

Abstract
This study investigated the effects of altering foot placement on the strategies used by able-bodied subjects to perform reaching tasks while standing. The motivation for this study was to consider the results in the context of a person with a spinal cord injury using a functional neuromuscular stimulation (FNS) system to stand while reaching. Three foot placement conditions were compared as subjects reached to the left, right, and center. Centers of pressure (COP), joint angles, and joint moments were calculated as postural parameters using force platform and video marker data. Side-by-side and wide foot placements resulted in similar postural parameters. In contrast, the modified tandem stance (feet spaced at pelvic width with one foot shifted forward) resulted in anterior/posterior COP excursions that were larger in magnitude and more consistent across reach directions when compared to the other foot placement conditions. Furthermore, the movement patterns used during the tandem stance were more consistent and may be more readily achievable with FNS than the movement patterns utilized with the side-by-side and wide stances. These results suggest that the modified tandem stance may enhance the functionality of FNS standing systems and may also be useful in other standing rehabilitation programs.
Keywords: Biomechanics, kinematics, neuromuscular stimulation, posture, spinal-cord injury (SCI)
I. Introduction
THE MOTIVATION for this study was to explore postural adjustments that may be useful for persons with spinal-cord injury (SCI) that utilize functional neuromuscular stimulation (FNS) to stand [1]–[6]. FNS is a technique that uses pulsatile electrical stimulation to activate paralyzed muscles in the lower extremities for the purpose of restoring motor function. In addition to therapeutic benefits that may be derived from standing with FNS, the technique may also provide increased functional capabilities to individuals with SCI [7]. Being able to stand and reach objects may enhance the independence of persons with SCI and improve their quality of life. In order to be able to reach at a counter with an FNS system, the user first must be able to maintain stable postural control while standing.
Able-bodied postural control has been analyzed by monitoring the subtle shifts in the center of pressure (COP) that occur when a subject is quietly standing [8], [9]. Alternative methods test postural stability by applying a perturbation to a standing subject and analyzing the subject’s response to this disturbance [10]–[16]. Other researchers have investigated postural responses when the perturbation was a result of a subject-controlled motion such as rapid arm movements [17], [18] or leaning while carrying a load [19]. Reaching while standing is another example of a subject-controlled perturbation, although most studies involving reaching have been predominantly concerned with kinematic control of the upper extremities [20], [21].
Postural responses in able-bodied individuals involve a coordinated activation of synergistic muscles that may be modulated by experience [12]. Adjusting the foot placement of a standing subject changes the biomechanical constraints of the lower extremities and would also likely alter postural responses. Examples of constraints that are dependent on foot placement include the size of the base of support and the geometrical orientations of the passive structures for the lower extremities. While the majority of the aforementioned studies were performed with the subjects in side-by-side stances, several studies examined postural responses with alternative foot placements. These studies found altered postural responses [9], [19] and utilization of different motor control strategies [8] when various foot placements were adopted. Therefore, altered postural responses as a function of foot placement may be due to changes in the biomechanical constraints that influence muscle coordination strategy.
In able-bodied individuals, standing balance can be maintained when reaching by a combination of coordinated joint rotations that may involve movement of the COP between the two feet. As an example of coordinated rotations, ankle plantarflexion can be combined with hip flexion on the same extremity to maintain balance. The COP must remain within the base of support, which is an area bounded by the outer points of contact for both feet with the floor. Since the base of support is defined by the positioning of the feet, the ability to shift the COP may be manipulated by adjusting foot placement prior to the execution of movement.
