

Abstract
Background
An inadequate level of flexibility of the adductor muscles is one of the most critical risk factors for chronic groin pain and strains. However, measurement methods of adductor muscle flexibility are not well defined.
Purpose
To determine the inter‐session reliability of the biarticular and monoarticular adductor muscle flexibility measures obtained from passive hip abduction with the knee flexed over the edge of the plinth test (PHA) and the passive hip abduction test at 90° of hip flexion (PHA90°).
Study design
Clinical Measurement Reliability study.
Methods
Fifty healthy recreational athletes participated in this study. All participants performed the PHA and PHA90° on four different occasions, with a two‐week interval between testing sessions. Reliability was examined through the change in the mean between consecutive pairs of testing sessions (ChM), standard error of measurement expressed in absolute values (SEM) and as a percentage of the mean score (%SEM), minimal detectable change at 95% confidence interval (MDC95), and intraclass correlation coefficients (ICC2,k).
Results
The findings showed negligible or trivial ChM values for the two adductor flexibility measures analyzed (<2°). Furthermore, the SEM and MDC95 were 2.1° and 5.9° and 2.2° and 6.2° for the measures obtained from the PHA and PHA90°, respectively, with %SEM scores lower than 5% and ICC scores higher than 0.90.
Conclusion
The findings from this study suggest that the adductor muscle flexibility measures analyzed have good to excellent inter‐session reliability in recreational athletes. Thus, clinicians can be 95% confident that an observed change between two measures larger than 5.9° and 6.2° for the flexibility measures obtained from the PHA and PHA90°, respectively, would indicate a real change in muscle flexibility.
Level of evidence
2
Keywords: Groin injury, muscle strain, physical therapy, range of motion, reproducibility
INTRODUCTION
Clinicians and sports medicine practitioners routinely assess and monitor the flexibility of the primary muscles involved in the hip joint abduction movement (biarticular muscles: gracilis; monoarticular muscles: adductor brevis, adductor longus, adductor magnus, pectineus and obturador externus) because it has been postulated that an inadequate level of flexibility is one of the most important risk factors for chronic groin pain and adductor muscle strains, particularly in athletes.1,2 Specifically, it has been suggested that having insufficient flexibility of the hip adductor muscles (mainly the biarticular muscles) might result in greater stress across the superior pubic ramus and pubic symphysis during powerful weight‐bearing sporting actions, increasing the likelihood of sustaining a chronic groin injury.2 It has also been suggested that participants in sports involving high numbers of repetitive, high intensity bouncing, sprinting, or sudden turning and jumping movements (e.g., soccer, ice hockey, rugby) who have insufficient flexibility in the hip adductor muscles (both biarticular and monoarticular muscles) are more prone to suffer a muscle strain3 because the demands in energy absorption generated during the above‐mention tasks may rapidly exceed the capacity of the adductor muscles.4
The passive hip abduction with knee flexed over the edge of the plinth test (PHA; Figure 1) and the passive hip abduction test at 90° of hip flexion (PHA90°; Figure 2) are the measurement methods described in the most prominent sports medicine textbooks5‐7 to assess the flexibility of the biarticular and monoarticular hip adductor muscles, respectively. However, before these two measurement methods can be used to identify athletes at an increased risk of injury and establish progress from training and/or rehabilitation programs, the validity and reliability of their outcomes must be determined.8 Although the PHA and PHA90° are indirect measures of the biarticular and monoarticular adductor muscle flexibility, these two tests have been considered appropriate by the most important American medical organizations.9,10
Figure 1.
