

Abstract
Context:
India is the second largest consumer of tobacco. Tobacco consumption in nonsmoking forms is culturally accepted even among women.
Aims:
This study aimed at understanding the patterns and predictors of smokeless tobacco (SLT) use among the urban low-socioeconomic women in Mumbai, India.
Materials and Methods:
This is a cross-sectional community-based survey of tobacco usage among women residing in seven low-socioeconomic communities in suburbs of Mumbai, India. Staff for the study was recruited, trained, clusters selected, accurately mapped, households identified, meetings held with community leaders, and household surveys conducted. Women using tobacco were invited to participate in the detailed survey and interviewed to document the various sociodemographic factors and in depth information on tobacco use. The data were computerized and analyzed.
Results:
About 22.30% of the total female population consumed tobacco, mainly in the smokeless forms, with only 0.50% of the tobacco users using smoked tobacco. Masheri was the most common form of tobacco used, followed by chewing tobacco. The median frequency of use of different tobacco products varied from 2 to 4 per day. The mean age at initiation of tobacco was 26.23 years. According to the results of univariate and multivariate logistic regression analysis, illiterate women, with advancing age, belonging to Hindu, Muslim, or Buddhist communities, who were either manual laborers or housewives, divorced or separated, and speaking Marathi were at higher risk of being tobacco user.
Conclusion:
Patterns and predictors of SLT use among women have been identified in the present study. This will guide in planning prevention and control strategies.
Keywords: India, predictors, prevalence, smokeless tobacco, women
INTRODUCTION
Globally, nearly 6 million people die from tobacco-related causes every year. If the present pattern of tobacco use persists, it is then estimated that there could be one billion premature deaths globally during the 21st century.[1] Overall, 6.7% of women used smokeless tobacco (SLT) in the 16 Global Adult Tobacco Survey (GATS) countries surveyed.[2] The use of SLT, which was limited to South-East Asian countries in the past is rapidly increasing all over. According to the Bloomberg global SLT market report the increasing awareness about the health risks associated with smoking has led to the development of several SLT alternatives. The US market forecast for the period 2010-2012 for SLT was expected to increase at a compounded annual growth rate of about 7%.[3] In the US during 2004-2005, 3% of adults (6% of men and 0.4% of women) used SLT.[4] According to the European Commission report on health effects of SLT products 2008, 24% of Swedish men and 3% of Swedish women use snus daily. Furthermore, 5% of Norwegian men use snus.[5]
India is the second largest consumer of tobacco. All sections of Indian population consume tobacco though the prevalence of habit and the types predominantly used vary across different geographical areas.[6] In India, tobacco consumption, mainly in the nonsmoking and application forms, is culturally accepted even among women. Hence, smokeless forms of tobacco use by women are widely prevalent. According to the GATS survey conducted among population between 15 and 65 years of age, 35% of adults in India use tobacco. The tobacco consumption rate varies by gender and place of residence. It is estimated that there are 274.9 million tobacco users in India with 163.7 million only SLT users, 68.9 million only smokers, and 42.3 million users of both smoking and smokeless forms of tobacco. Higher rates of tobacco consumption of 38.4% are seen in the rural areas as compared to 25.3% in the urban areas. The use of SLT is more common among both men (24% smokeless, 15% smoking, and 9% both smoking and smokeless) and women (17% smokeless, 2% smoking, and 1% both smoking and smokeless) as compared to the smoking forms.[7] According to the National Family Health Survey-3 (NFHS-3), 57% of men in the age group 15-54 years and 11% of women in the age group 15-49 years, including 9% of pregnant women, use some form of tobacco.[8]
We conducted the present survey incorporated in a community-based cancer screening program to understand the prevalence of the different types of tobacco used by urban low-socioeconomic women in Maharashtra and identify the key sociodemographic factors associated with tobacco use.
MATERIALS AND METHODS
This is a cross-sectional survey of tobacco usage mainly among women residing in seven low-socioeconomic communities in suburbs of Mumbai, India. This survey is part of a screening program for common cancers among women.
