

Abstract
Background and Aims:
Acute postoperative pain is still a neglected and unresolved issue in day to day practice. Acute pain services were conceived three decades ago to form a dedicated team to monitor pain assessment and treatment as per laid down pain protocols and guidelines. The concept of acute pain service (APS) is slowly evolving in India.
Material and Methods:
This nationwide questionnaire survey was conducted to identify the status of postoperative pain, the prevalent treatment practices, and the prevalence of acute pain services in India. An electronic communication was sent to 4000 Indian Society of Anesthesiologists life members.
Results:
We received only 146 responses mainly from faculties/consultants from few corporate hospitals or medical colleges. About 68 APSs were functioning, however, 20 APS do not have any training programs and 34 have no written protocols. Anesthesiologists were involved in postoperative pain management only when epidural analgesia was employed.
Conclusion:
This survey found that majority of anesthesiologists agree to establish an APS, however administrative issues seem to be a major barrier.
Keywords: Acute pain service, pain in India, post-operative pain, questionnaire survey
Introduction
Inadequate pain relief after surgery has been highlighted by many pain surveys in the last decade.[1,2,3] Impact of unrelieved pain leads to deleterious effects on almost all systems of the body resulting in delayed recovery and psychological distress and anxiety. Lately, the concept of acute pain service (APS) is emerging in India. There is some evidence to show that the presence of APS and development of guidelines reduces pain scores and enhance patient satisfaction in the hospital.[4]
APS is defined as a dedicated health care personnel driven service which assesses, monitors and treats pain and side effects of pain medications, on a 24 hour basis. Audits are performed to evaluate the efficacy of pain service. Royal College of Surgeons and College of Anaesthetists working party on pain after surgery[2] recommended that APS should be introduced in all major hospitals performing surgery in the UK. Nearly, all major hospitals in North America, Europe and Australia have vibrant APSs. We proposed to collect realistic data regarding the existence of APS, and to evaluate its quality assurance in India. This attempt also included the prevalent pain practices, hospital opioid policy and attitude of anesthesiologists regarding APS.
Material and Methods
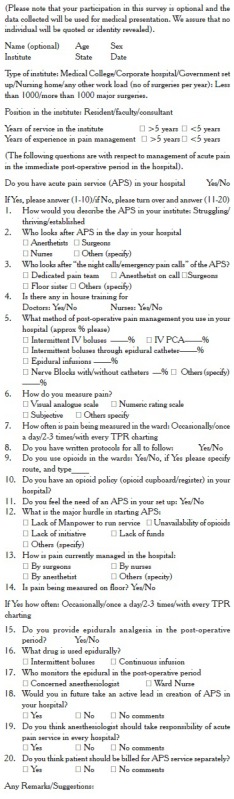
This prospective questionnaire (20 items questions) survey was undertaken (July-November 2011) by sending a four pages electronic proforma by E-mail to 4000 anesthesiologists across India in all states. Around 100 printed proformas were also served at various conferences of anesthesiologists by hand for completion. Whosoever completed the questionnaire (Annexure 1), were considered to have consented to participate in the aforesaid survey. Question nos. 1-10 were related to APS, aimed to elicit details of APSs in their hospital and question nos. 11-20 were to gather information regarding prevalent post-operative pain management practices in their hospital. Data mainly the responses was analyzed as percentages, using IBM SPSS statistics, version 14.0.