In the case of SCI individuals standing with FNS, stimulated muscles provide stability through joint stiffness, but precise control of joint rotations may be impractical. However, COP shifts may be possible by gross adjustments of the stimulation levels to the lower extremities. Sufficient joint stiffness is also necessary to maintain balance during upper extremity motions involved in reaching. It is intuitive that widening one’s stance from a side-by-side foot placement may increase one’s ability to shift weight in the medial/lateral (M/L) direction (see Section II for foot placement definitions). Likewise, shifting a foot forward from the side-by-side stance to a modified tandem stance should increase one’s ability to shift weight in the anterior/posterior (A/P) direction. Furthermore, altering foot placement may change the coordination between joint rotations that are required to shift one’s weight while reaching. In both the side-by-side and wide foot placements, a complex balance of opposing ankle plantarflexion/dorsiflexion and hip flexion/extension may be required to maintain the A/P COP within a base of support limited by foot length. However, the modified tandem stance increases the A/P base of support and may allow a coordinated movement where ankle dorsiflexion and hip flexion simultaneously occur during reaching. This would result in a potentially simpler postural control problem, as stiffness in the form of ankle plantarflexion and hip extension moments would both act in the same direction to maintain balance. Such a control strategy may prove more feasible to implement with an FNS standing system.
In this study, we focused on the task of reaching at a counter because it may provide increased functional benefits to individuals with SCI. More specifically, preparatory adjustments prior to reaching and the postural responses to this subject-controlled perturbation were of particular interest. This study with able-bodied individuals investigates the possibility that proper foot placement may improve postural stability while standing and performing reaching tasks. Using able-bodied individuals for initial studies allows the repetitive testing of multiple conditions without the safety concerns that dominate experimental protocols involving persons standing with FNS. The use of able-bodied experiments in the design of FNS systems is commonplace [16], [22], [23] and rooted in the belief that FNS standing should mimic intact standing without being overly complex. Foot placements that provide advantages to able-bodied individuals will be considered as likely candidates for improved standing with FNS.
The goals of this study were: 1) to quantify the postural effects of foot placement on able-bodied subjects while standing and reaching at a counter and 2) to use the results in the design of control strategies for FNS standing systems. It was hypothesized that a wide foot placement would result in an enhanced utilization of M/L COP excursions when reaching to the right and left. A second hypothesis was that a modified tandem stance would result in an increased utilization of A/P COP excursions and that it would significantly affect joint coordination strategy when reaching forward.
II. Methods
A. Experimental Protocol
Five participants (age 28.8 ± 7.6 years) volunteered for this study after providing informed consent. As depicted in Fig. 1, [24], the participants performed a series of reaching tasks using three different foot placements: side-by-side stance; wide stance; and modified tandem stance. The side-by-side stance had the feet at a width (ankle joint center to ankle joint center) approximately equal to the distance between the subject’s anterior superior iliac spines. The wide stance also had the subject’s feet side-by-side, but at a width twice that of the side-by-side stance [19]. The modified tandem stance had the feet at side-by-side width, but with one leg shifted anteriorly and the other shifted posteriorly, each by half the subject’s foot length (similar to the 45° position in [9]). The leg chosen to shift forward corresponded to the subject’s dominant hand that was utilized for the reaching tasks (all five subjects were right-hand dominant). As each participant performed the reaching tasks, 29 reflective markers (12 additional markers were used for static calibration) were tracked using a six camera Motion Analysis (Santa Rosa, CA) video system (Fig. 2). The participant also stood with each foot on a separate Kistler (Amherst, NY) force platform during the trials to measure ground reactions and centers of pressure.
Fig. 1.
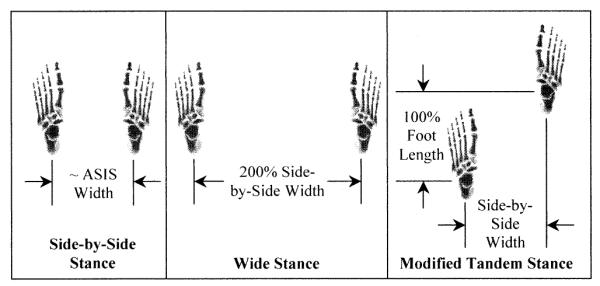
Foot placements used during the reaching trials. The ankle joint to ankle joint stance width for the side-by-side foot placement was approximately the width between the subject’s anterior superior iliac spines. Stance widths for the alternative foot placements are indicated in terms of the side-by-side stance width. For the tandem stance, the ankle joint to ankle joint stance depth is 100% of the participant’s foot length. The images of the foot and other body segments depicted in Figs. 1–3, and 5 were created using SIMM software (Musculographics, Evanston, IL).