Staff for the program, chiefly consisting of the medical social workers, primary health workers, porters, and the data management personnel were recruited and trained for the duration of 2 months to conduct the different project activities. The seven slum clusters were selected and accurately mapped to identify each and every house, lanes and by-lanes of the area along with important landmarks. Several meetings were held with the community leaders to explain the importance of the survey and garner their support for the same. Every house in the area was numbered and a household survey was initially conducted to identify the number of members in each household, gender distribution, age distribution, their tobacco use history, and a list of eligible women was generated. The criteria for eligibility was women tobacco users of any age (current user or past tobacco user — who have consumed tobacco for at least 3 consecutive years) residing in the selected clusters. The households of the eligible women were revisited, and a written informed consent in local language was obtained after explaining them the purpose and methodology of the program. For the illiterate women, the consent form was explained and left thumb impression was obtained in the presence of a witness from the local area and those who wished to participate. The participant women were then interviewed with a detailed questionnaire to document the various sociodemographic factors and in depth information on tobacco use habits. After this, the women were given information about the hazards of tobacco use.
The data were entered in MYSQL version 2.11.6 (Stata Corp LP a company, US). Data error check was done by cross tabulation and checks for data consistency were conducted in MYSQL and intercooled Stata 8.2 (Oracle corporation's procedural extension for SQL). Data were analyzed in Stata. The prevalence of tobacco use habits and the different forms of tobacco use was tabulated. The relation of various sociodemographic factors with tobacco use habits was analyzed with univariate and multivariate logistic regression analysis. This paper presents the findings of the same.
RESULTS
The survey of the seven community areas consisting of total population of 68,481, shows the prevalence of tobacco use of 21.77%, with 21.27% of the total male population and 22.30% of the total female population consuming tobacco. The prevalence of tobacco use varied from 15.30% to 25.19% among the male population and 13.44-25.81% among the female population in the seven clusters studied. Tobacco consumption was also reported among the minor population (<18 years), with 31 male minors (0.28% of all male minors) and 41 female minors (0.40% of all female minors) consuming tobacco.
The different forms of tobacco used by the participant women are shown in Figure 1. Masheri, that is, burnt tobacco powder used to clean teeth is the major form of tobacco used (68.69%) followed by chewing tobacco (20.30%). Only 31 women (0.50%) used smoking forms of tobacco. The minor females who consumed tobacco predominantly used it in the form of masheri.
Figure 1.

Tobacco consumption among participant women
The distribution of the different forms of tobacco used by the participant women in each of the seven community areas is shown in Figure 2. Masheri is the most common form of tobacco used in each cluster, though the prevalence among the tobacco users varied from 53.90% in cluster 1 to 95.43% in cluster 5, followed by tapkir/snuff in some clusters (0.57-38.53%) and chewing tobacco (5.33-26.24%) in others.
Figure 2.
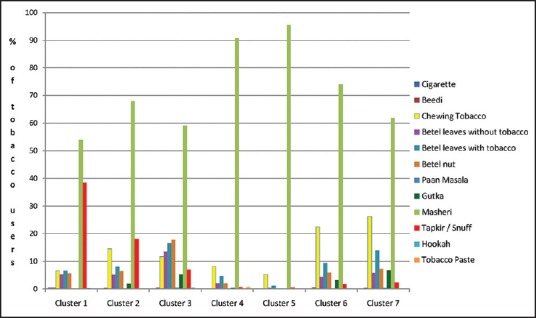
Distribution of various forms of tobacco consumed by participant women in each cluster
The median frequency and the range of daily use of different tobacco products by the participant women [Figure 3] are as follows, tobacco chewing (4, [1-20]); betel leaves with or without tobacco (3, ([1-36]); betel nuts (3, [1-15]); paan masala (3, [1-10]); gutkha (4, [1-33/60]); masheri (2, [1-30]); tapkir/snuff (3, [1-19]); tobacco paste (3, [1-5]); and smoking forms (4, [1-10]).
Figure 3.