Results
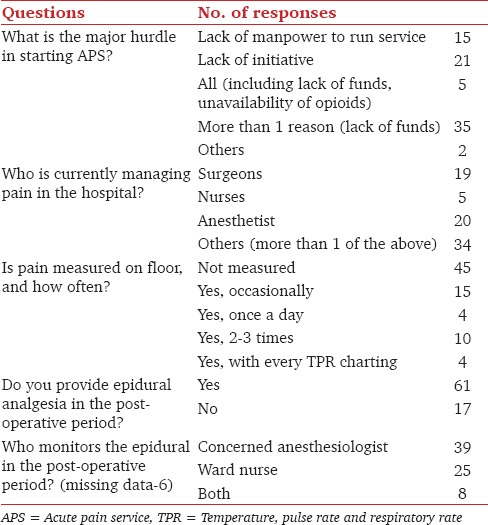
A total of 4000 electronic questionnaires and 100 hard copies were sent and 146 responses were received including 105 electronic submission and 41 hard copies from nearly all states of India. 78% responses were received from the hospitals where more than 1000 surgeries are performed every year, including 48% from medical colleges 26% from corporate hospitals, rest from smaller set ups [Figure 1]. Among the respondents, 65 were anesthesia faculties, 53 consultants, and 24 residents with 56% responders having more than 5 years experience in anesthesiology. Only 47% (68) doctors reported to have an APS. Quality of APS is depicted in Figure 2. Only three hospitals had a dedicated pain team at night also. Forty four (65%) APSs were managed by anesthesiologists, the rest others were managed by surgeons and nurses. Level of pain assessment was also variable. Pain was assessed 2-3 times a day in 26 hospitals and 24 had pain established as a fifth vital sign on the temperature, pulse rate and respiratory rate chart and 10 hospitals measured pain once a day only despite an APS. Pain was assessed by using different pain scales. Visual analog scale was used in 25 hospitals, numerical rating scale in 9 and 15 hospitals assessed pain verbally. An opioid policy was in place in 86% hospitals (opioid cupboard, opioid register) but only 50% APSs used opioids in the wards and followed written protocols [Table 1]. There was no pain education provision in 29% hospitals. Major hurdles in starting an APS were reported as lack of manpower (15/78), or lack of initiative (21/78) or both. Pain was equally managed by anesthesiologists or surgeons with nurses in some hospitals with 58% having no pain measurement. Majority anesthesiologists (78%) managed pain by epidurals, mostly (46%) by intermittent opioid boluses by them or in other 26% hospitals, nurses took care of epidurals. Majority of anesthesiologists (85%) opined that they would take an active role in APS, if the service would start and 97% were ready to take the responsibility [Table 2]. Regarding the cost of APS, 62% suggested in favor of a separate billing for pain services provided.
Figure 1.
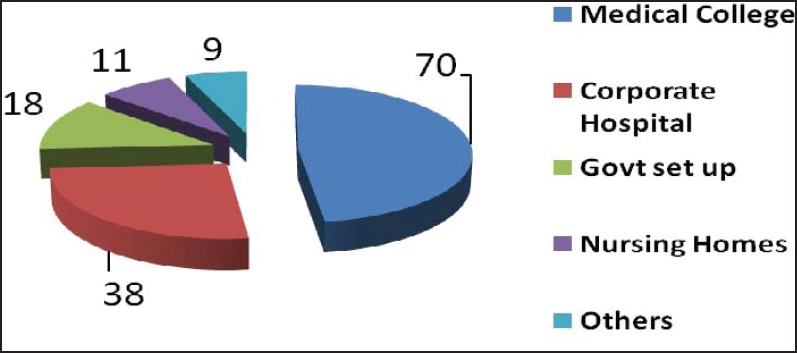
Type of the hospital (n = 146)
Figure 2.
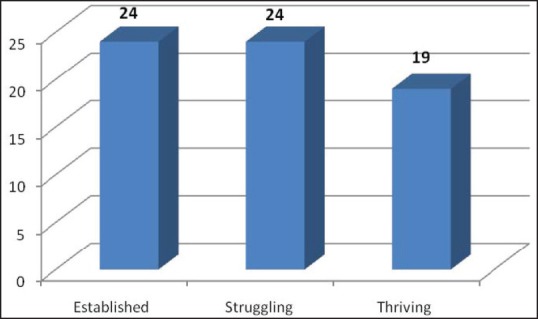
Status of acute pain service (n = 68, missing data-1)
Table 1.
