

Abstract
Background
Burnout is typically viewed as an individual condition, and no link has been identified between burnout and loneliness.
Objective
To investigate the association of burnout with loneliness and social network degree and centrality.
Methods
A survey containing the Maslach Burnout Inventory (MBI), a 3-question loneliness scale, and a social connectivity component was sent to residents in a large urban academic medical center internal medicine residency program.
Results
The response rate was 77% (95 of 124 residents). We defined significant burnout as MBI subscores of ≥ 27 for emotional exhaustion (EE), ≥ 10 for depersonalization (DP), or both. This was met by 43 (45%), 47 (49%), and 31 (33%) out of 95 respondents, respectively. Those with significant burnout had higher loneliness scores: 5.6 versus 4.5 for EE (P = .002; OR = 1.50; 95% CI 1.15–1.95); 5.4 versus 4.6 for DP (P = .024; OR = 1.33; 95% CI 1.03–1.71); and 5.8 versus 4.6 for both EE and DP (P = .001; OR = 1.54; 95% CI 1.17–2.02). Rating a larger number of coresidents as closer connections on a 5-point Likert scale was not associated with lower burnout scores. No measures of centrality were associated with burnout scores for EE and/or DP. High personal accomplishment subscores on the MBI did correlate significantly with several measures of centrality.
Conclusions
Burnout was associated with loneliness in a dose-dependent fashion. Greater sense of personal accomplishment was associated with greater network centrality.
What was known and gap
Burnout has been studied as an individual phenomenon, but little is known about the effect of loneliness and the presence of social networks.
What is new
A study showed that burnout was associated with loneliness, while a greater sense of personal accomplishment was associated with greater network centrality.
Limitations
Single site, single specialty study reduces generalizability; social network tool lacks established validity evidence.
Bottom line
The study provides a starting point for research on how group and social network factors affect trainee burnout.
Introduction
Burnout syndrome, characterized by emotional exhaustion (EE), depersonalization (DP), and a decreased sense of personal accomplishment (PA), is common within the continuum of medical training and practice.1,2 Burnout is associated with depression; suicidal ideation; lower patient satisfaction; decreased altruism, empathy, and perceived quality of care; and increased unprofessional behavior and self-reported errors.3–9
The majority of internal medicine residents (78%) report symptoms of burnout at least once during residency training, with 23% reporting burnout throughout all 3 years of training.5 In 1 study, 61% of residents reported becoming more cynical, and 23% reported becoming less humanistic during training.10
While burnout often is considered an individual affliction, ties between individuals create social networks and allow individuals to influence each other.11,12 The literature on social networks has demonstrated the spread of emotions, such as happiness and loneliness, as well as the spread of negative afflictions, such as smoking and obesity.11
Residency programs represent unique social networks, and we sought to investigate the relationship between burnout and loneliness. We hypothesized that residents with greater loneliness would have greater burnout, and that residents who are more central within their social network have less burnout.
Methods
Setting and Participants
We piloted our study of loneliness and burnout in a single internal medicine residency program as a proof of concept prior to conducting a larger study. Categorical internal medicine (IM-C), preliminary year internal medicine (IM-P), and internal medicine-pediatrics (MP) residents from a program set in an urban academic medical center were included. The latter 2 groups had large parts of their training embedded in the internal medicine residency.