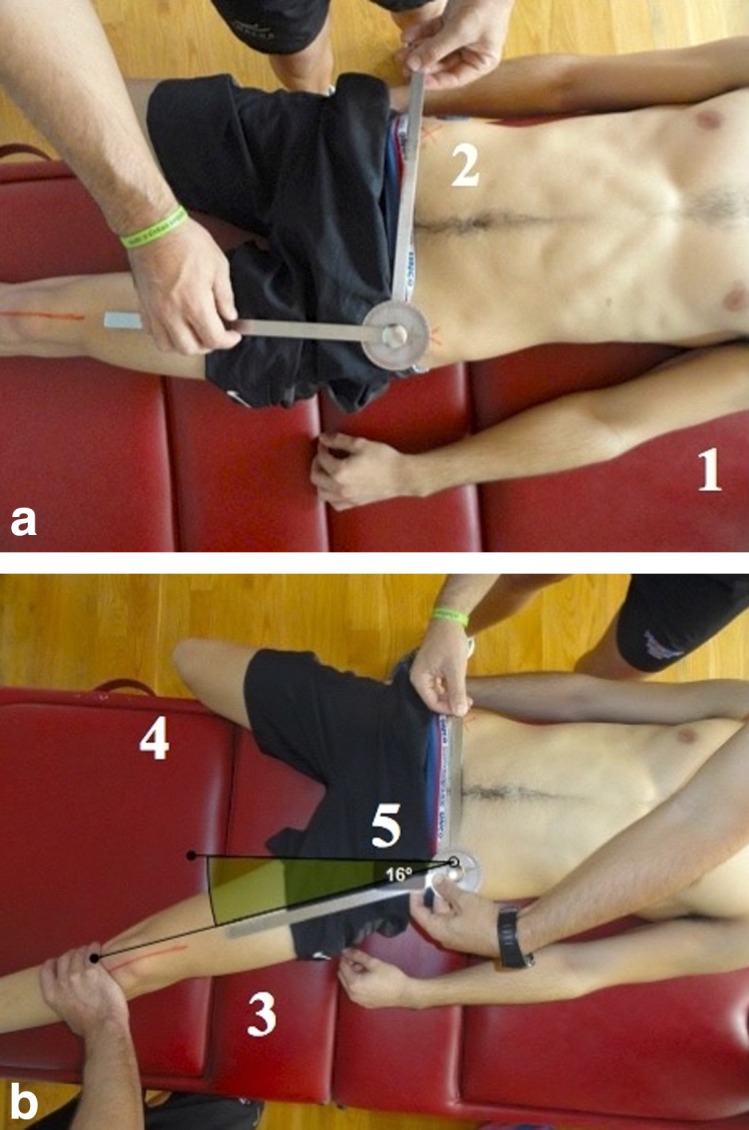
Passive hip abduction with knee flexed over the edge of the plinth test.
Starting Position (Figure 1a):
The subject lies supine on the plinth with the contralateral leg hangs off the side of the plinth and the tested leg extended and placed on the plinth as shown (1).
Goniometer placement process:
The tester places one goniometer arm joining both anterior‐superior iliac spines and the other arm is placed over the anterior face of the tested limb following its bisector line, as shown (2).
Testing movement (Figure 1b):
The assistant tester performs a slow and progressively hip abduction movement with knee extended (neutral position “0”), as shown (3).
Stabilization:
The assistant tester must avoid rotation of the lower limb. The contralateral extremity (non‐tested) is fixed to the plinth by flexion of the knee to approximately 90° as shown (4).
Measurement:
The tester reads and records the abduction measurement angle formed by the two goniometer arms, in this case 16° as shown (5).
Notes: There are some compensatory movements that must be taken into account: Lateral inclination of the contralateral pelvis, the extension of the contralateral knee, and/or the rotation of the tested limb.
Figure 2.

Passive hip abduction test at 90° of hip flexion.
Starting Position (Figure 2a):
The subject lying supine on the plinth. The tested hip placed in 90° of flexion with the knee flexed in a confortable position as shown (1).
Inclinometer calibration process:
The inclinometer must be placed in the vertical plane (0 degrees), as shown (2).
Testing movementFigure 2b):
The tester performs a slow and progressive hip abduction movement with the knee flexed and hip remaining at 90° as shown (3).
Stabilization:
The assistant tester presses on the anterior surface of the contralateral hemipelvis to avoid its rotation. Further, he must hold the external surface of the contralateral limb firmly on the plinth as shown (4).
Measurement:
The inclinometer´s telescopic arm must be placed over the anterior surface of the tested limb following its parallel imaginary bisector line. Then, the tester reads and records the angle formed by the longitudinal axis of the anterior surface of the limb from the vertical plane as shown (5), in this case 33°.