Fig. 2.
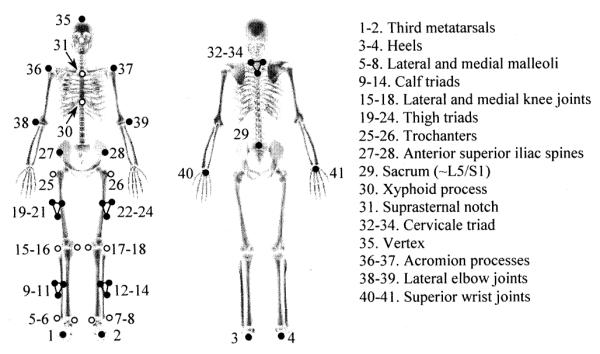
Reflective marker set used for video tracking. Twenty-nine reflective markers were dynamically tracked during the reaching motions (filled circles). Twelve additional markers were used during static calibration to identify anatomical landmarks (open circles). The triads were rigid groupings of three markers attached to segments of interest.
During the reaching trials, each participant moved a 1-kg object to selected positions on a table 90 cm in height. Initially, each participant moved the object with their right (dominant) hand to their maximum reach in the anterior direction (maximum center reach). The subjects were instructed to let their left arm hang freely at their side and not to use their left hand to lean against the table. The maximum center reach was measured and 75% of this distance was marked at three different orientations: 45° to the right of center; center; and 45° to the left of center. Movements to these locations were referred to as “targeted” reaches. Participants were then asked to perform a series of six motions for each trial at a comfortable pace that would be completed within a 20-s interval. As depicted in Fig. 3, the motions included targeted and maximum reaches in the right, center, and left directions. The targeted reaches in each direction were of equal length, while the maximum reaches indicated the maximal reach capability in each direction. This series of six reaches was repeated three times for each foot placement for a total of nine trials (54 reaches) for each participant.
Fig. 3.
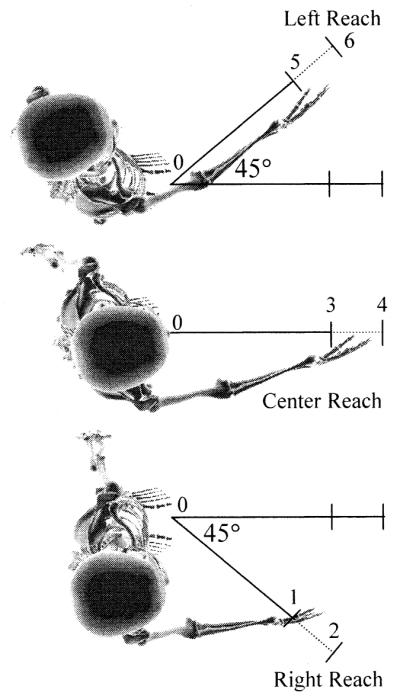
Overhead view of reaching trials. (1) Targeted right reach. (2) Maximum right reach. (3) Targeted center reach. (4) Maximum center reach. (5) Targeted left reach. (6) Maximum left reach. Subjects began at the starting position (0) and returned to this position between each reach. The model depicting the reaching motion was developed with SIMM using kinematic data measured during the reaching trials.
B. Biomechanical Analysis
The following parameters were calculated to quantify postural adjustments during reaching: maximum reach; COP trace boundaries; COP excursions; joint angle excursions; and joint moments. Maximum reach was measured using the 27 untargeted tasks per subject, while COP excursions and joint angle excursions were measured using the 27 targeted tasks per subject. The data from the set of six reaches in each trial were used to determine COP trace boundaries and correlations between various pairs of kinematic/kinetic variables. Joint moments were calculated for the targeted center reach from each of the nine trials per subject.