Data Collection and Instruments
Data collection was anonymous and included demographics, burnout, loneliness, and social connectivity data. REDCap was used as the survey platform and was collected at a single point in time (December 2013).13 The survey collected data on residents' sex, relationship status, program type, and year in training. Residents completed the Maslach Burnout Inventory (MBI), which is the most common questionnaire used to measure burnout. The MBI consists of 22 questions covering the domains of EE, DP, and PA. Answers fall on a Likert scale from 0 (never) to 6 (every day). In accordance with prior definitions of burnout in medicine, EE scores ≥ 27 and/or DP scores ≥ 10 are considered “significant” burnout. Low PA scores (≤ 33) have a worse correlation with negative consequences of burnout. The MBI has well-established discriminant and convergent validity, and 3-factor analysis has shown it to be invariant among different groups, including residents.14 Cronbach α ratings for the MBI are 0.9 for EE, 0.76 for DP, and 0.76 for PA.1
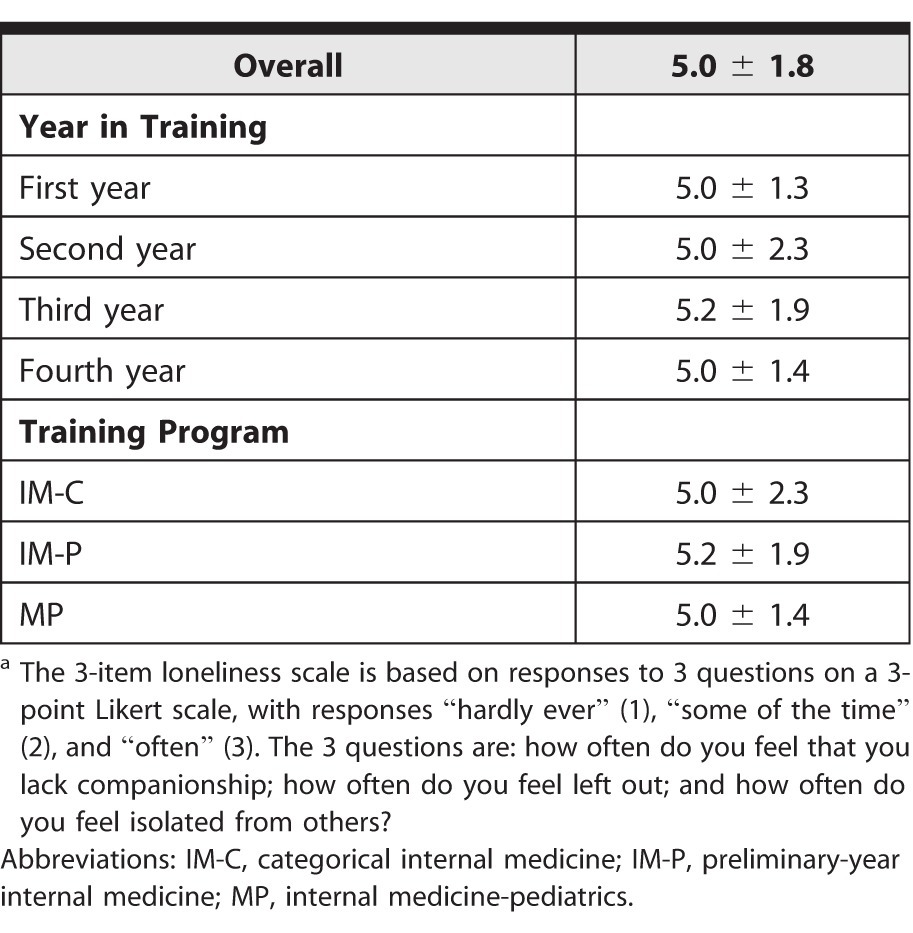
We used a 3-item loneliness scale developed by Hughes et al.15 The scale uses a Likert scale from 1 (hardly ever) to 3 (often). The short scale has demonstrated convergent and discriminant validity, a 0.82 (high positive) correlation with the much longer 20-item revised UCLA Loneliness Scale,16,17 and a Cronbach α of 0.72, demonstrating reliability.17
The loneliness scales measure a lack of perceived connection to others, but this may be influenced by those outside the workplace. In an effort to explore the role of residency programs as social networks, we had residents rate their connectivity to all other residents and used these data to generate 2 categories of social network outcomes: degree (number of connections) and centrality (location and/or role within the network).18–21 No validity evidence was available for the rating scale we used for social connectivity.
The study was approved by the University of Cincinnati Medical Center/Cincinnati Children's Hospital Medical Center Institutional Review Board.
Outcomes
The primary outcome was the relationship between burnout and loneliness. Additional outcomes included the relationships between burnout and social network degree and centrality.
Analysis
Two-sample t tests were used to assess differences between burnout and loneliness. Logistic regression was used to assess differences between burnout and social connection. Chi-square tests were used to assess differences between burnout and sex and between burnout and marital status.
The UCINET Social Network Analysis software was used to derive degree and centrality measures, which are detailed in figure 1. These measures were then used to assess their association with burnout.