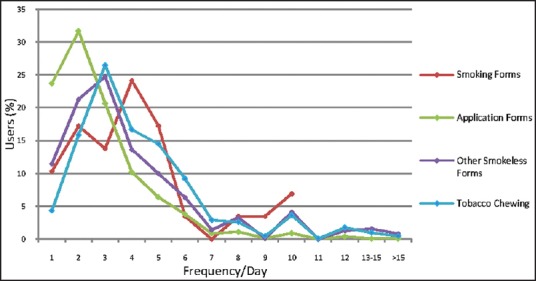
Frequency of use of various forms of tobacco
The mean age at initiation of tobacco use was 26.23 years among women in our study. The median age at initiation and the range for different tobacco products is as follows: Tobacco chewing: 29 years, (2-69); betel leaves with or without tobacco: 30 years, (3-77); betel nuts: 30 years, (3-77); paan masala: 32.5 years, (14-44); gutkha: 27 years, (4-68); masheri: 24 years, (2-69); tapkir/snuff: 20 years, (3-61); tobacco paste: 24 years, (20-33); and smoking forms: 35 years, (10-63) [Figure 4].
Figure 4.
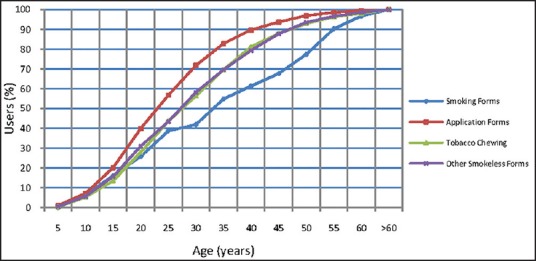
Cumulative distribution of age at initiation of various forms of tobacco
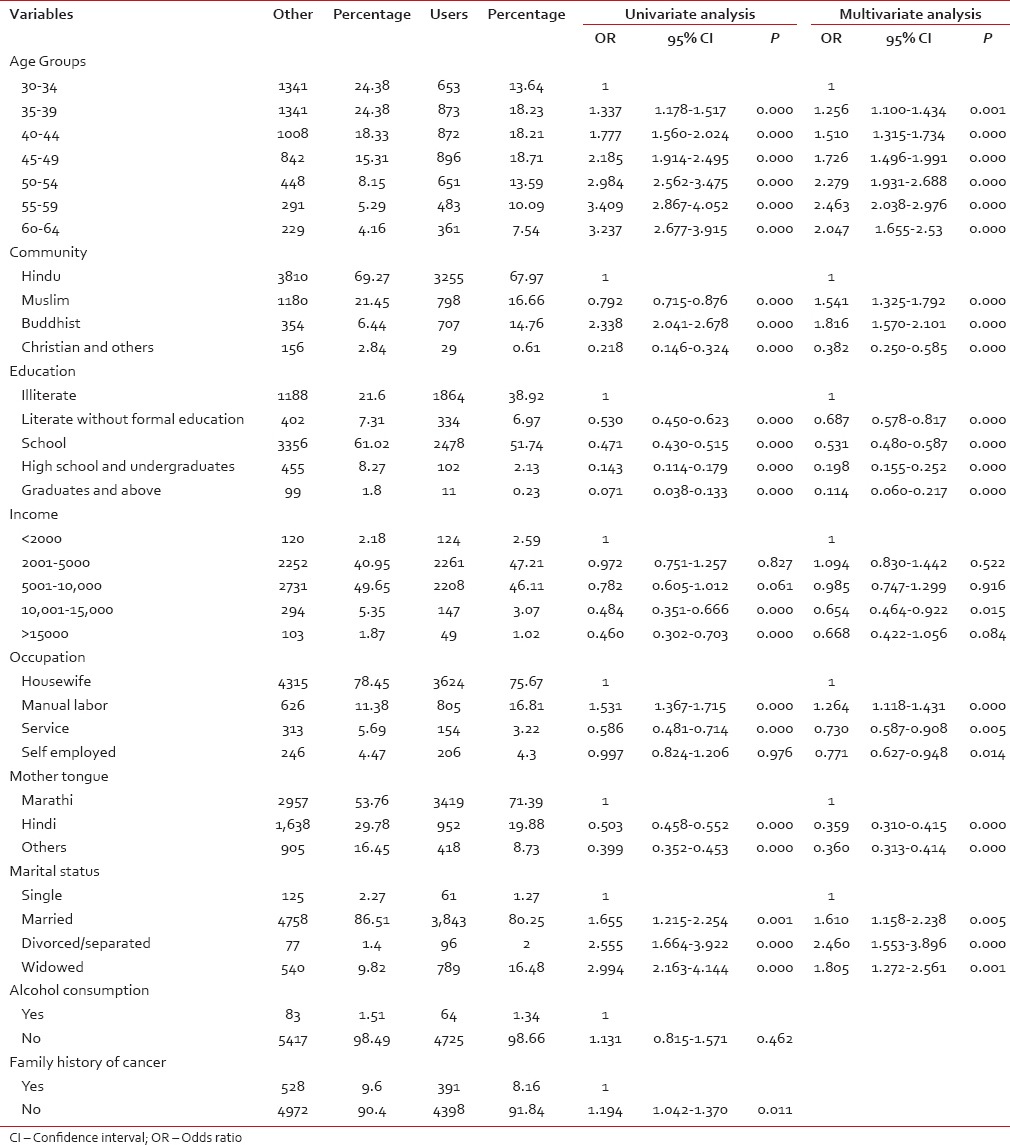
Univariate and multivariate logistic regression analysis were performed to identify the relation of various sociodemographic factors with the tobacco use habit among the participant women [Table 1]. According to the results of the multivariate logistic regression analysis age of women, community, education, occupation, mother tongue, and marital status were statistically significant. The illiterate, divorced, or separated women with advancing age, speaking Marathi, belonging to Hindu, Muslim, or Buddhist communities, who were either manual laborers or housewives were at higher risk of being a tobacco user as compared to other women.
Table 1.
Multivariate analysis showing relation of various socio-demographic variables with the tobacco consumption habit
DISCUSSION
The prevalence of tobacco consumption was similar among both men and women of the selected communities, with an average prevalence of 21.77% (all age groups included). The NFHS-3 survey reported the prevalence of tobacco use of 16.6% among women aged 15-49 years and 41.2% among men aged 15-54 years in Mumbai, India.[8] According to the GATS India survey, the prevalence of tobacco use, among individuals aged 15 years or older, was 48% among men and 20% among women. While the GATS survey in 14 low- and middle-income countries have noted tobacco use prevalence of 48·6% in men and 11·3% in women among individuals 15 years or older.[2] Tobacco consumption was also noted among children <14 years in the present survey, indicating that the habit is initiated early in life, and preventive action also needs to be incorporated from early years.
Among adults in the WHO South-East Asia region, the use of SLT was higher among males as compared to females in Bhutan, India, Myanmar, Nepal, and Sri Lanka while it's use was higher among females as compared to males in Bangladesh, Indonesia, and Thailand.[9] In Sri Lanka, 15.8% of population use SLT products and its use is three-fold higher among men as compared to women.[10] The prevalence of SLT use among women for overall India and for Maharashtra state was 18.4% and 18.9%, respectively.