

Abstract
Background and Aims:
Propofol, the most commonly used intravenous (IV) anesthetic agent is associated with hypotension on induction of anesthesia. Different methods have been used to prevent hypotension but with variable results. The objective of this study was to evaluate efficacy of equipotent doses of phenylpehrine and ephedrine in preventing the hypotensive response to the induction dose of propofol.
Material and Methods:
One hundred thirty five adult patients were randomised to one of the study groups: propofol-saline (PS), propofol-phenylephrine (PP) or propofol-ephedrine (PE) by adding study drugs to propofol. Anesthesia was induced with a mixture of propofol and the study drug. Patients were manually mask-ventilated for 5 min using 40% oxygen in nitrous oxide and isoflurane at 1%. A baseline mean arterial pressure (MAP) was recorded prior to induction of anesthesia. Systolic, diastolic and mean blood pressure and heart rate were recorded every minute for up to 5 min after induction. Hypotension was defined as a 20% decrease from the baseline MAP.
Results:
There were no significant demographic differences between the groups. Overall incidence of hypotension in this study was 38.5% (52/135). Rate of hypotension was significantly higher in group PS than group PP (60% vs. 24.4% P = 0.001) and group PE (60% vs. 31.1% P = 0.005). In contrast, a significant difference in rate of hypotension was not observed between groups PP and group PE.
Conclusion:
In equipotent doses, phenylephrine is as good as ephedrine in preventing the hypotensive response to an induction dose of propofol.
Keywords: Ephedrine, hypotension, induction, phenylephrine, propofol
Introduction
Propofol is one of the most commonly used intravenous (IV) induction agent. It has many benefits over other IV induction agents, but it is associated with hypotension on induction of anesthesia.[1,2] Different methods have been employed with variable results to counter the hypotensive effects of propofol including slow drug administration,[3] preloading with IV fluids,[4,5] co-administration of ephedrine,[5,6,7] phenylephrine,[8] ketamine[9] etc.
Phenylephrine is a synthetic noncatecholamine that principally stimulates alpha-1 adrenergic receptors directly.[10] Ephedrine is a mixed-acting sympathomimetic drug that stimulates both alpha and beta adrenergic receptors.[10] Both these drugs are compatible in solution with propofol.[11]
A thorough search of literature could not reveal any comparative study of these two drugs in equipotent doses during general anesthesia.
The objective of this study was to comparatively evaluate the efficacy of ephedrine versus phenylephrine in preventing propofol induced hypotension during induction of anesthesia.
Material and Methods
This randomized, double blind study was conducted between September 03, 2009 and September 09, 2010. After approval from Ethical Review Committee of the hospital (1059-ANE/ERC-08), 135 American Society of Anesthesiologists (ASA) I-II patients of either sex, aged between 18 and 60 years, undergoing elective surgery requiring general anesthesia, were included in the study. Patients scheduled for emergency surgery, patients with known hypertension, thyroid disease, peripheral vascular disease, ischemic heart disease, cardiac arrhythmias or having cardiac pace maker, patients taking any heart rate modifying drugs, monoamine oxidase inhibitors, or drugs affecting autonomic nervous system and patients allergic to any of the study drugs were excluded from the study. After obtaining written informed consent, patients meeting the inclusion criteria were randomized and allocated to one of the three study groups by using sealed opaque envelope method.
· Group propofol-saline (PS): 2 ml. 0.9% sodium chloride as placebo control.
· Group propofol-phenylephrine (PP): 2 ml (50 mcg/ml) phenylephrine.
· Group propofol-ephedrine (PE): 2 ml (4 mg/ml) of ephedrine.