FIGURE 1.

Description of Loneliness and Social Network Aspect of the Study
Results
Response Rates
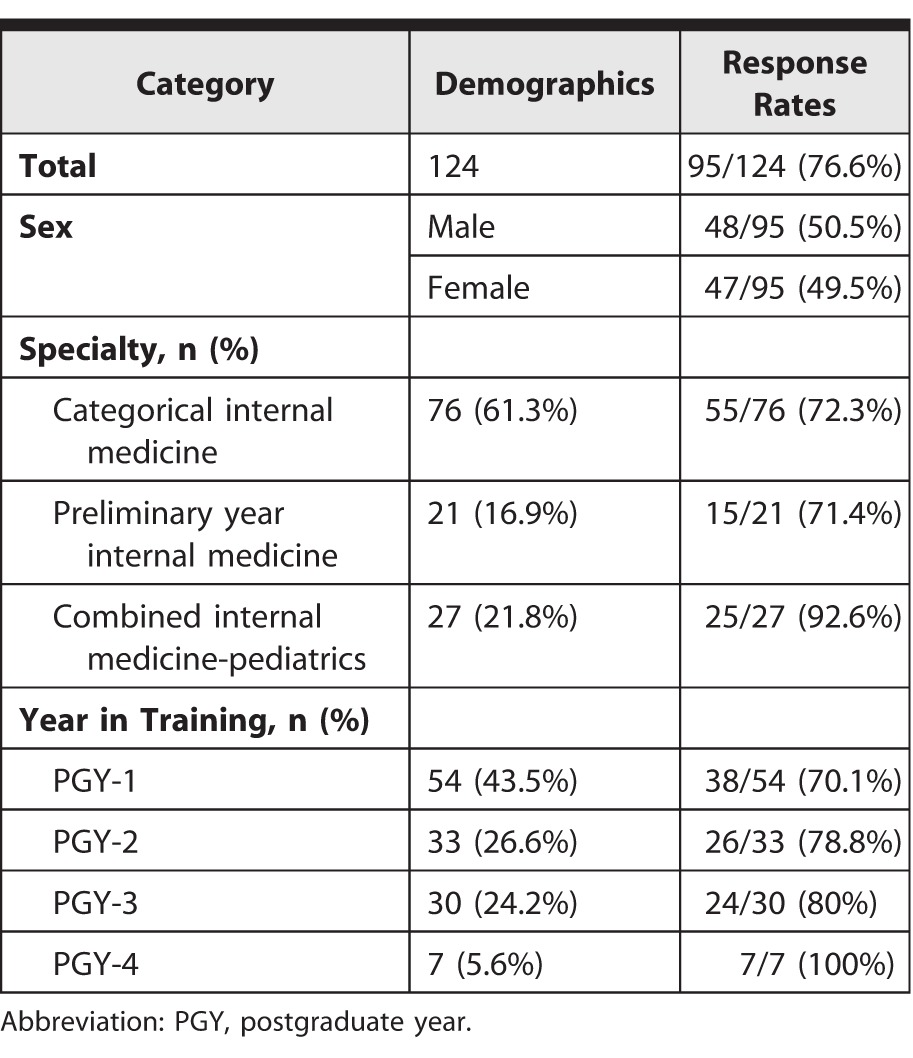
A total of 95 of 124 residents (77%) responded, with additional demographic data for respondents shown in table 1.
TABLE 1.