[7] In the present study, almost all women tobacco users used SLT products (99.50%) while only 31 women (0.50%) smoked tobacco. GATS, India survey reported the smoking prevalence of 3% among females aged 15 years or older, with most females smokers smoking daily.[7] Gupta in his survey in Mumbai during 1992-1994 reported smoking prevalence of only 0.4% among women aged 35 years or older.[11] According to the 1992 WHO report of women and tobacco, smoking by women is often socially unacceptable in many of the developing countries, and hence, women often use tobacco chewing as the alternate, more acceptable form.[12] According to the demographic and health survey conducted in nine South and Southeast Asian countries, smoking prevalence was much lower in women than men.[13]
According to the GATS, India estimates there are 206 million adults using various SLT products, among which 18.9 million women chew betel quid with tobacco, 18.2 million chew khaini, 11.1 million use gutkha, 24.1 million use tobacco for oral application, and another 20.7 million use some other SLT products.[7] In the present study, the prevalence of masheri use was 12.9%, chewing tobacco was 3.81%, betel leaves with or without tobacco was 2.94%, and tapkir/snuff was 0.99% among the total female population. Masheri, application of burned tobacco to clean the teeth, was the most common form of tobacco used by women in the present survey. This form of tobacco use is typically more common in the state of Maharashtra. Hence, in the present survey, many children too were found to be using masheri. Earlier survey in Mumbai had also reported masheri as the most dominant form of tobacco use among women.[11] A survey among pregnant women in rural Maharashtra found 30.9% using masheri during pregnancy.[14] Chewing tobacco and use of tapkir/snuff were the other commonly used forms of SLT in most of the areas surveyed in the present study. Betel quid chewing is a common habit among both men and women in Bangladesh, India, Pakistan, and Sri Lanka.[15] The demographic and health survey reported the use of chewing tobacco common in India, Nepal, Bangladesh, Maldives, and Cambodia.[13] Betel quid with tobacco is the traditional form of tobacco use in Sri Lanka.[10]
The prevalence of tobacco use habit varied from 15% to 25% in the seven clusters among the men and 13-26% among women of all age groups. In 1992-1994, the prevalence of tobacco use among men and women, 35 years and older, was 69.3% and 57.5%, respectively, in Mumbai. Women are almost solely used smokeless forms of tobacco.[11] Masheri was the most common form of tobacco used in each of the clusters in the present study, with the prevalence varying from 54% to 95% among the tobacco users in different clusters.