For purpose of comparison we calculated the equipotent doses of phenylephrine and ephedrine from the study of Saravanan et al.[12] that demonstrated a relative potency ratio for phenylephrine: ephedrine of 80:1 (100 mcg: 8 mg).[12] Study drug was prepared by drawing 20 ml propofol (1%) and 2 ml lignocaine (2%) in 25 ml syringe. The study drug was added to this mixture according to the study group mentioned above to make a total volume of 24 ml (containing 8.33 mg/ml propofol). All the study drugs were prepared by an anesthesiologist who was not involved in data collection and analysis. All patients were premedicated with oral midazolam 7.5 mg 1 h before the operation. In the operating room, standard monitoring (pulse oximetry, noninvasive blood pressure, and electrocardigram) was instituted. Baseline SBP, DBP, MAP and heart rate were taken from an average of two readings taken 5 min apart by the primary investigator. After securing IV access, all patients were preoxygenated with 100% oxygen for 3 min using circle circuit. Anesthesia was induced by using mixture of propofol, lignocaine and study drug, according to assigned group, over 1 min through an IV infusion pump (Graseby syringe pump 3400) by the primary investigator, who was blinded to the study drug. After administering the calculated induction dose (2 mg/kg) of propofol, if needed an additional one ml of the same mixture was given every 10 s until hypnosis was achieved as assessed by loss of verbal response from the patient. Any patient requiring more than three propofol increments was planned to be excluded from the study but none of our patients required more than three propofol increments. All the patients were ventilated with a bag valve mask for 5 min using 40% oxygen in nitrous oxide and isoflurane at 1%. SBP, DBP and mean blood pressure and heart rate readings were recorded every minute for upto 5 min after induction. At this point, the study was terminated, and rest of the anesthesia technique was left at the discretion of primary anesthetist. Hypotension was defined as a 20% decrease from the baseline MAP. Hypotension requiring treatment was defined as a decrease in MAP to 60 mmHg or less. In case of a decrease in MAP to 60 mmHg or less, 200 ml bolus of normal saline was infused over 2 min followed immediately by another 200 ml bolus if needed (to a maximum of 400 ml). If this failed to raise the blood pressure to >60 mmHg, incremental doses of either phenylephrine 100 mcg (if heart rate was >60 beats/min) or ephedrine 8 mg (if heart rate was <60 beats/min) were given. Isolated bradycardia (heart rate <50/min) without associated hypotension, was treated with injection atropine 0.5 mg intravenously.
The number of patients required in each group was determined by using power analysis based on the previous study.[8] The sample size required detecting 20% reduction in MAP from baseline at 5% level of significance and 80% power was 45 patients in each group. Data was entered and analyzed in statistical software Statistical Package for Social Sciences (SPSS) version 19.0, (SPSS Inc., Chicago, IL). Frequencies and percentage were computed for gender, ASA level and hypotension among the groups and analyzed by Chi-square test. Means and standard deviations were estimated for age, weight, height, body mass index and for hemodynamic response like SBP and DBP, MAP, heart rate and analyzed by analysis of variance with Post-hoc multiple comparison test after normality assumptions by Kolmogorov–Smirnov and Shapiro–Wilk test. Chi-square test was used to compare proportion difference for prevention of hypotensive response among groups. P < 0.05 was considered statistically significant.
Results
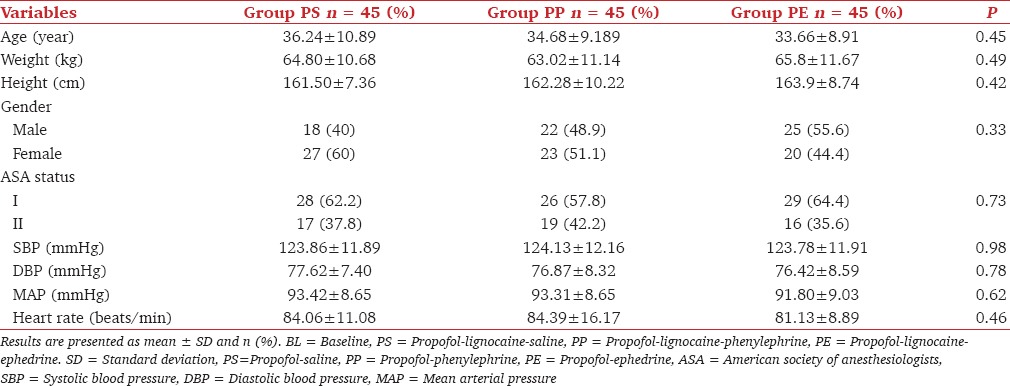
A total of 135 patients scheduled for elective surgical procedure under general anesthesia were included in this study, and all of them completed the study. Demographic data and baseline variables are given in Table 1. No significant differences were observed in age, weight, height, gender, ASA level, baseline heart rate, SBP, DBP and mean blood pressure.
