

Summary
Background
Absence of the left circumflex artery (LCX) is an extremely rare congenital anomaly of the coronary circulation. While some coronary circulation anomalies are associated with significant complications, including sudden cardiac death and premature atherosclerosis, absence of the LCX is largely considered benign, though it has been associated with exertional chest pain, which may mimic acute coronary syndrome. Diagnosis is made when heart catheterization is performed in the work up for acute coronary syndrome or when computed tomography coronary angiography is performed during evaluation of coronary artery disease.
Case Report
We report a 55 year old female who presented with non-exertional chest pain in the setting of an emotional stressor. The initial work up was only significant for elevated troponins, and subsequent left heart catheterization revealed findings consistent with congenital absence of the LCX. No significant stenosis was appreciated, and no intervention was performed. Following catheterization, the patient’s troponins began to trend down, and her chest pain resolved.
Conclusions
Congenitally absent LCX is a rare entity detected when work up is performed to rule out acute coronary syndrome in patients presenting with exertional chest pain. This is the first reported case of chest pain unrelated to physical activity reported in a patient with an absent LCX. There is no specific treatment for an absent LCX; however, proper identification of this anomaly and differentiation from complete occlusion of the LCX is important in making an accurate diagnosis of myocardial ischemia and for choosing the best intervention when ischemia is present.
MeSH Keywords: Chest Pain, Congenital Abnormalities, Coronary Angiography, Coronary Vessel Anomalies
Background
Coronary anomalies are not uncommon, occurring in 0.3–0.9% [1] of patients evaluated with coronary angiography; the most common anomaly involves the LCX arising from the right coronary sinus, with an incidence of 0.18–0.67% [2]. However, complete absence of the LCX is an extremely rare occurrence, with a reported incidence of only 0.003% [1]. Among the few reported cases, imaging with either catheter angiography or computed tomography coronary angiography has consistently revealed the presence of a super-dominant right coronary artery (RCA) and enlarged diagonal branches from the left anterior descending artery (LAD) to supply the lateral wall of the left ventricle [3,4].
Case Report
We present a 55 year old previously healthy Hispanic female who presented after a single 5-minute episode of severe, non-radiating retrosternal chest pain and shortness of breath. She related the pain to significant emotional stress and anxiety, after she was informed of the death of her husband. The patient’s physical exam, electrocardiography, and laboratory findings were benign, except for persistently elevated troponins on serial measurements (peak troponin I value of 0.28). Left heart catheterization revealed a congenital absence of the left circumflex coronary artery (LCX) as illustrated in Figure 1 and Video 1, with a super-dominant right coronary artery (RCA) with an extensive posterolateral ventricular branch (PLV) supplying the territory normally supplied by the LCX, illustrated in Figure 2 and Video 2. The patient was diagnosed with a congenital absence of the LCX without evidence of atherosclerotic cardiovascular disease. Following left heart catheterization, the patient was free of chest pain and was discharged the following day with recommendations for lifestyle modifications and a prescription for aspirin 81 mg daily to cover for any underlying vascular disease.
Figure 1.
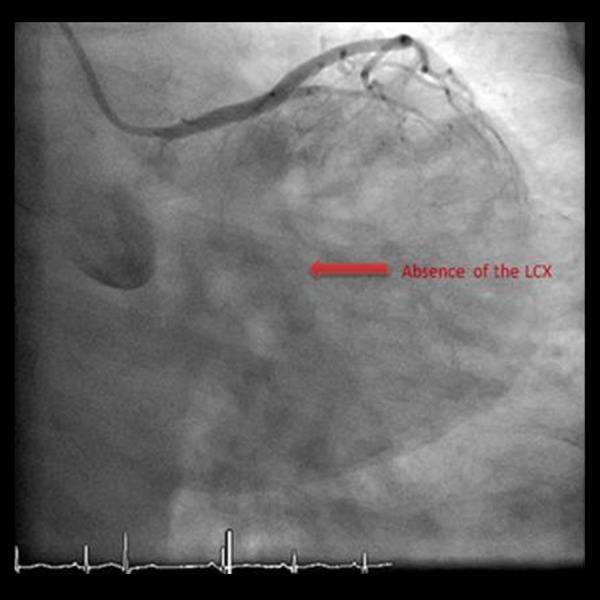
Left coronary angiogram showing absent LCX with a patent left main coronary artery and patent LAD (right anterior oblique caudal view).
Video 1.
Left coronary angiogram showing flow through the left main coronary artery and LAD, with absence of the LCX (corresponds to Figure 1).
Figure 2.
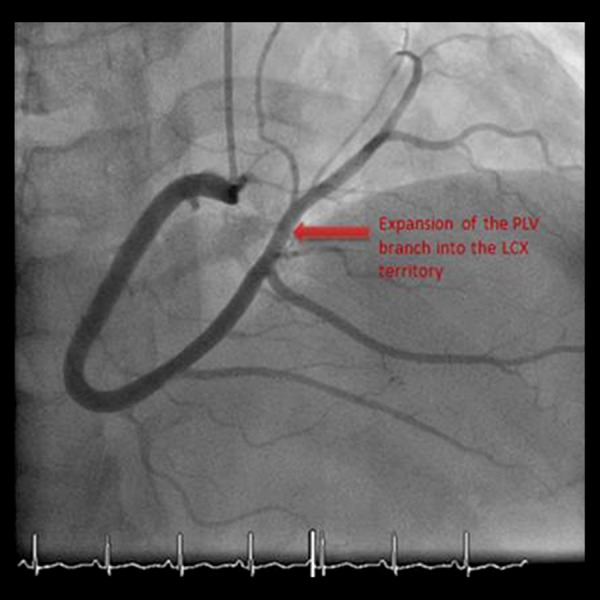
Super dominant RCA with PLV branch supplying the LCX territory (anterior-posterior cranial view).