Feedback from centers with APS (n = 68)
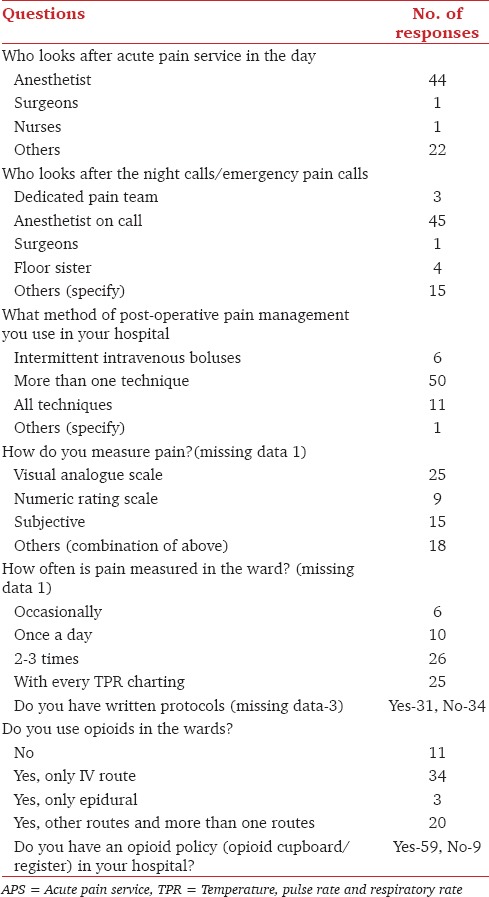
Table 2.
Feedback from centers without APS (n=78)
Discussion
This post-operative pain survey encompassing prevailing pain practices, personnel, drug and protocol related issues shows that the concept of “APS” is slowly emerging in India.
This survey shows that in only 45% hospitals, anesthesiologists were involved in post-operative pain and non-anesthesiologists (55%) like surgeons or nurses were mainly responsible for pain management in the wards. Most of APSs are run in corporate or big teaching hospitals. Except in APS scenarios, pain is not routinely measured or documented in the hospitals. Epidural analgesia is the commonest mode of analgesia used for post-operative pain often with opioid boluses by the concerned OT anesthesiologists. At an optimistic note, majority of the anesthesiologists feel the need of an APS in their hospital as well as wish to take the responsibility to run the service. However, a busy hospital environment, paucity of staff, inappropriate attitude and inadequate knowledge of pain management remain the main barriers for pain management. In many hospitals anesthesiologists are overwhelmed with their responsibilities in the operation theatre with little time to spare for post-operative pain visits.[5]
APS is still not well organized in India, even though the anesthesiologist takes care of post-operative pain relief in major surgical procedures as well as takes care of the surgical ICU.[6]
APSs started in mid 1980s[7,8,9] with an understanding that a dedicated team is required for regular and frequent pain assessment with well-defined goals for pain treatment including written protocols and continual education of the heath care staff. There is evidence to show that establishing APS can improve standard of care, reduce morbidity, hasten hospital discharge and lower health costs apart from improving patients’ satisfaction.
Vijayan[3] conducted a six countries questionnaire survey and reported that, in India, less than 30% patients receive adequate acute pain relief. This study also testifies that only 31 respondents have written protocols, 59 have an opioids policy (opioid cupboard, register) and only 34 use intravenous opioids in wards despite having an APS.
In India, there is no single stakeholder of post-operative pain. Anesthesiologists are managing pain only when epidural or regional analgesia techniques are extended in the post-operative period. Until nurses are trained in post-operative pain management, possibly the critical issue of post-operative pain shall remain unresolved. The first step for successful pain management is assessing and documenting pain as fifth vital sign, which is to be charted on the vital signs chart by the nurses. The scenario is further compounded as patients also do not complain about pain and do not expect a great pain relief after surgery, and usually are fearful of opioid side effects.[10]
Much more disheartening observation is that, pain training is not imparted in 29% of APSs and 50% do not have any written protocols to follow. In 60% of APSs, pain is not measured regularly. Therefore the quality of services provided by APS is also questionable. Despite a firm existence of APSs in UK and internationally, many patients continue to suffer unnecessary pain. In UK, a survey of 14 hospitals[11] report that 60% patients had pain score of 5 or more at 24 hours, with 39% reporting similar pain intensity and 8% severe pain at 7 days after surgery. In another UK survey on pain services,[10] 95% respondents reveal that better organization is needed rather than new drugs and treatment. Indian studies[12,13] on APSs also emphasized that despite an APS in a cancer hospital setting, 60% patients complained of moderate to severe pain. Developed countries have an established APS in place and usually conduct quality assurance studies which are missing in India so comparison was not possible; therefore, a direct comparison of quality assurance was not attempted.