Notes: Because the hip is flexed, the ischiofemoral, pubofemoral and the iliofemoral ligaments are slackened. Thus, any limitation in the hip abduction movement is mainly attributed to the monoarticular adductor muscles and not the ligaments. If the subject tested has very good muscle‐tendon flexibility, then abduction movement could be limited by bony contact of the femoral neck with the acetabular rim.
Regarding the reliability of these tests, only three studies (to the authors’ knowledge) have addressed the examination of the inter‐session reliability (defined as the day‐to‐day variability in measurements) of the measure obtained from the PHA, showing moderate to high scores.11‐13 However, two of the three above‐mentioned studies11,13 analyzed the inter‐session reliability of the measure obtained from the PHA using video captures and computer‐based 3D analysis. This measurement instrument (3D video analysis) increases the time required to conduct the test and, hence, reduces the external validity of the measure because is not possible to assess a patient or athlete in mere seconds or minutes. In addition, the video analysis software might slightly deform the electronic images, prejudicing, and consequently, increasing the difficulty of identifying anatomic landmarks. Only one study10 used a standard goniometer to determine the inter‐session reliability of the measure obtained from the PHA. The use of a goniometer as the key instrument of measure may allow practitioners to assess hip adductor muscle flexibility with just one trial and produce results directly in degrees, reducing both the time demands of the test and its difficulty.14 Surprisingly, no studies have examined the reliability of the PHA90°. The determination of the inter‐session reliability of the measures obtained from the PHA and PHA90° is important for clinicians, coaches, physicians and scientists, as if determined reliable, they can be used to estimate the magnitude of individual differences in the response to treatment and monitor the performance or health of their patients and athletes.15 Therefore, the purpose of this study was to estimate the inter‐session reliability of the biarticular and monoarticular adductor muscle flexibility measures obtained from PHA and PHA90° tests in recreational athletes.
METHODS
A convenience sample of 25 male (age: 22.2 ± 2.5 years; stature: 175.8 ± 5.6 cm; body mass: 74.1 ± 6.1 kg) and 25 female (age: 20.9 ± 0.9 years; statute: 166.5 ± 7.2 cm; body mass: 61.8 ± 7.7 kg) university students who were recreationally active (engaging in 1.5 h of moderate physical activity 3–4 days per week) completed this study. Although all participants reported engaging in recreational sports (i.e., football, basketball, running), none were involved in a systematic and specific strength and flexibility training program. Participants were instructed to maintain their regular training regimens throughout the experimental period and not to take part in any vigorous physical activity 48 h preceding each testing day.
The exclusion criteria were: (1) episodes of groin and/or adductor injury over the previous six months, (2) missing a testing session, and (3) the presence of self‐reported delayed onset muscle soreness at any testing session. The participants were verbally informed about the study's procedures before testing, and they provided written informed consent. The study was approved by the University Office for Research Ethics (DPS.FAR.01.2014), and conformed to the Declaration of Helsinki.
The test‐retest reliability of the biarticular and monoarticular hip adductor muscle measures obtained from the PHA and PHA90°, respectively, was analyzed using a repeated measures design. Thus, each participant underwent the testing procedure twice on four different occasions with a two‐week interval between testing sessions. The rationale for using 50 participants and four testing sessions to determine the reliability in our study (instead of the two testing sessions that have been typically used in previous reliability studies) was based on the simulations run by Hopkins,8 who stated that, in order to achieve an accurate reliability assessment, a minimum of three testing sessions and 50 participants were needed.
Two physical therapists with greater than 10 years’ experience (one conducted the tests and the other ensured the maintenance of proper testing position of the participants throughout the assessment maneuver) conducted each of the four testing sessions at the same time of the day under the same environmental conditions. The physical therapists were blinded to the purpose of the study and test results from previous testing sessions.
A pre‐test warm‐up routine was not performed in an attempt to reflect real sports and clinic conditions. Participants were instructed to perform two maximal trials of the PHA and PHA90° for each limb in a randomized order, and the mean score for each test was used in the subsequent analysis. The mean of the two trials of the PHA and PHA90° performed at each testing session was used for subsequent statistical analyses instead of the highest score because the magnitude of the error component decreased when the scores were averaged.16 Patients who did not tolerate the sensation of stretching or with low experience with it might set the endpoint of a trial of the test before achieving his/her peak hip abduction range of motion peak score due to a feeling of apprehension. To avoid the possible influence of this source of error on the stability of the measure, when a variation >5% was found in the range of motion values between the two trials, an extra trial was performed, and the two most closely related trials were used for the subsequent statistical analyses. Participants were examined wearing sports clothes and without shoes. The participants were allowed to rest for 30 s between trials, limbs, and tests.