The median frequency of use of the different tobacco products varied between 2 and 4 times/day. An earlier survey in Mumbai had also reported most men and women using SLT products 2-5 times in a day, with the frequency of use being slightly more among men as compared to women.[11] The same survey had reported 90% women using mishri <3 times in a day.[11] In the present survey, wherein 69% of tobacco users used mishri, the median frequency of use was twice a day.
The median age at initiation varied between 20 and 30 years for different SLT products in the present study. In the GATS, India survey, the mean age of initiation among women, for tobacco (all forms) was 17.8 years and 18.5 years and for SLT was 17.1 years and 21 years, for overall India and Maharashtra, respectively.[7] Though the mean age at initiation of tobacco use was 26.23 years among women in the present study, there were also several minor girls who used tobacco, mainly in the form of masheri. The median age at initiation of masheri was 24 years in our study. Gupta reported that more than 50% of masheri users had initiated the habit before 10 years of age.[11] In the present survey, the median age at initiation of betel quid chewing and smoking was 30 years and 35 years, respectively. Whereas an earlier survey among men and women in Mumbai found the median age at initiation of betel quid chewing and smoking to be 20 years.[11]
According to results of univariate and multivariate logistic regression analysis age of women, community, education, occupation, mother tongue, and marital status were significantly associated with tobacco use. Tobacco use was associated with advancing age among women in our study. The same has also been reported in GATS India report[7] study from Chennai in India,[16] a study among Lumbee Indian women in North Carolina,[17] demographic and health surveys from nine South and Southeast Asian countries,[13] and three studies from Bangladesh.[18,19,20] Tobacco consumption was more among women belonging to Hindu, Muslim, or Buddhist religion as compared to Christians and others in the present survey. In the GATS India survey, the use of SLT was reported to be very high among the Buddhist women and rather low among the Christian women.[7] In the NFHS-2 survey, tobacco consumption was significantly more among the scheduled castes and scheduled tribe populations.[21] A study on SLT consumption among married women in rural Bangladesh found its use to be more among Muslim women.[20] In the present survey, tobacco consumption was associated with illiteracy. The relation of illiteracy and low education level with tobacco consumption has also been reported in several other surveys and reports from different regions.[7,13,14,17,18,19,20,21,22] In the present survey though only one category of low per capita family income was significantly associated with tobacco consumption, a clear trend of lower income related to higher tobacco consumption was observed. Tobacco use has been associated with poverty and lower socioeconomic status in many reports.[13,19,20,22] The risk of tobacco consumption was more among manual laborers in the present survey. In the GATS India report, the use of tobacco was lower among students and home makers as compared to self-employed, government, or nongovernment employees, retired, and unemployed.[7] The divorced or separated were at higher risk of being a tobacco user as compared to other women in the present study. The SLT consumption was associated with being widowed[17] in the North Carolina study and being divorced, separated, or widowed in a study from Bangladesh.[20]
SLT, and women and tobacco are globally emerging health issues that need to be well understood and properly addressed. Though a lot of work has been done with regards to understanding the science and consequences of smoking tobacco, the same remains incomplete for SLT. Although the present paper presents local data of SLT use among women, the predictors of its use are likely to remain similar for the region. This issue needs to be seriously addressed as the SLT market is expected to increase globally in the coming years.