Table 1.
Comparison of demographic and BL data among groups
Mean hemodynamic responses of groups PP and PE (study groups) were compared with group PS (control group) and compared with each other to see significant differences. Hypotension was also compared among the groups. Overall incidence of hypotension in this study was 38.5% (52/135).
Systolic blood pressure at each minute was compared among control group (group PS) and both study groups (groups PP and PE). A statistically significant difference was found in groups PP and PE from min 1 to 5 as compared to control group [Figure 1]. Similarly the difference in DBP at each minute was statistically significant from min 1 to 5 in group PP as compared to control the group. In group PE, DBP was found to be significantly different from min 2 to 5 as compared to control the group [Figure 2]. The MAP in groups PP and PE was significantly different at all times in comparison with group PS [Figure 3].
Figure 1.
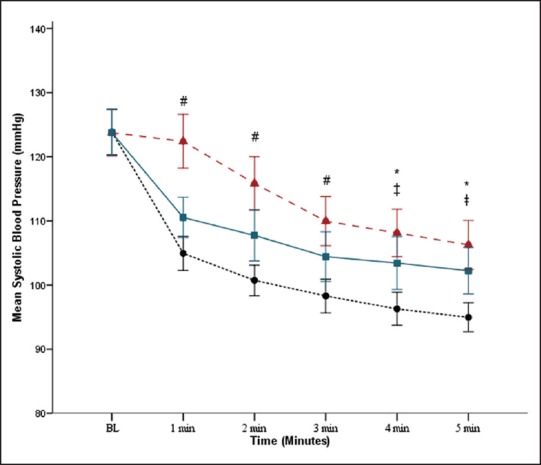
Comparison of mean systolic blood pressure with respect to time among propofol-saline (PS), (•), propofol-phenylephrine (PP), (Δ) and propofolephedrine (PE), (◾). *P < 0.05 PS versus PP; ‡P < 0.05 PS versus PE; #P < 0.05 all multiple groups comparison significant
Figure 2.
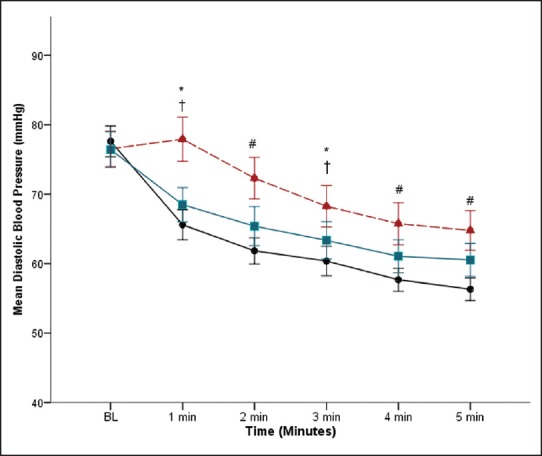
Comparison of mean diastolic blood pressure with respect to time among propofol-saline (PS), (•), propofol-phenylephrine (PP), (Δ) and propofolephedrine (PE), (◾). *P < 0.05 PS versus PP; †P < 0.05 PP versus PE; #P < 0.05 all multiple groups comparison significant
Figure 3.
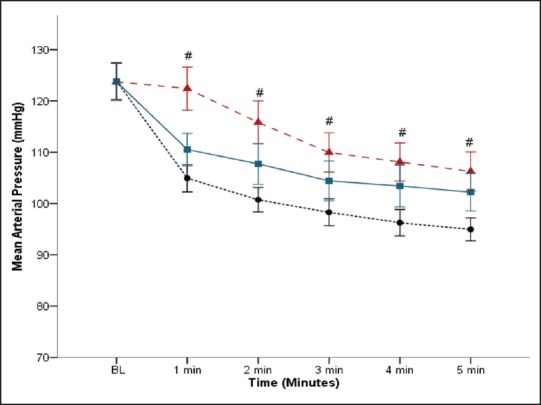
Comparison of mean arterial pressure with respect to time among propofol-saline, (•), propofol-phenylephrine, (Δ) and propofol-ephedrine, (◾). #P < 0.05 all multiple groups comparison significant
The change in heart rate was significant in Group PP in 1st and 2nd min as compared to control the group. Group PE did not show any significant difference in heart rate in comparison with the control group. Results demonstrated decrease in heart rate in patients who received the phenylephrine [Figure 4].