An ISOMED inclinometer (Portland, Oregon) with a telescopic arm was used as the key measure for the PHE90° test, while a flexible adjustable long arm goniometer was employed for the PHA test. The inclinometer was consistently leveled to a vertical reference before each measurement. A low‐back protection support (Lumbosant, Murcia, Spain) placed beneath the low back of each participant was used to standardize the lordotic curve (15°) during the both tests. Variations in pelvic position and stability may affect the final score of several measurements of hip movement range of motion.17 Thus, to accurately measure hip joint range of motion, the assessment procedure in this study provided reproducible stabilization of the pelvis using an assistant clinician during all tests.
The endpoint for each test was determined by one or more of these three criteria: (a) the examiner's perception of firm resistance, (b) the palpable onset of pelvic rotation, and (c) the participant feeling a strong but tolerable stretch, slightly before the occurrence of pain.
For a better understanding of the assessment methods (i.e., instrumental, clinician positioning, final point), additional descriptions of the PHA and PHA90° tests are displayed in Figures 1 and 2, respectively.
Prior to the statistical analysis, the distributions of raw data sets were checked using the Kolmogorov‐Smirnov test, which demonstrated that all data had a normal distribution (p > 0.05). Men and women were not analyzed separately based on the fact that previous studies have reported that, in both sexes, the baseline joint ROM responds in the same way whether or not specific and systematic flexibility training is performed.18,19 Descriptive statistics were calculated for the hip adductor muscle flexibility measurements. Paired t‐tests were used to test for differences between the scores of the dominant and non‐dominant limbs.
The test‐retest reliability of the hip adductor muscle flexibility measures was determined through the change in the mean (ChM), standard error of measurement (SEM), the minimal detectable change at a 95% confidence interval (MDC95) and intraclass correlations (ICC2k).20 The test‐retest reliability for the hip adductor muscle flexibility measures was calculated separately for the consecutive pairs of trials (2‐1, 3‐2, 4‐3) to be consistent with the interval time between testing sessions (two weeks).8
The ChM was estimated using a spreadsheet designed by Hopkins21 via the unequal‐variances t‐statistic computed for changes in scores between paired sessions. To make inferences about the true value of the effect, the uncertainty in the effect was expressed as 90% confidence intervals and as likelihoods that the true value of the effect represented substantial change (negative or positive).22 The probability that the true value of the effect was positive or negative was inferred as follows: < 0.5%, most unlikely; 1–5%, very unlikely; 6–25%, unlikely; 26–75%, possibly; 76–95%, likely; 96‐99%, very likely; > 99%, most likely.19 The SEM was calculated using the raw data via the following formula: √MSE, where MSE is the error mean square from the repeated measures analysis of variance. The MDC95 was calculated as SEM × √2 × 1.96. The ICC2.k were calculated using the following formula:
where MSS is the subject's mean square, MSE is the error mean square, MST is the trials mean square, n is the sample size and k is the number of trials. Magnitudes of correlations were assessed using the following scale of thresholds: < 0.80 low, 0.80–0.90 moderate, and >0.90 high.8
RESULTS
Descriptive statistics (mean ± standard deviation for testing session 1) for each variable are displayed in Table 1. The paired t‐test analysis reported no significant differences between the dominant and non‐dominant legs for both the biarticular (PHA: mean difference less than 0.7°; p > 0.05; degrees of freedom 49; t‐statistic ranged from ‐1.01 to 0.01) and monoarticular (PHA90°: mean difference less than 1.3°; p > 0.05; degrees of freedom, 49; t‐statistic ranged from ‐0.9 to 1.6) hip adductor muscle flexibility measures analyzed in each testing session; therefore, the average of the two legs was used for subsequent reliability analyses.
Table 1.