Resident Demographics and Response Rates
Burnout
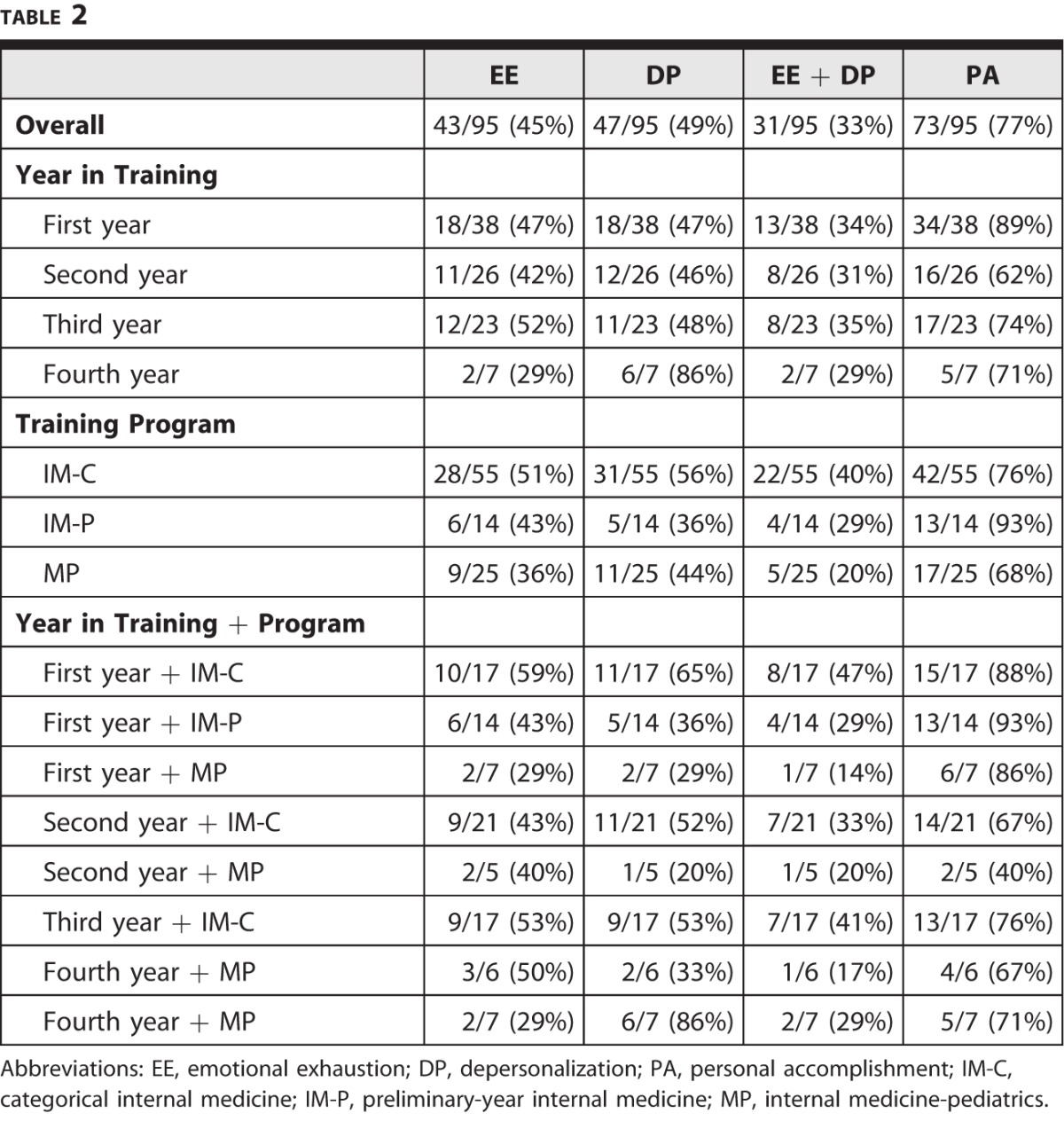
Of 95 residents, 43 (45%) met criteria for burnout by emotional exhaustion (EE) scores, 47 (49%) met burnout criteria by depersonalization (DP) scores, and 31 (33%) met burnout criteria by both EE and DP scores. Rates of burnout by year in training, type of program, and both are shown in table 2.
TABLE 2.
Burnout
Loneliness
Loneliness was greatest in IM-P residents and third-year IM-C residents (table 3).
TABLE 3.
Lonelinessa
Loneliness and Burnout and Loneliness
Residents with significant burnout by EE scores, DP scores, or both rated themselves as more lonely (EE: 5.6 versus 4.5; P = .002; OR = 1.50; 95% CI 1.15–1.95; DP: 5.4 versus 4.6; P = .024; OR = 1.33; 95% CI 1.03–1.71; and EE and DP: 5.8 versus 4.6; P = .001; OR = 1.54; 95% CI 1.17–2.02). However, personal accomplishment (PA) scores ≤ 33 were not associated with loneliness. Adjusting for year of training or program, no association was found between burnout and loneliness (figure 2).
