

Pulmonary embolism resulting from deep vein thrombosis (DVT) of leg veins is a frequent and preventable cause of death among hospitalized patients. Most of the patients admitted in medical or surgical wards have one or more risk factors for DVT putting these patients at higher risk of acquiring venous thromboembolism (VTE) and its complications. Yet, among hospital staff, compliance with VTE prophylaxis is quite variable, and frequently, suboptimal.1 Data on the use of VTE prophylaxis among hospitalized patients in the Kingdom of Saudi Arabia (KSA), especially the Southern region are limited. We studied the usage and methods of VTE prophylaxis in a mixed cohort of in-hospital patients in the Aseer region of KSA.
All in-patients at the Aseer Central Hospital on 20th July 2014 were assessed for the utilization and mode of prophylaxis for VTE. This was performed by on-site physical review of the case files and medication sheets of all patients admitted for 48 hours or more in the general wards, high dependency areas, and intensive care units (ICUs) of the hospital. Eligibility for thromboprophylaxis was ascertained as per the standard hospital practice.2 Data were collected regarding: a) use or no use of VTE prophylaxis; and b) the method of VTE prophylaxis used. Patients in day-care units and those visiting the hospital for brief treatments for less than 2 days were not included. Patients admitted with or receiving therapeutic treatment for diagnosed acute DVT were also excluded; however, patients receiving long-term prophylaxis for VTE before current hospitalization were included.
Of the eligible 297 patients (mean age; 42.85 years, 61% males) included in the study, 236 (80%) received VTE prophylaxis, while 59 (20%) did not receive any prophylaxis. Pharmacological prophylaxis was used in all but one of the patients receiving thromboprophylaxis. Low molecular weight heparin was used in 144 (49%) patients, while unfractionated heparin was used in 86 (29%); the rest were on warfarin. The only patient who received mechanical thromboprophylaxis was placed on a foot pump (Figure 1). Among the hospital units, the usage of VTE prophylaxis was the highest in the ICUs, where 100% of the patients received prophylaxis. Our results suggest that the usage of thromboprophylaxis among hospitalized patients at Aseer Central Hospital is fairly adequate. Low molecular weight heparin is the predominant modality of VTE prophylaxis employed.
Figure 1.
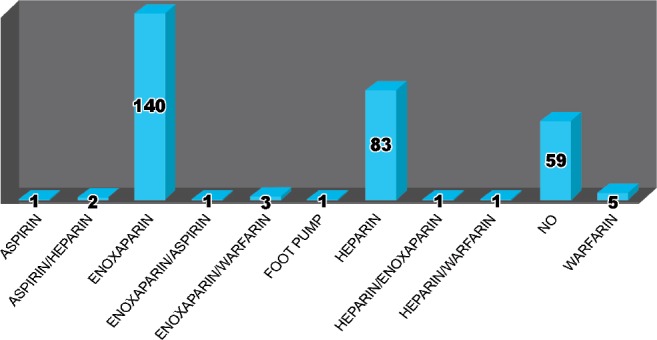
Frequency and methods of thromboprophylaxis used in 297 hospitalized patients. The numbers represent the absolute number of patients receiving the particular method of prophylaxis. Overall, 80% patients received prophylaxis, mostly using medications. Enoxaparin was the most commonly used pharmacotherapy for thromboprophylaxis followed by unfractionated herapin.
Compliance with usage of the recommended VTE prophylaxis in hospitalized patients has been generally found to be dismal around the world.1 In the Epidemiologic International Day for the Evaluation of Patients at Risk for Venous Thromboembolism in Acute Hospital Care Setting (ENDORSE) study, a multinational cross-sectional survey was conducted to assess the prevalence of VTE risk and the use of VTE prophylaxis in the acute hospital care setting. Surprisingly, only 58.5% of the surgical patients, and 39.5% of medical patients at risk of VTE received recommended VTE prophylaxis.3
In KSA, the burden of thromboembolic disorders is believed to be huge. Limited studies available show a serious under-utilization of effective VTE prophylaxis among the hospitalized patients across the Kingdom. In a recent retrospective study involving 968 patients at a tertiary care hospital in the Eastern region of KSA, only half of the patients at risk of VTE received any form of prophylactic therapy, and an even smaller percentage of them received the recommended VTE prophylaxis.4 Consistent with these studies, the utilization rate of VTE prophylaxis among hospitalized patients in the present study are also suboptimal, although marginally better than some other series. In a similar one-day observational study at a tertiary care hospital in Riyadh, only approximately 47% of eligible patients in acute medical wards were found to be receiving appropriate VTE prophylaxis.5 Our observations further underscore the need for increasing the awareness on, and ensuring compliance with the use of effective VTE prophylactic therapies among hospitalized patients in the kingdom and elsewhere.
A limitation of this study is that it only examined a cross-sectional view of the use of VTE prophylaxis on one day in a tertiary care hospital, which limits the generalizability of the conclusions to general hospital practice. However, it provides an insight into the compliance with this important preventive practice at the Kingdom’s hospitals. Larger prospective studies involving multiple healthcare settings at different levels are needed to more adequately define the pattern and usage of VTE prophylaxis in KSA.
Footnotes
References
- 1.Hill J, Treasure T. National Clinical Guideline Centre for Acute and Chronic Conditions. Reducing the risk of venous thromboembolism in patients admitted to hospital: summary of NICE guidance. BMJ. 2010;340:c95. doi: 10.1136/bmj.c95. [DOI] [PubMed] [Google Scholar]
- 2.Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schuünemann HJ. American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel. Executive summary: Antithrombotic Therapy and Prevention of Thrombosis 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):S7–S47. doi: 10.1378/chest.1412S3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cohen AT, Tapson VF, Bergmann JF, Goldhaber SZ, Kakkar AK, Deslandes B, et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet. 2008;371:387–394. doi: 10.1016/S0140-6736(08)60202-0. [DOI] [PubMed] [Google Scholar]
- 4.Rehmani RS, Memon JI, Alaithan A, Ghabashi A, Shahid K, Latif S, et al. Venous thromboembolism risk and prophylaxis in a Saudi hospital. Saudi Med J. 2011;32:1149–1154. [PubMed] [Google Scholar]
- 5.Saeed MA, Hassan IS. Deep venous thrombosis prophylaxis at the Department of Medicine, King Abdulaziz Medical City, Riyadh. Ann Thorac Med. 2012;7:52. doi: 10.4103/1817-1737.91550. [DOI] [PMC free article] [PubMed] [Google Scholar]