Descriptive values (mean ± standard deviation [SD] for testing session 1) for PHA and PHA90° measurements and test‐retest reliability statistics: change in the mean between consecutive testing sessions (ChM), standard error of measurement (SEM), minimal detectable change at 95% confidence interval (MDC95) and intraclass correlation coefficients (ICC2, K).
| Test | Testing Session 1 | Testing Session 2 ‐ Testing Session 1 | Testing Session 3 ‐ Testing Session 2 | Testing Session 4 ‐ Testing Session 3 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD (º) | ChM | SEM | %SEM | MDC95 | ICC | ChM | SEM | %SEM | MDC95 | ICC | ChM | SEM | %SEM | MDC95 | ICC | |
| PHA | 52.5 | −0.6 | 2.9 | 5.5 | 8.1 | 0.92 | 0.4 | 1.5 | 2.9 | 4.2 | 0.97 | −1.2 | 1.9 | 3.7 | 5.4 | 0.99 |
| PHA90° | 64.4 | 1.8 | 2.7 | 4.2 | 7.6 | 0.99 | −0.2 | 2.2 | 3.5 | 6.0 | 0.99 | −0.4 | 1.8 | 2.9 | 5.1 | 0.99 |
PHA: passive hip abduction with knee flexed over the edge of the plinth test; PHA90°: passive hip abduction test at 90° of hip flexion; º: degrees.
Reliability statistics (ChM, SEM, %SEM, MDC95 and ICC) for the PHA and PHA90° values are also presented in Table 1 separately for the three consecutive pairs of testing sessions. The reliability scores obtained for each of the consecutive paired testing sessions (2‐1, 3‐2 and 4‐3) were almost identical, and the mean of the two paired testing sessions for each flexibility measure might be used as a reliability criterion of reference.8
The ChMs between consecutive pairs of testing sessions (2‐1, 3‐2, 4‐3) were “most likely trivial” (p > 0.05; trivial effect with a probability of >95%, mean difference ranged from ‐0.6 to 1.8°) for both biarticular and monoarticular hip adductor muscle flexibility measures. The SEM and MDC95 for both biarticular and monoarticular flexibility measures ranged from 1.5° to 2.9° and from 4.2° to 8.1°, respectively, with %SEM scores lower than 5% and ICC scores higher than 0.91.
DISCUSSION
The purpose of this study was to determine the inter‐session reliability of the biarticular and monoarticular adductor muscle flexibility measures obtained from PHA and PHA90° tests in recreational athletes. In this regard, the results of the current study showed that the biarticular and monoarticular adductor muscle flexibility measures analyzed had excellent inter‐session reliability scores.
The ChM between consecutive testing sessions was negligible or trivial for both the biarticular (ranged from ‐1.2° to 0.4°) and the monoarticular (ranged from ‐0.4° to 2.2°) adductor muscle flexibility measures. Similar ChM scores were reported by Cejudo et al.12 and Fourcher et al.13 for the biarticular adductor flexibility measure obtained from the PHA test in adolescent athletes, futsal and handball players. Thus, the findings of the current study, in conjunction with findings from previously conducted research, may support the idea that both testing procedures are simple to administer and the instructions are easy to follow for the patients/athletes because no systematic error associated with learning effects or insufficient recovery time was found. In addition, this finding also indicates that, in the absence of a systematic flexibility training program, the hip adductor muscle flexibility tendency over time may be considered stable and linear in uninjured athletes.
Another aspect of reliability that was assessed was the precision of measurements, which was determined using the SEM.20 Admittedly, the clinical decision regarding the cut‐off precision values of a measure is challenging, especially since there are no clear guidelines for reference value establishment, and there is the potential need to evaluate multiple factors (training status, sex, age) to reach a knowledgeable decision. However, it appears to be accepted that variability of a measure lower than 10% could be considered appropriate for clinical and research purposes.16,23 Based on this criterion, the biarticular and monoarticular adductor muscle flexibility measures analyzed in this study showed very good precision, since their percentage of variability (%SEM) ranged from 2.9 to 5.5% and from 2.9 to 4.2% for PHA and PHA90°, respectively.
In terms of practical applications, it has been suggested that the MDC95 can be used to indicate the limit for the smallest change that indicates a real improvement in a single person.20 Therefore, clinicians can be 95% confident that an observed change between two measures larger than 5.9° and 6.2° for the flexibility measures obtained from the PHA and PHA90°, respectively, would likely indicate a real change in hip adductor muscle flexibility.