This study has many limitations. The sample size is small to draw a tangible picture about the status of APSs in India. Many recipient of the electronic study questionnaire may have not responded as APS probably does not exist in their places of practice. We expected at least ten percent reply of questionnaires which may have had a better reflection about the status of post-operative pain services in India. A new multi-centric survey may be planned with an electronic submission to receive a larger sample. A new validated questionnaire with a more comprehensive approach be applied ensuring all questions to be completed by all respondents.
Annexure 1: A survey on views on the existence of acute pain service (APS) in India
Footnotes
Source of Support: Nil
Conflicts of Interest: None declared.
References
- 1.Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: Results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97:534–40. doi: 10.1213/01.ANE.0000068822.10113.9E. [DOI] [PubMed] [Google Scholar]
- 2.London: Royal College of Surgeons; 1990. Royal College of Surgeons and College of Anaesthetists Working Party on Pain after Surgery. [Google Scholar]
- 3.Vijayan R. Seattle: IASP Press; 2011. Managing acute pain in developing world. Pain clinical updates. [Google Scholar]
- 4.Kainzwaldner V, Rachinger-Adam B, Mioc-Curic T, Wöhrle T, Hinske LC, Luchting B, et al. Quality of postoperative pain therapy: Evaluation of an established anesthesiology acute pain service. Anaesthesist. 2013;62:453–9. doi: 10.1007/s00101-013-2177-7. [DOI] [PubMed] [Google Scholar]
- 5.Gayatri P. Postoperative pain services. Indian J Anaesth. 2005;49:17–9. [Google Scholar]
- 6.Rao M. Acute postoperative pain. Indian J Anaesth. 2006;50:40–4. [Google Scholar]
- 7.Ready LB, Oden R, Chadwick HS, Benedetti C, Rooke GA, Caplan R, et al. Development of an anesthesiology-based postoperative pain management service. Anesthesiology. 1988;68:100–6. doi: 10.1097/00000542-198801000-00016. [DOI] [PubMed] [Google Scholar]
- 8.Petrakis JK. Acute pain services in a community hospital. Clin J Pain. 1989;5(Suppl 1):S34–41. doi: 10.1097/00002508-198903001-00008. [DOI] [PubMed] [Google Scholar]
- 9.Maier C, Kibbel K, Mercker S, Wulf H. Postoperative pain therapy at general nursing stations. An analysis of eight year's experience at an anesthesiological acute pain service. Anaesthesist. 1994;43:385–97. doi: 10.1007/s001010050071. [DOI] [PubMed] [Google Scholar]
- 10.Powell AE, Davies HT, Bannister J, Macrae WA. Rhetoric and reality on acute pain services in the UK: A national postal questionnaire survey. Br J Anaesth. 2004;92:689–93. doi: 10.1093/bja/aeh130. [DOI] [PubMed] [Google Scholar]
- 11.Moss E, Taverner T, Norton P, Lesser P, Cole P. A survey of postoperative pain management in fourteen hospitals in the UK. Acute Pain. 2005;7:12–20. [Google Scholar]
- 12.Jain PN, Myatra SN, Kakade AC, Sareen R. An evaluation of postoperative analgesia in acute pain service in an Indian cancer hospital (a preliminary experience of patient satisfaction survey) Acute Pain. 2008;10:9–14. [Google Scholar]
- 13.Jain PN, Chatterjee A. Development of acute pain service in an Indian cancer hospital. J Pain Palliat Care Pharmacother. 2010;24:129–35. doi: 10.3109/15360281003713842. [DOI] [PubMed] [Google Scholar]