FIGURE 2.
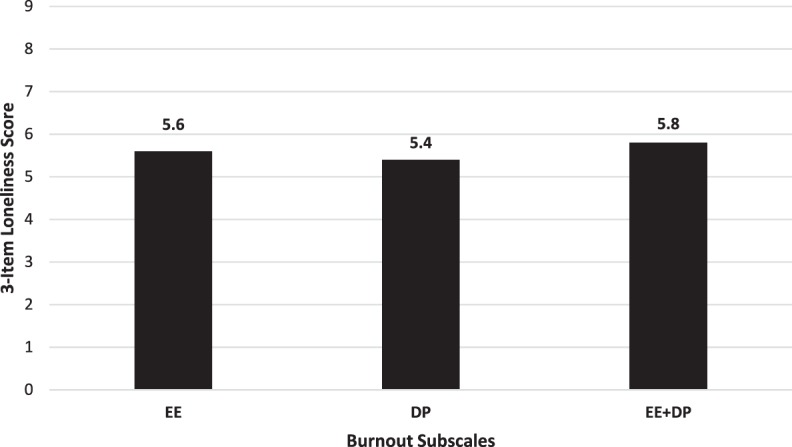
Loneliness by Burnout Subscale
Abbreviations: EE, emotional exhaustion; DP, depersonalization.
Burnout and Social Network
Scores of 3 and 4
On a scale of 0 to 4, ratings of 3 (“have had many conversations”) and 4 (“would go to for support”) were considered strong connections. Logistic regression showed that the total number of scores of 3 and 4 in residents' social network did not significantly correlate with burnout as measured by EE, DP, or both (P = .77, P = .83, and P = .24, respectively). Subjects rating more coresidents as 3s and 4s in their social networks had higher PA scores (P = .024).
Scores of 4
Using only the number of coresidents who rated 4s as a predictor of burnout, logistic regression showed no significant association with EE, DP, EE and DP, or PA (P = .48, P = .88, P = .67, and P = .06, respectively). After adjusting for year in training or program, no relationship was found between burnout and number of scores of 3 + 4 or 4.
In the social network portion of the study, 47 of 95 respondents (49%) left some blanks. We treated blanks as 0s.
Measures of Degree and Centrality
The UCINET Social Network Analysis software was used to generate measures of degree and centrality: In Degree, Out Degree, Closeness Centrality, Eigenvector Centrality, and Clustering Coefficient (figure 1).
None of the measures of degree or centrality were associated with burnout as defined by EE and/or DP scores. However, subjects with high PA scores had significantly higher In Degree, Out Degree, Closeness Centrality, and Eigenvector Centrality measures (P = .027, P = .001, P = .002, and P = .001, respectively). Betweenness Centrality and Clustering Coefficient measures were not associated with PA score (P = .13 and P = .30, respectively).
When adjusted for by training year or program, no relationship was found between burnout and any of the measures of degree or centrality.
Burnout and Sex
Use of chi-square testing showed that male residents had greater DP rates (60.4% versus 39.1%, P = .039). No other significant differences in rates of burnout scores between men and women were noted with P values of .67 for EE, .34 for EE and DP, and .43 for PA.
Burnout and Marital Status
Chi-square tests showed no significant association between burnout and marital status, with P values of .52, .57, .52, and .24 for EE, DP, EE and DP, and PA, respectively.
Discussion
Our study is the first to demonstrate a relationship between loneliness and burnout. Those with greater burnout—meeting burnout criteria by both EE and DP—had higher loneliness scores. There was no significant relationship between social network measures of degree or centrality and EE and/or DP scores. However, high PA scores were associated with several social network measures, including In Degree, Out Degree, Closeness Centrality, and Eigenvector Centrality.
No other studies that have explored the relationships between burnout, loneliness, and social network degree and centrality were available for comparison. However, Vaughan et al22 found greater social capital—in the form of more interactions with problem-based learning group peers and having seniors in a wider academic support network—associated with better academic achievement.