Maximum reach was calculated from marker data by determining the displacement of the right wrist marker from the starting reach position to the maximum reach positions. An increase in maximum reach when using a particular foot placement would indicate that greater reach distances could be achieved before approaching the limits of functional capability. The COP traces were calculated and normalized in the A/P direction by the A/P base of support and in the M/L direction by the M/L base of support for each respective stance. To find the COP trace boundaries, the normalized data were converted to polar coordinates and the outer radial boundary of the trace was determined. Plots of the COP trace boundaries illustrate the area within the base of support used by the subject and allow comparisons of weight shift patterns across reaching directions. In addition, the maximum A/P and M/L COP excursions during the targeted reaches were compiled to compare these values at equal reach distances. Maximum COP excursions give an indication for each foot placement of the role that lower extremity weight shifts play in the completion of each reach task. The remaining analyses focused upon the targeted reaching tasks since they represent functional reaching tasks that are likely to be used in activities of daily living.
Joint centers for the ankles, knees, hips, and L5/S1 intervertebral disk were estimated using tracked and reconstructed anatomical landmark positions [25]. In addition, clusters of anatomical landmark and joint center positions were used to designate axes for the calf, thigh, lower torso, and upper torso. Three successive Euler rotations (flexion/extension, abduction/adduction, and axial twist) were used to define the joint angles between adjacent sets of segmental axes throughout the reaching motion. From these data, joint angle excursions were determined by subtracting joint angles at the targeted reach posture from the initial posture. Joint angle excursions were used to indicate the strategy of joint coordination utilized during reaching for each foot placement. Next, segment parameters were calculated using participant anthropometric measurements and predictive equations [26], [27]. Joint moments occurring during the targeted center reach were then determined using Newton-Euler equations of motion starting at the foot segments and working successively through the body to the lower torso [28]. Maximum joint moments were analyzed to predict whether the joints were exposed to greater magnitudes of loading when adopting different foot placements.
In order to further analyze coordination strategies, correlation coefficients (−1≤0≤1) were calculated to quantify the relationship between pairs of kinematic/kinetic variables. The time series of wrist marker position was used as an indicator of reach output; the time series of the A/P component of COP and the A/P component of sacral marker position were used to represent lower body maneuvers. The correlation coefficients were calculated between wrist marker position and each of the lower body measures to evaluate the consistency in the relationships between these varaibles. The A/P component of these values was chosen since FNS reaching will likely involve predominantly sagittal joint rotations of the lower extremities.
C. Statistical Analysis
Multivariate ANOVA was performed using SAS (Cary, NC) to test the dependence of maximum reach, COP excursions, and joint angle excursions on trial number, foot placement, and reach direction. In addition, these dependent variables were tested using least square means for effects between foot placements, reach directions, and foot placement/reach direction interactions. Each dependent variable was tested for significance at p < 0.05 on each individual subject’s data and combined as a group of five subjects. These steps were taken to determine if one subject biased the results of the group and to determine the percentage of subjects that followed the overall trend of the group. Therefore, dependent variables that displayed statistical significance for all five subjects individually and as a group of five subjects were considered to be the strongest relationships. Similarly, multivariate ANOVA was utilized to test the dependence of the maximum joint moments for targeted center reach on trial number and foot placement. For this dependent variable, least square means were tested for effects between foot placements. As before, the maximum joint moments for targeted center reach were tested for significance at p < 0.05 on each individual subject’s data and as a group of five subjects.
III. Results
A. Maximum Reach
Maximum reach was not significantly dependent on foot placement (Fig. 4). Across the set of five subjects, maximum reach to the left was significantly greater than maximum reach to the right or to the center. Maximum reach to the left was also significantly greater when analyzing each of the five subjects individually. None of the parameters tested using ANOVA were statistically dependent on the trial number.
Fig. 4.

Maximum reach distances with respect to foot placement and reach direction. The maximum reach values depicted were averaged over five subjects and three repetitions. Brackets extending from the bar graphs indicate standard error values. For each of the foot placements, maximum reach to the left was significantly greater (p < 0.05) than maximum reach to the right or to the center for each of the five subjects and as a group.
