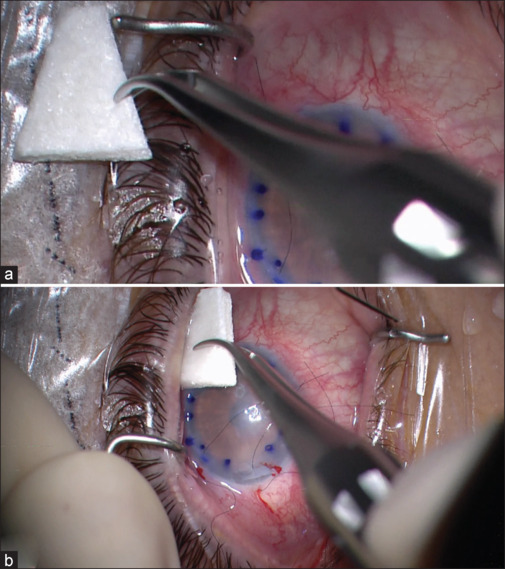
(a) Tips of the cellulose sponge spears are cut off. (b) Cellulose sponges are inserted between the bulbar conjunctiva and the eyelid speculum
The surgeon or his assistant cuts (nearly) the entire triangle-shaped cellulose tip from the plastic shaft of a standard microsurgical spear when it is still dry; this step is repeated for two to four sponges. To augment posterior pressure, a single (dry) cellulose sponge is wedged under the superior speculum blade, and another is wedged under the inferior speculum blade using forceps [Fig. 1]. If the sponges do not spontaneously hydrate, the surgeon hydrates them with balanced salt solution (BSS) to increase their size. The sponges, which are now wedged between the globe and speculum blades, transmit some of the eyelid speculum’s weight onto the bulbar surface posterior to the iris. The speculum-sponge complex, in turn, indents the sclera and augments posterior pressure. The anterior chamber is tested again by burping one of the incisions [Fig. 2]. If the anterior chamber sufficiently shallows, the surgeon reforms the chamber again and proceeds with his standard DMEK technique. If it does not appropriately shallow, an additional sponge or sponges may be placed in a similar fashion.
Figure 2.
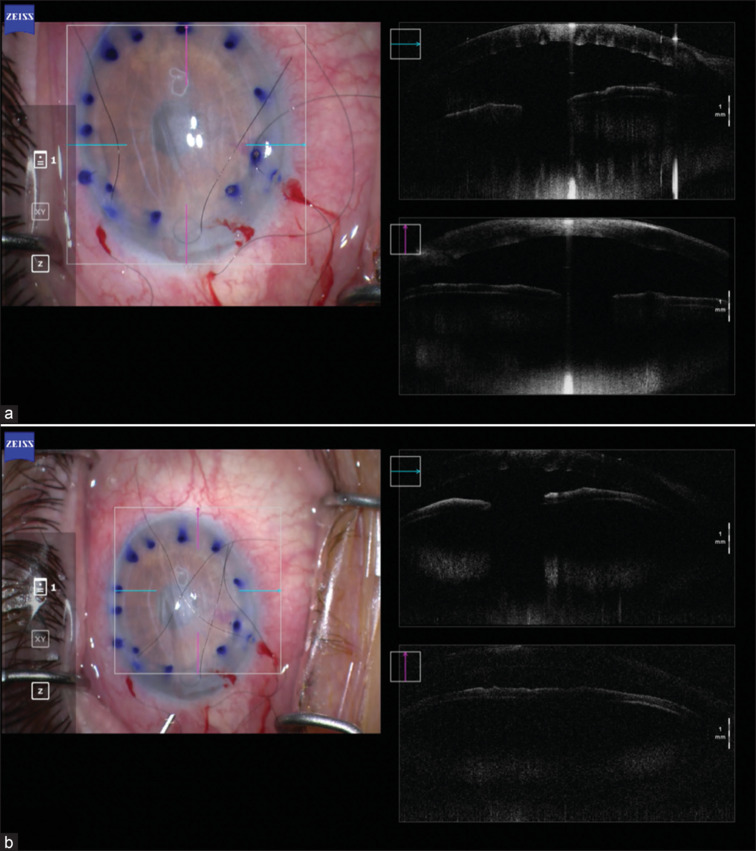
Intraoperative anterior segment optical coherence tomography demonstrating (a) difficult to shallow chamber before cellulose sponge insertion, and (b) easy to shallow chamber after cellulose sponge insertion
After tissue unscrolling and centering using a bimanual two-cannula technique, a small air or gas bubble is placed to secure the graft and the eye is titrated to a normal intraocular pressure. Following this step, the sponges are carefully removed one at a time, taking care to observe the anterior chamber volume fluctuations that result. After removal of the sponges, final bubble titration can then be completed as usual [Video 1].