Acknowledgments
We gratefully acknowledge the funding support for the present service program through the Department of Atomic Energy (DAE) under the XIth 5 years plan period. The patient care cost is partly subsidized by the Tata Memorial Hospital, and the rest is supported by the DAE and the Women's Cancer Initiative (WCI). A mobile vehicle for screening was donated to the project by the WCI. The sponsors (DAE and WCI) had no role in planning, designing, or conducting the program. The authors wish to acknowledge the contributions of the following persons who have been directly or indirectly associated with the program, namely Pranoti Satpute, Padma Sadalge, Nabha Kadam, Neha Malaiya, Sharmila Pimple, Pallavi Uplap, Yogesh Kumar, Srikant Atreya, Nilesh Ingole, Kavita Anand, Parishi Majmudar, Rajendra Kerkar, Amita Maheshwari, Rajendra Badwe, Vani Parmar, Neeta Nair, Meenakshi Thakur, Subhash Ramani, Shubhada Kane, Ajit Dulhan, and all the staff working for this project.
Financial support and sponsorship
The study was supported by the Department of Atomic Energy (DAE), Government of India under the XIth 5 years plan. Tata Memorial Hospital is partly subsidized the treatment cost for the patients and part of it was supported by the Women's Cancer Initiative (WCI) and the DAE. The WCI also donated a mobile screening vehicle for the program.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.WHO Report on the Global Tobacco Epidemic, 2011 . Geneva: World Health Organization; 2011. [Last accessed on 2014 Oct 13]. WHO Report on the Global Tobacco Epidemic, 2011. Available from: http://www.who.int/tobacco/global_report/2011/en/ [Google Scholar]
- 2.Giovino GA, Mirza SA, Samet JM, Gupta PC, Jarvis MJ, Bhala N, et al. Tobacco use in 3 billion individuals from 16 countries: An analysis of nationally representative cross-sectional household surveys. Lancet. 2012;380:668–79. doi: 10.1016/S0140-6736(12)61085-X. [DOI] [PubMed] [Google Scholar]
- 3.Research and Markets: Global Smokeless Tobacco Market Report: 2010 Edition. [Last accessed on 2014 Oct 14]. Available from: http://www.bloomberg.com/apps/news?pid=newsarchive&sid=ay63Vy1ALVI8 .
- 4.SAMHSA, Office of Applied Studies, National Survey on Drug Use and Health, 2004 and 2005. [Last accessed on 2014 Oct 15]. Available from: http://www.oas.samhsa.gov/NSDUH/2k5nsduh/tabs/Sect2peTabs37to41.pdf .
- 5.Thomsen M, Ahlbom A, Bridges J, Rydzynski K. Health Effects of Smokeless Tobacco Products. Scientific Committee on Emerging and Newly Identified Health Risks. SCENIHR European Commission Report. [Last accessed on 2014 Oct 13]. Available from: http://www.ec.europa.eu/health/ph_risk/committees/04_scenihr/docs/scenihr_o_013.pdf .
- 6.Reddy KS, Gupta PC, editors. Report on Tobacco Control in India (New Delhi, India) New Delhi, India: Ministry of Health & Family Welfare. 2004. [Last accessed on 2014 Oct 14]. Available from: http://www.mohfw.nic.in/WriteReadData/l892s/4898484716Report%20on%20Tobacco%20Control%20in%20India.pdf .
- 7.Global Adult Tobacco Survey (GATS): India: 2009-2010. Published by IIPS, Mumbai and Funded by the Ministry of Health and Family Welfare, GOI. 2010. [Last accessed on 2014 Oct 15]. Available from: http://www.searo.who.int/LinkFiles/Regional_Tobacco_Surveillance_System_GATS_India.pdf .