Video 2.
Left coronary angiogram showing flow through the super dominant RCA and PLV (corresponds to Figure 2).
The major differential diagnosis for patients with suspected congenital absence of the LCX would be 100% occlusion at the base of the LCX. This was not the case in our patient because patients with 100% occlusion at the base of the LCX would reveal a trace amount of contrast at the ostium of the LCX, resulting in the visualization of a “stump” at the takeoff point of the LCX. No such “stump” was identified in our patient (Figure 1).
Discussion
Although considered a benign finding, absent LCX has been associated with chest pain, likely due to coronary steal phenomenon, where the myocardium normally supplied by the LCX steals blood flow away from the territories normally supplied by the RCA and diagonal branches of the LAD, resulting in transient ischemia of these territories [3]. Absent LCX has not been shown to be the precipitating factor of any major cardiac event, though it has been documented that patients with an absent LCX have presented with disease in other coronary beds; in these cases, the absence of the LCX was an incidental finding, and the patients were managed according to standard acute coronary syndrome protocol [4]. One case report describes a patient with absent LCX who presented with myocardial ischemia due to 90% occlusion of the super-dominant RCA, resulting in inferior, posterior and lateral wall myocardial infarction, which they reported as being equivalent to two-vessel disease involving both the RCA and LCX (this patient was treated with placement of bare-metal stents in the mid-RCA and mid-LAD) [5].
Other coronary anomalies have been associated with significant cardiac symptoms: coronary anomalies where the left coronary artery originates from the right coronary sinus or the right coronary artery originates from the left coronary sinus have been associated with sudden cardiac death during exertion; this occurs because exercise causes the aortic root and pulmonary trunk to dilate, resulting in compression of the anomalous vessel, which courses between the aorta and pulmonary trunk [1]. Anomalous origin of coronary arteries, particularly the LCX, have been associated with accelerated atherosclerosis, believed to be due to increased mechanical trauma, abnormal wall stress, and abnormal flow strain on the anomalous vessels [1].
While the absence of a LCX has yet to be significantly associated with any major cardiac event, identification of patients with this anomaly is crucial when performing cardiac interventions because patients with an absent LCX (or other coronary anomalies) are at increased risk of being misdiagnosed during cardiac catheterization procedures (e.g. congenitally absent LCX mistaken for 100% occlusion of the LCX), and they require extra care when performing cardiac bypass procedures to avoid accidental ligation or transection of anomalous vessels and to ensure that the grafts are placed properly to restore perfusion to ischemic myocardium [4,6].
Conclusions
Congenital absence of the LCX is a rare entity which is most often detected when work up is performed to rule out acute coronary syndrome in patients presenting with chest pain-usually during exertion, or, as in the presented case, following an emotional stressor. Left heart catheterization and computed tomography coronary angiography can confirm the diagnosis of absent LCX. There is no specific treatment for an absent LCX, as the condition is largely considered to be benign; however, proper identification of this anomaly and collateral circulation (super-dominant RCA and enlarged diagonal branches of the LAD) is important in making an accurate diagnosis of myocardial ischemia and for choosing the best intervention when ischemia is present. Proper identification of anomalous coronary anatomy is important in preventing accidental injury to anomalous vessels during bypass procedures and to ensure adequate reperfusion of ischemic myocardium.
References
- 1.Ali M, Hanley A, McFadden EP, Vaughan CJ. Coronary artery anomalies: A practical approach to diagnosis and management. Heart Asia. 2011;3:8–12. doi: 10.1136/ha.2010.003244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rissam HK, Garg L, Mittal UK, et al. Uncommon variants of left circumflex coronary artery (LCX): Evaluation with 256-slice dual source CT coronary angiography. BMJ Case Rep. 2015;2015 doi: 10.1136/bcr-2015-210495. pii: bcr2015210495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hongsakul K, Suwannanon R. Congenital absence of left circumflex artery detected by computed tomography coronary angiography: A case report. Case Rep Vasc Med. 2012;2012:204657. doi: 10.1155/2012/204657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ali FS, Khan SA, Tai JM, et al. Congenital absence of left circumflex artery with a dominant right coronary artery. BMJ Case Rep. 2009;2009 doi: 10.1136/bcr.08.2008.0772. pii: bcr08.2008.0772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Guo J, Xu M. Congenital absence of the left circumflex artery associated with inferior myocardial infarction. Intern Med. 2012;51(1):71–74. doi: 10.2169/internalmedicine.51.6141. [DOI] [PubMed] [Google Scholar]
- 6.Page HL, Engel HJ, Campbell WB, Thomas CS. Anomalous origin of the left circumflex coronary artery: Recognition, angiographic demonstration, and clinical significance. Circulation. 1974;50:768–73. doi: 10.1161/01.cir.50.4.768. [DOI] [PubMed] [Google Scholar]