The association of a greater sense of personal accomplishment and several social network measures may reflect residents moving to more central roles within the network as their experience and confidence grow. It may also reflect the challenges of connecting with other residents in the context of work hour restrictions, less time spent by attending physicians on inpatient services, and reduced likelihood of rotating with the same coresidents long enough to form meaningful connections. Therefore, residents may gain a sense of personal accomplishment when they are able to navigate the aforementioned obstacles in order to feel connected to others.
By program, the IM-C residents reported the highest level of burnout, despite being the core of the residency program. Fourth-year MP residents reported the greatest DP, perhaps as this group remains in training an additional year beyond their colleagues in categorical MP programs. Interestingly, fourth-year MP residents had the lowest EE of any group, which could be attributed to a greater sense of comfort with the daily tasks of residency. However, the PA scores for fourth-year MP residents were lower than those for second-year IM-C residents, which may point to an alternative explanation.
The IM-P residents, who were only part of the program for 1 year, had the lowest sense of personal accomplishment. We assumed that more first-year versus fourth-year residents would report a low sense of personal accomplishment, which did hold true. However, we have no explanation for why the second-year residents in our study had the greatest sense of personal accomplishment overall.
Most studies of burnout in trainees are led by faculty. Having a trainee colleague involved may have helped with response rates, especially considering that the principal investigator was a MP resident, and 25 of 27 (93%) of these residents responded to the survey. At the same time, our study has several limitations. First, the cross-sectional survey study was performed at a single point in time, and both factors reduce generalizability. Recent research has pointed to increased rates of burnout from the start of residency that persist into subsequent years.23 Our survey was completed during the middle of the year and may have resulted in higher burnout scores than if we had measured burnout at other points during the year. Second, despite a high response rate at 77%, our findings could have been different had we reached everyone in the network. Third, no validity evidence was available for our connectivity scale, and we chose the cutoffs that were thought to constitute significant connection. Choosing different ranges may have resulted in differing interpretations of results.
Conclusion
We found residents with significant burnout to have higher rates of loneliness in a dose-dependent fashion. In addition, residents with a higher sense of personal accomplishment also had greater centrality within the residency. As few interventions at the level of the individual have been shown to be effective in preventing or mitigating burnout, more exploration of the effects of group-level interventions is needed. Our study is a starting point for future research to assess the effect of group and social networks on trainee burnout.
Footnotes
At the time of writing, Jordan Shapiro, MD, was a Resident, Internal Medicine & Pediatrics, University of Cincinnati Medical Center and Cincinnati Children's Hospital Medical Center, and is now Assistant Professor of Internal Medicine, Division of General Medicine, Section of Hospital Medicine; Bin Zhang, PhD, is Assistant Professor of Statistics, Division of Biostatistics and Epidemiology, Cincinnati Children's Hospital Medical Center; and Eric J. Warm, MD, is Richard W. and Sue P. Vilter Professor of Medicine and Director of Internal Medicine Training Program, University of Cincinnati Medical Center.
Funding: Statistical support was provided by the National Center for Advancing Translational Sciences of the National Institutes of Health, under Award Number UL1TR000077.