B. Centers of Pressure
In Fig. 5, COP trace boundaries are separated in each reach direction for a representative set of six reaches from subject one and combined for the entire reaching sequence when averaged over all subjects. In this figure, side-by-side foot placement boundaries are outlined with a rectangle, and the cross hairs indicate the theoretical maximum A/P and M/L boundaries for each stance. Qualitatively, the COP traces occurred within unique boundaries for each reach direction when using the side-by-side and wide stances. In contrast, the COP traces using the modified tandem stance were similar for all reach directions. When averaged across subjects, the COP trace boundaries for the self-selected and wide stances were similar to one another.
Fig. 5.

COP trace boundaries as a function of foot placement. The first row of traces was taken from individual trials that were representative of the group, while the second row of traces are averages over five subjects and three repetitions. In the first row, the right and left reach COP trace boundaries are represented with thin lines and the center reach COP with a thick line. In the second row, a thick line represents a composite of all three reach directions.
Both A/P and M/L COP excursions were statistically dependent upon reach direction. A/P COP excursions were statistically greater for targeted center reach as compared to targeted left reach in 5/5 subjects and for targeted right reach as compared to targeted left reach in 4/5 subjects. In addition, both A/P and M/L COP excursions were also dependent upon foot placement. When comparing specific reaching tasks, A/P COP excursions were significantly greater for targeted right reach when using the modified tandem stance than when using the side-by-side or wide stances (Fig. 6). Similarly, A/P COP excursions for targeted center reach were significantly greater when using the modified tandem stance as compared to the side-by-side or wide stances. In contrast, M/L COP excursions for targeted left reach were significantly greater when using the side-by-side and wide stances than when using the tandem stance.
Fig. 6.

COP excursions as a function of reach direction and foot placement. For each subject, the data points represent the COP excursion averaged over three trials for each foot placement. Inequality signs represent group-averaged statistical differences between foot placements for p 0.05. For example, T > S means that the modified tandem stance had a significantly greater center of pressure excursion than the side-by-side stance. The number of subjects that showed individual significance appears within parentheses. (Abbreviations: S1 … S5—subjects one-five; S—side-by-side; W—wide; and T—modified tandem.)
C. Joint Angle Excursions
All joint angle excursions were dependent upon reach direction except trunk extension and right ankle abduction. For example, right hip external rotation, left hip internal rotation, and trunk lateral bending to the left all significantly increased from targeted right to targeted center to targeted left reach. When comparing foot placements, right ankle plantarflexion was significantly greater for the side-by-side and wide stances during targeted center reach as compared to the modified tandem stance, which instead involved dorsiflexion (Table I). In contrast, significantly greater right hip abduction occurred when using the modified tandem stance for targeted left reach as compared to the self-selected stance. Left ankle eversion was also significantly greater when using the wide stance for targeted left reach as compared to the tandem stance. Each of these joint angle excursions provided insight into the changes in coordination strategy that occurred when the foot placement was altered.
TABLE I.