The need of placing the tested hip and knee in approximately 90° of flexion during the hip abduction movement for the PHA90° test may have been a priori considered a source of error, as it makes the testing procedure more difficult than the PHA. However, the precision of measure scores in the current study were very good and similar to those found for the PHA. Perhaps the use of an inclinometer instead of a goniometer may have contributed to the good reliability scores reported for the PHA90°. In this sense, the elongation of the inclinometer´ telescopic arm makes it become a goniometer with only one arm, with the advantage of having a gravity level that provides an accurate measure. In addition, the inclinometer allows the physical therapist who conducts the tests to easily identify the same initial position (the parallel imaginary bisector line of the tested limb) during successive trials without estimating the joint movement center.24
Lower precision in measurement results has been reported by Fourcher et al.11 for the PHA. Specifically, Fourcher et al.13 reported precision of measurement expressed through a coefficient of variation (its magnitude is similar to %SEM) of approximately 7.2%.
One possible reason Fourcher et al.13 showed lower measurement precision scores for the PHA may be attributed to the different testing procedure and instrument of measurement used. In contrast with our study and also with previous ones,11,12 Fourcher et al.13 did not use a low‐back protection support to fix the pelvis in an attempt to minimize any movement that may bias the final score. In addition, Fourcher et al.13 used digital motion analysis software to obtain the peak hip abduction angle measure instead of a goniometer. The video analysis software might have slightly deformed the electronic images, prejudicing the identification of anatomic landmark procedures and, consequently, reducing the precision of the measure. A comparison of the precision of the results for the PHA90° obtained in the current research with other studies is not possible; because to the authors’ knowledge, this study is the first that has addressed this issue.
Finally, the results of the current study reported high relative reliability scores for the PHA (ICC > 0.90). Similar ICC scores have been reported by Cejudo et al.12 and, slightly lower scores by Fourcher et al.13 (ICC scores of 0.93 and 0.85, respectively).
While the results of this study have provided information regarding the intra‐tester reliability of these common musculoskeletal screening tests, limitations to the study must be acknowledged. The age distribution of participants was relatively narrow, and the generalizability to the broader population could not be ascertained. Similarly, whether the tests would be as reliable in a population of injured participants must be considered, although pre‐season screening is generally performed in healthy, uninjured populations. Finally, the use of two clinicians to carry out the tests appears to limits the practical application of these measurement methods in the sports and clinic contexts, especially for the PHA90°. As these measurement methods are simple to administer, the role of the assistant clinician (who provides suitable stabilization of the pelvis during all the tests) could be carried out by any postgraduate student or athletic trainer who performed one or two 10‐minute training sessions (statement based on the authors’ experience).
CONCLUSION
The findings from this study suggest that the adductor muscle flexibility measures analyzed have good inter‐session reliability in healthy recreational athletes. Thus, clinicians can be 95% confident that an observed change between two measures larger than 5.9° and 6.2° for the flexibility measures obtained from the PHA and PHA90°, respectively, would likely indicate a real change in muscle flexibility.