Discussion
We present a simple, effective technique that employs the absorbent, expansile properties of cellulose sponges to transmit some of the weight of an eyelid speculum onto the ocular surface and thereby exert an indenting force on the globe to augment posterior pressure in challenging DMEK cases. Approximately half of the Principal Investigator’s (PI’s) DMEK cases are performed with an endothelium-out tap-technique (the other half are performed with an endothelium-in pull-through technique). The PI tests the anterior chamber’s propensity to shallow in every tap-technique case before tissue injection. In approximately one-half of tap-technique cases, or about 25% of all of the PI’s DMEK cases, the eye benefits from augmentation of the posterior pressure with self-retained cellulose sponges to optimize the anterior chamber depth. This includes many eyes with trabeculectomies and tube shunts. Surgeons who perform DMEK exclusively with an endothelium-out tap-technique may find our cellulose sponge technique to benefit their cases more frequently.
At our institution, an “open” style Lieberman speculum is employed, but surgeons utilizing “closed” style bladed speculums should experience similar results. Although in our experience no more than four sponges have been required, we recommend caution in exceeding this number given the theoretical risk of chorioretinal trauma induced by significant bulbar distortion. Our practice is to restore normal intraocular pressure before placing the sponges to minimize the duration of hyptony and mitigate the risk of spontaneous fibrin formation, which can have deleterious effects on DMEK unscrolling. However, some surgeons may find it more efficient to skip this step by placing the sponges to the desired effect while the eye is hypotonous, reforming the chamber, and injecting the tissue.
The strengths of this technique are that it is easy to execute, utilizes materials that are ubiquitous in every operating theater, and does not require advanced planning. The utility of the technique stems from it being hands-free, which enables the surgeon to use his usual bimanual maneuvers to unfurl a DMEK scroll in eyes that may otherwise present challenges to unscrolling.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video available on: https://journals.lww.com/ijo
References
- 1.EBAA . Washington, D.C: Eye Bank Association of America; 2023. 2022 Eye Banking Statistical Report. [Google Scholar]
- 2.Price MO, Lisek M, Kelley M, Feng MT, Price FW., Jr Endothelium-in versus endothelium-out insertion with descemet membrane endothelial keratoplasty. Cornea. 2018;37:1098–101. doi: 10.1097/ICO.0000000000001650. [DOI] [PubMed] [Google Scholar]
- 3.Tan TE, Devarajan K, Seah XY, Lin SJ, Peh GSL, Cajucom-Uy HY, et al. Descemet membrane endothelial keratoplasty with a pull-through insertion device: Surgical technique, endothelial cell loss, and early clinical results. Cornea. 2020;39:558–65. doi: 10.1097/ICO.0000000000002268. [DOI] [PubMed] [Google Scholar]
- 4.Yu AC, Myerscough J, Spena R, Fusco F, Socea S, Furiosi L, et al. Three-year outcomes of tri-folded endothelium-in descemet membrane endothelial keratoplasty with pull-through technique. Am J Ophthalmol. 2020;219:121–31. doi: 10.1016/j.ajo.2020.07.004. [DOI] [PubMed] [Google Scholar]
- 5.Yoeruek E, Bayyoud T, Hofmann J, Bartz-Schmidt KU. Novel maneuver facilitating descemet membrane unfolding in the anterior chamber. Cornea. 2013;32:370–3. doi: 10.1097/ICO.0b013e318254fa06. [DOI] [PubMed] [Google Scholar]
- 6.Terry MA, Straiko MD, Veldman PB, Talajic JC, VanZyl C, Sales CS, et al. Standardized DMEK technique: Reducing complications using prestripped tissue, novel glass injector, and sulfur hexafluoride (SF6) gas. Cornea. 2015;34:845–52. doi: 10.1097/ICO.0000000000000479. [DOI] [PubMed] [Google Scholar]
- 7.Varadaraj V, Woreta FA, Stoeger CG, Tran KD, Jorgenson R, Srikumaran D. Surgeon preference for endothelial keratoplasty techniques. Cornea. 2020;39:2–7. doi: 10.1097/ICO.0000000000002118. [DOI] [PubMed] [Google Scholar]
- 8.Mednick Z, Sorkin N, Einan-Lifshitz A, Santaella G, Trinh T, Chan CC, Rootman DS. Long-term outcomes of descemet membrane endothelial keratoplasty in postvitrectomized eyes with the use of pars plana infusion. Cornea. 2020;39:457–60. doi: 10.1097/ICO.0000000000002228. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.