- 8.Bhat PN, Arnold F, Gupta K, Kishore S, Parasuraman S, Arokiosamy P, et al. National Family Health Survey (NFHS-3), 2005-06, India. 1st ed. I. Mumbai: International Institute for Population Sciences (IIPS) and Macro International; 2007. [Last accessed on 2014 Oct 15]. Morbidity and health care; p. 43. Available from: http://www.pdf.usaid.gov/pdf_docs/PNADK385.pdf . [Google Scholar]
- 9.Sinha DN, Gupta PC, Ray C, Singh PK. Prevalence of smokeless tobacco use among adults in WHO South-East Asia. Indian J Cancer. 2012;49:342–6. doi: 10.4103/0019-509X.107726. [DOI] [PubMed] [Google Scholar]
- 10.Somatunga LC, Sinha DN, Sumanasekera P, Galapatti K, Rinchen S, Kahandaliyanage A, et al. Smokeless tobacco use in Sri Lanka. Indian J Cancer. 2012;49:357–63. doi: 10.4103/0019-509X.107729. [DOI] [PubMed] [Google Scholar]
- 11.Gupta PC. Survey of sociodemographic characteristics of tobacco use among 99,598 individuals in Bombay, India using handheld computers. Tob Control. 1996;5:114–20. doi: 10.1136/tc.5.2.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chollat-Traquet C. Women and Tobacco. WHO. 1992. [Last accessed on 2014 Oct 17]. Available from: http://www.apps.who.int/iris/bitstream/10665/37510/1/9241561475_engpdf?ua=1 .
- 13.Sreeramareddy CT, Pradhan PM, Mir IA, Sin S. Smoking and smokeless tobacco use in nine South and Southeast Asian countries: Prevalence estimates and social determinants from Demographic and Health Surveys. Popul Health Metr. 2014;12:22. doi: 10.1186/s12963-014-0022-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pratinidhi A, Gandham S, Shrotri A, Patil A, Pardeshi S. Use of ‘Mishri’ A smokeless form of tobacco during pregnancy and its perinatal outcome. Indian J Community Med. 2010;35:14–8. doi: 10.4103/0970-0218.62547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vol. 85. IARC; 2004. [Last accessed on 2014 Oct 17]. Betel-Quid and Areca-Nut Chewing and Some Areca-Nut-Derived Nitrosamines. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; p. 230. Available from: http://www.monographs.iarc.fr/ENG/Monographs/vol85/mono85.pdf . [PMC free article] [PubMed] [Google Scholar]
- 16.Chockalingam K, Vedhachalam C, Rangasamy S, Sekar G, Adinarayanan S, Swaminathan S, et al. Prevalence of tobacco use in urban, semi urban and rural areas in and around Chennai City, India. PLoS One. 2013;8:e76005. doi: 10.1371/journal.pone.0076005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Spangler JG, Bell RA, Dignan MB, Michielutte R. Prevalence and predictors of tobacco use among Lumbee Indian women in Robeson County, North Carolina. J Community Health. 1997;22:115–25. doi: 10.1023/a:1025112822200. [DOI] [PubMed] [Google Scholar]
- 18.Abdullah AS, Driezen P, Ruthbah UH, Nargis N, Quah AC, Fong GT. Patterns and predictors of smokeless tobacco use among adults in Bangladesh: Findings from the International Tobacco Control (ITC) Bangladesh survey. PLoS One. 2014;9:e101934. doi: 10.1371/journal.pone.0101934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Palipudi KM, Sinha DN, Choudhury S, Zaman MM, Asma S, Andes L, et al. Predictors of tobacco smoking and smokeless tobacco use among adults in Bangladesh. Indian J Cancer. 2012;49:387–92. doi: 10.4103/0019-509X.107745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hossain MS, Kypri K, Rahman B, Arslan I, Akter S, Milton AH. Prevalence and correlates of smokeless tobacco consumption among married women in rural Bangladesh. PLoS One. 2014;9:e84470. doi: 10.1371/journal.pone.0084470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rani M, Bonu S, Jha P, Nguyen SN, Jamjoum L. Tobacco use in India: Prevalence and predictors of smoking and chewing in a national cross sectional household survey. Tob Control. 2003;12:e4. doi: 10.1136/tc.12.4.e4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Thakur JS, Prinja S, Bhatnagar N, Rana S, Sinha DN. Socioeconomic inequality in the prevalence of smoking and smokeless tobacco use in India. Asian Pac J Cancer Prev. 2013;14:6965–9. doi: 10.7314/apjcp.2013.14.11.6965. [DOI] [PubMed] [Google Scholar]