Figure 4.
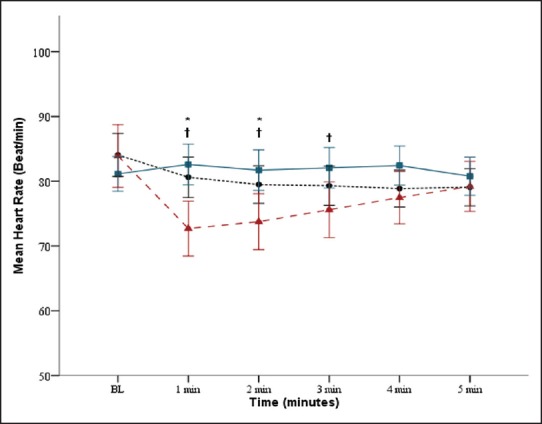
Comparison of mean heart rate with respect to time among propofolsaline (PS), (•), propofol-phenylephrine (PP), (Δ) and propofol-ephedrine (PE), (◾). *P < 0.05 PS versus PP; †P < 0.05 PP versus PE
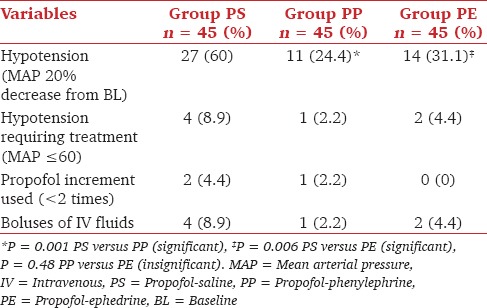
Table 2 shows the rate of hypotension that was significantly higher in group PS than group PP (60% vs. 24.4% P = 0.001). Similarly, this difference was also significant in groups PS and PE (60% vs. 31.1% P = 0.006).
Table 2.
Comparison of hypotension among groups
In comparison of groups PP and PE, SBP values were significantly different from min 1 to 3 [Figure 1]. In contrast DBP values were significant for a longer period, that is, from 1st to 5th min [Figure 2]. The MAP also came to be significantly different from min 1 to 5 [Figure 3]. These values show better control of SBP, DBP and MAP in group PP than group PE.
Difference in heart rate was only significant from 1st to 3rd min. Heart rate was found to be decreased from the baseline in group PP than group PE [Figure 4].
When the rate of hypotension was compared between groups PP and PE, significant difference was not observed as shown in Table 2 (24.4% vs. 31.1% P = 0.48).
Four patients in group PS, two patients in group PE and one patient in group PP required IV normal saline for treatment of hypotension and they responded adequately. None of the patient required ephedrine, phenylephrine or atropine for treatment of hypotension or bradycardia.
Discussion
Hypotension following induction of anesthesia using propofol is caused by propofol-mediated decrease in sympathetic activity including decrease in systemic vascular resistance[1] and decrease in cardiac output by a combination of venous and arterial vasodilation,[1,14] impaired baroreflex mechanism and depression of myocardial contractility.[15] Independent of the presence of cardiovascular disease, the incidence of this propofol-mediated hypotension ranges from 25% to 67.5%.[1,9,16]
Our study revealed a higher incidence of hypotension (60% in Group PS). Since we used a standard (fixed) dose of propofol, our population may have experienced more vasodilatation as compared to other populations.
Our study demonstrated a significant reduction in the incidence of propofol induced hypotension with simultaneous administration of phenylephrine or ephedrine mixed with propofol. However, hypotension was still present in 24.4% and 31.1% of patients respectively.