Conflict of interest: The authors declare they have no competing interests.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
- 1.Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory Manual. 3rd ed. Palo Alto, CA: Consulting Psychologists Press;; 1998. [Google Scholar]
- 2.Ishak WW, Lederer S, Mandili C, Nikravesh R, Seligman L, Vasa M, et al. Burnout during residency training: a literature review. J Grad Med Educ. 2009;1(2):236–242. doi: 10.4300/JGME-D-09-00054.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dyrbye LN, Massie FS, Jr, Eacker A, Harper W, Power D, Durning SJ, et al. Relationship between burnout and professional conduct and attitudes among US medical students. JAMA. 2010;304(11):1173–1180. doi: 10.1001/jama.2010.1318. [DOI] [PubMed] [Google Scholar]
- 4.Brazeau CM, Schroeder R, Rovi S, Boyd L. Relationships between medical student burnout, empathy, and professionalism climate. Acad Med. 2010;85(suppl 10):33–36. doi: 10.1097/ACM.0b013e3181ed4c47. [DOI] [PubMed] [Google Scholar]
- 5.Campbell J, Prochazka AV, Yamashita T, Gopal R. Predictors of persistent burnout in internal medicine residents: a prospective cohort study. Acad Med. 2010;85(10):1630–1634. doi: 10.1097/ACM.0b013e3181f0c4e7. [DOI] [PubMed] [Google Scholar]
- 6.Dyrbye LN, Thomas MR, Massie FS, Power DV, Eacker A, Harper W, et al. Burnout and suicidal ideation among US medical students. Ann Intern Med. 2008;149(5):334–341. doi: 10.7326/0003-4819-149-5-200809020-00008. [DOI] [PubMed] [Google Scholar]
- 7.Halbesleben JR, Rathert C. Linking physician burnout and patient outcomes: exploring the dyadic relationship between physicians and patients. Health Care Manage Rev. 2008;33(1):29–39. doi: 10.1097/01.HMR.0000304493.87898.72. [DOI] [PubMed] [Google Scholar]
- 8.Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136(5):358–367. doi: 10.7326/0003-4819-136-5-200203050-00008. [DOI] [PubMed] [Google Scholar]
- 9.Fahrenkopf AM, Sectish TC, Barger LK, Sharek PJ, Lewin D, Chiang VW, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336(7642):488–491. doi: 10.1136/bmj.39469.763218.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Collier VU, McCue JD, Markus A, Smith L. Stress in medical residency: status quo after a decade of reform? Ann Intern Med. 2002;136(5):384–390. doi: 10.7326/0003-4819-136-5-200203050-00011. [DOI] [PubMed] [Google Scholar]
- 11.Christakis NA, Fowler JH. Social contagion theory: examining dynamic social networks and human behavior. Stat Med. 2013;32(4):556–577. doi: 10.1002/sim.5408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cacioppo JT, Fowler JH, Christakis NA. Alone in the crowd: the structure and spread of loneliness in a large social network. J Pers Soc Psychol. 2009;97(6):977–991. doi: 10.1037/a0016076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rafferty JP, Lemkau JP, Purdy RR, Rudisill JR. Validity of the Maslach Burnout Inventory for family practice physicians. J Clin Psychol. 1986;42(3):488–492. doi: 10.1002/1097-4679(198605)42:3<488::aid-jclp2270420315>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 15.Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26(6):655–672. doi: 10.1177/0164027504268574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Russell D, Peplau LA, Cutrona CE. The revised UCLA Loneliness Scale: concurrent and discriminant validity evidence. J Pers Soc Psychol. 1980;39(3):472–480. doi: 10.1037//0022-3514.39.3.472. [DOI] [PubMed] [Google Scholar]
- 17.Russell DW. UCLA Loneliness Scale (version 3): reliability, validity, and factor structure. J Pers Assess. 1996;66(1):20–40. doi: 10.1207/s15327752jpa6601_2. [DOI] [PubMed] [Google Scholar]
- 18.Hanneman RA, Riddle M. Chapter 10: centrality and power. Introduction to Social Network Methods. 2015 In. http://faculty.ucr.edu/~hanneman/nettext/C10_Centrality.html. Accessed July 9. [Google Scholar]
- 19.Wasserman S. Social Network Analysis: Methods and Applications. 183–184. Cambridge, UK: Cambridge University Press; 1994. pp. 125–128.pp. 188–190. [Google Scholar]
- 20.Abraham A, Hassanien A, Snášel V. Computational Social Network Analysis: Trends, Tools, and Research Advances. London, UK: Springer;; 2010. pp. 101–103. eds. [Google Scholar]
- 21.Morselli C. Inside Criminal Networks. New York, NY: Springer;; 2009. pp. 40–44. [Google Scholar]
- 22.Vaughan S, Sanders T, Crossley N, O'Neill P, Wass V. Bridging the gap: the roles of social capital and ethnicity in medical student achievement. Med Educ. 2015;49(1):114–123. doi: 10.1111/medu.12597. [DOI] [PubMed] [Google Scholar]
- 23.Pantaleoni JL, Augustine EM, Sourkes BM, Bachrach LK. Burnout in pediatric residents over a 2-year period: a longitudinal study. Acad Pediatr. 2014;14(2):167–172. doi: 10.1016/j.acap.2013.12.001. [DOI] [PubMed] [Google Scholar]