REFERENCES
- 1.Árnason Á Sigurdsson SB Gudmundsson A Holme I Engebretsen L Bahr R. Physical fitness, injuries, and team performance in soccer. Med Sci Sports Exerc. 2004;36:278‐285. [DOI] [PubMed] [Google Scholar]
- 2.Verrall GM Slavotinek JP Barnes PG Esterman A Oakeshott RD Spriggins AJ. Hip joint range of motion restriction precedes athletic chronic groin injury. J Sci Med Sport. 2007;10:463‐466. [DOI] [PubMed] [Google Scholar]
- 3.Hrysomallis C. Hip adductors’ strength, flexibility, and injury risk. J Strength Cond Res. 2009;23:1514‐1517. [DOI] [PubMed] [Google Scholar]
- 4.Witvrouw E Danneels L Asselman P D’Have T Cambier D. Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players a prospective study. Am J Sports Med. 2003;31:41‐46. [DOI] [PubMed] [Google Scholar]
- 5.Peterson‐Kendall F Kendall‐McCreary E Geise‐Provance P Rodgers M Romani W. Muscles Testing and Function with Posture and Pain, 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005. [Google Scholar]
- 6.Gerhardt JJ, Cocchiarella L, Lea RD. The American Medical Association. The Practical Guide to Range of Motion Assessment. Chicago, IL, USA: American Medical Association; 2002. [Google Scholar]
- 7.Prentice WE. The thigh, hip, groin, and pelvis. In: Arnheim's Principles of Athletic Training: A Competency‐Based Approach, 11th ed. New York, NY: McGraw Hill; 2003. [Google Scholar]
- 8.Hopkins WG. Measures of reliability in sports medicine and science. Sports Med. 2000;30:1‐15. [DOI] [PubMed] [Google Scholar]
- 9.American Academy of Orthopaedic Association. Joint Motion: Method of Measuring and Recording. Chicago, IL: Park Ridge; 1965. [Google Scholar]
- 10.American Medical Association. Guides to the Evaluation of Permanent Impairment. 4th ed. Milwaukee WI; American Medical Associaion; 2001. [Google Scholar]
- 11.NBozic PR Pazin NR Berjan BB Planic NM Cuk ID. Evaluation of the field tests of flexibility of the lower extremity: reliability and the concurrent and factorial validity. J Strength Cond Res. 2010;24:2523‐2531. [DOI] [PubMed] [Google Scholar]
- 12.Cejudo A Sainz de Baranda P Ayala F Santonja F. Test‐retest reliability of seven common clinical tests for assessing lower extremity muscle flexibility in futsal and handball players. Phys Ther Sport. 2015;16:107‐113. [DOI] [PubMed] [Google Scholar]
- 13.Fourchet F Materne O Horobeanu C Hudacek T Buchhelt M. Reliability of a novel procedure to monitor the flexibility of lower limb muscle groups in highly‐trained adolescent athletes. Phys Ther Sport. 2013;14:28‐34. [DOI] [PubMed] [Google Scholar]
- 14.Cejudo A Sainz de Baranda P Ayala F Santonja F. A simplified version of the weight‐bearing ankle lunge test: description and test‐retest reliability. Manual Ther. 2014;19:355‐359. [DOI] [PubMed] [Google Scholar]
- 15.Atkinson G Nevill AM. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998;26:217‐238. [DOI] [PubMed] [Google Scholar]
- 16.Vincent WJ. Statistics in Kinesiology, 2nd ed. Champaig IL: Human Kinetics; 1999. [Google Scholar]
- 17.Bohannon RW Gajdosik RL LeVeau BF. Relationship of pelvic and thigh motions during unilateral and bilateral hip flexion. Phys Ther. 1985;65:1501‐1504. [DOI] [PubMed] [Google Scholar]
- 18.Akbari A Moodi H Moein AA Nazok R. The effect of therapeutic ultrasound and duration of stretching of the hamstring muscle group on the passive knee extension. J Med Sci. 2000;6:968‐973. [Google Scholar]
- 19.Voigt L Vale RDS Abdala DW Freitas WD Novaes JDS Dantas EHM. Effects of a ten seconds repetition of incentive of the static method for the development of the young adult men's flexibility. Fitn Perform J. 2007;6:352‐356. [Google Scholar]
- 20.Weir JP. Quantifying test‐retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. 2005;19:231‐240. [DOI] [PubMed] [Google Scholar]
- 21.Hopkins WG. A spreadsheet for deriving a confidence interval, mechanistic inference and clinical inference from a p value. Sportscience. 2007;11:16‐20. [Google Scholar]
- 22.Hopkins W Marshall S Batterham A Hanin J. Progressive statistics for studies in sports medicine and exercise science. Med Sci Sports Exerc. 2009;41(1):3‐12. [DOI] [PubMed] [Google Scholar]
- 23.Atkinson G Nevill AM Edwards B. What is an acceptable amount of measurement errorϿ. The application of meaningful “analytical goals” to the reliability analysis of sports science measurements on a ratio scale. J Sports Sci. 1999;17:18. [Google Scholar]
- 24.Clapis PA Davis SM Davis RO. Reliability of inclinometer and goniometric measurements of hip extension flexibility using the modified Thomas test. Physiother Theory Pract. 2007;24:135‐141. [DOI] [PubMed] [Google Scholar]