Our findings are consistent with the findings of Imran et al. who have shown a dose related (50 mcg vs. 100 mcg) incidence of hypotension (56% vs. 20%) when phenylephrine was combined with propofol[8]
Dhungana et al. in their study compared preloading with haemaccel (colloid fluid) and ephedrine for prevention of hypotension during propofol induction. They found that only 22.5% patients developed hypotension when ephedrine (0.2 mg/kg, mean dose 10 mg) was used compared with 23.1% in colloid group and 67.5% in control group.[5] In our study slightly more (31.1%) patients in the ephedrine group became hypotensive which can be attributed to a relatively lower dose of ephedrine (8 mg) used in our study.
Michelsen et al. observed an attenuation of hypotension, associated with propofol induction with the use of a prophylactic ephedrine. They used ephedrine in the dose of 0.1 mg/kg and 0.2 mg/kg IV 1 min before induction of anesthesia with propofol and fentanyl.[7] Gamlin et al. observed effective obtundation of hypotension accompanied with tachycardia as higher doses of ephedrine (15, 20 and 25 mg) was used in their study.
We did not observe a statistically significant increase in the heart rates in patients receiving ephedrine in our study. However we found statistically significant decrease in heart rates in patients receiving phenylephrine in the 1st and 2nd min after induction of anesthesia. Propofol alters the baroreflex mechanism, resulting in a smaller increase in heart rate for a given decrease in arterial pressure.[18] Recent studies suggest that induction of anesthesia with propofol attenuates desflurane-mediated sympathetic activation.[19] This fact probably further contributed to the significant decrease in heart rate in patients who received phenylephrine (group PP). Ephedrine seems to counteract and compensate for the decrease in heart rate associated with administration of propofol, and the heart rate remained stable at baseline in patients who received ephedrine.
We found that both phenylephrine and ephedrine effectively maintained a significantly higher level of MAP than the control group. However, neither of these two drugs completely prevented the hypotensive response.
Conclusion
In equipotent doses, phenylephrine is as good as ephedrine in preventing the hypotensive response to an induction dose of propofol.
Footnotes
Source of Support: Nil
Conflicts of Interest: None declared.
References
- 1.Claeys MA, Gepts E, Camu F. Haemodynamic changes during anaesthesia induced and maintained with propofol. Br J Anaesth. 1988;60:3–9. doi: 10.1093/bja/60.1.3. [DOI] [PubMed] [Google Scholar]
- 2.Fairfield JE, Dritsas A, Beale RJ. Haemodynamic effects of propofol: Induction with 2.5 mg kg-1. Br J Anaesth. 1991;67:618–20. doi: 10.1093/bja/67.5.618. [DOI] [PubMed] [Google Scholar]
- 3.Aitkenhead AR. Intravenous anaesthetic agents. In: Aitkenhead AR, Smith G, Rowbotham DJ, editors. Textbook of Anaesthesia. Philadelphia: Churchill Livingstone; 2007. pp. 34–51. [Google Scholar]
- 4.Turner RJ, Gatt SP, Kam PC, Ramzan I, Daley M. Administration of a crystalloid fluid preload does not prevent the decrease in arterial blood pressure after induction of anaesthesia with propofol and fentanyl. Br J Anaesth. 1998;80:737–41. doi: 10.1093/bja/80.6.737. [DOI] [PubMed] [Google Scholar]
- 5.Dhungana Y, Bhattarai BK, Bhadani UK, Biswas BK, Tripathi M. Prevention of hypotension during propofol induction: A comparison of preloading with 3.5% polymers of degraded gelatin (Haemaccel) and intravenous ephedrine. Nepal Med Coll J. 2008;10:16–9. [PubMed] [Google Scholar]
- 6.Rasooli S, Parish M, Mahmoodpoor A, Moslemi F, Sanaie S, Faghfuri S. The effect of intramuscular ephedrine in prevention of hypotension due to propofol. Pak J Med Sci. 2007;23:893. [Google Scholar]
- 7.Michelsen I, Helbo-Hansen HS, Køhler F, Lorenzen AG, Rydlund E, Bentzon MW. Prophylactic ephedrine attenuates the hemodynamic response to propofol in elderly female patients. Anesth Analg. 1998;86:477–81. doi: 10.1097/00000539-199803000-00004. [DOI] [PubMed] [Google Scholar]
- 8.Imran M, Khan FH, Khan MA. Attenuation of hypotension using phenylephrine during induction of anaesthesia with propofol. J Pak Med Assoc. 2007;57:543–7. [PubMed] [Google Scholar]
- 9.Bano F, Zafar S, Sabbar S, Aftab S, Haider S, Sultan ST. Intravenous ketamine attenuates injection pain and arterial pressure changes during the induction of anesthesia with propofol: A comparison with lidocaine. J Coll Physicians Surg Pak. 2007;17:390–3. [PubMed] [Google Scholar]
- 10.Westfall TC, Westfall DP. Adrenergic agonists and antagonists. In: Brunton LL, Lazo JS, Parker KL, editors. Goodman & Gilman's the Pharmacological Basis of Therapeutics. 11th Edition. United States of America: McGraw-Hill; 2006. pp. 237–95. [Google Scholar]
- 11.Trissel LA, Gilbert DL, Martinez JF. Compatibility of propofol injectable emulsion with selected drugs during simulated Y-site administration. Am J Health Syst Pharm. 1997;54:1287–92. doi: 10.1093/ajhp/54.11.1287. [DOI] [PubMed] [Google Scholar]
- 12.Saravanan S, Kocarev M, Wilson RC, Watkins E, Columb MO, Lyons G. Equivalent dose of ephedrine and phenylephrine in the prevention of post-spinal hypotension in Caesarean section. Br J Anaesth. 2006;96:95–9. doi: 10.1093/bja/aei265. [DOI] [PubMed] [Google Scholar]
- 13.White PF. Clinical pharmacology of intravenous induction drugs. Int Anesthesiol Clin. 1988;26:98–104. doi: 10.1097/00004311-198802620-00003. [DOI] [PubMed] [Google Scholar]
- 14.Robinson BJ, Ebert TJ, O’Brien TJ, Colinco MD, Muzi M. Mechanisms whereby propofol mediates peripheral vasodilation in humans. Sympathoinhibition or direct vascular relaxation? Anesthesiology. 1997;86:64–72. doi: 10.1097/00000542-199701000-00010. [DOI] [PubMed] [Google Scholar]
- 15.Ebert TJ, Muzi M, Berens R, Goff D, Kampine JP. Sympathetic responses to induction of anesthesia in humans with propofol or etomidate. Anesthesiology. 1992;76:725–33. doi: 10.1097/00000542-199205000-00010. [DOI] [PubMed] [Google Scholar]
- 16.Larsen R, Rathgeber J, Bagdahn A, Lange H, Rieke H. Effects of propofol on cardiovascular dynamics and coronary blood flow in geriatric patients. A comparison with etomidate. Anaesthesia. 1988;43(Suppl):25–31. doi: 10.1111/j.1365-2044.1988.tb09064.x. [DOI] [PubMed] [Google Scholar]
- 17.Gamlin F, Freeman J, Winslow L, Berridge J, Vucevic M. The haemodynamic effects of propofol in combination with ephedrine in elderly patients (ASA groups 3 and 4) Anaesth Intensive Care. 1999;27:477–80. doi: 10.1177/0310057X9902700507. [DOI] [PubMed] [Google Scholar]
- 18.Sellgren J, Ejnell H, Elam M, Pontén J, Wallin BG. Sympathetic muscle nerve activity, peripheral blood flows, and baroreceptor reflexes in humans during propofol anesthesia and surgery. Anesthesiology. 1994;80:534–44. doi: 10.1097/00000542-199403000-00009. [DOI] [PubMed] [Google Scholar]
- 19.Lopatka CW, Muzi M, Ebert TJ. Propofol, but not etomidate, reduces desflurane-mediated sympathetic activation in humans. Can J Anaesth. 1999;46:342–7. doi: 10.1007/BF03013225. [DOI] [PubMed] [Google Scholar]