Joint Angle Excursions as a Function of Reach Direction and Foot Placement. The Angles Listed Are the Variables That Showed Consistent Dependence on Foot Placement Across the Group of Subjects. Results Were Averaged Over Five Subjects and Three Repetitions. Standard Errors Are Also Displayed. Inequality Signs Represent Group-Averaged Statistical Differences Between Foot Placements for p < 0.05. The Number of Subjects That Showed Individual Significance Appears Within Parentheses. (Abbreviations: S—Side-by-Side; W—Wide; And T—Modified Tandem)
| Joint Angle |
Reach Direction |
Side-by- Side (S) |
Wide (W) |
Modified Tandem (T) |
Statistical Significance |
|---|---|---|---|---|---|
| Right Hip | Right | 4.1° ± 1.1° | 1.8° ± 1.0° | 1.3° ± 1.0° | |
| Abduction | Center | 6.7° ± 1.0° | 7.2° ± 1.0° | 5.3° ± 1.0° | |
| Left | 5.9° ± 1.0° | 9.0° ± 1.0° | 11.8° ± 1.0° | T > S (4/5) | |
|
| |||||
| Right Ankle | Right | 1.1° ± 0.7° | 2.0° ± 0.6° | -1.1° ± 0.6° | |
| Plantarflexion | Center | 1.6° ± 0.6° | 2.3° ± 0.6° | -2.4° ± 0.6° | S > T (5/5), W > T (5/5) |
| Left | -1.5° ± 0.6° | -0.2° ± 0.6° | -2.1° ± 0.6° | ||
|
| |||||
| Left Ankle | Right | -0.8° ± 0.5° | -1.3° ± 0.5° | -2.5° ± 0.5° | |
| Eversion | Center | 1.1° ± 0.5° | 1.0° + 0.5° | -1.4° ± 0.5° | |
| Left | 3.5° ± 0.5° | 3.8° ± 0.5° | 1.5° ± 0.5° | W > T (4/5) | |
D. Maximum Joint Moments
Joint moments for targeted center reach are displayed as a function of normalized reach time, with the participant in the starting posture at 0% and returning to the initial posture at 100% (Fig. 7). Maximum right knee flexion and right hip abduction moments were significantly greater when using the modified tandem stance as compared to the side-by-side and wide foot placements. Trunk extension moments were also significantly greater when using the modified tandem stance as compared to the wide foot placement. These maximal joint moments occurred as targeted center reach was approached. Maximum left hip extension moments were also significantly greater when using the tandem stance as compared to the side-by-side and wide foot placements. In contrast, these maximal joint moments occurred during the initial and final standing postures.
Fig. 7.

Joint moments during targeted center reach. Results were averaged over five participants and three repetitions. The moments were normalized over reach time with 0% and 100% representing the starting posture. Inequality signs represent statistical differences for maximum moments as a function of foot placement. The number of subjects that showed individual significance appears within parentheses. (Abbreviations: S—side-by-side; W—wide; and T—modified tandem.)
E. Coordination Patterns During Reaching
The mean correlation coefficient between wrist displacement and A/P COP was 0.89 (0.85 ≤ R ≤ 0.92) for side-by-side, 0.88 (0.81 ≤ R ≤ 0.94) for wide, and 0.87 (0.80 ≤ R ≤ 0.94) for modified tandem stances. Three subjects displayed inverse relationships between wrist displacement and sacral marker position for the side-by-side (mean = −0.42, −0.60 ≤ R ≤ −0.12) and wide stances (mean = −0.50, −0.74 ≤ R ≤ −0.20). In contrast, the remaining two subjects had consistently positive correlations averaging 0.49 (0.33 ≤ R ≤ 0.65) for the side-by-side and 0.42 (0.10 ≤ R ≤ 0.69) for the wide stances. For the modified tandem stance, correlations between wrist displacement and sacral marker position were always positive, with four subjects resulting in higher coefficients (mean = 0.80, 0.70 ≤ R ≤ 0.89) than the remaining subject (mean = 0.51, 0.31 ≤ R ≤ 0.71). In Fig. 8, the time series of the variables are displayed for trials performed by subject one that are representative of the group. In addition, stick figures are displayed that illustrate the relative changes of these variables during reaching.
Fig. 8.

Coordination patterns during reaching. Results are shown for trials performed by subject one that are representative of the group. The graphs in column one represent a set of reaches using the side-by-side stance, and the graphs in column two represent a set of reaches using the modified tandem stance. Wrist displacement, A/P COP, and A/P sacral marker position were normalized over the time taken to complete the set of six reaching tasks. Correlation coefficients between the wrist displacement and the kinematic/kinetic measurements are displayed in the lower right-hand corner of these graphs. The stick figures in the third row demonstrate the relative changes of these parameters during reaching.
IV. Discussion and Conclusion
Although targeted reaching distances were normalized to maximum center reach, there were some subject-to-subject differences in the magnitude of the biomechanical parameters. This might be due to individual differences in reaching strategy or differences in height, arm length, and/or other anthropometric measures. In contrast, no statistical dependencies were found due to trial number, which implies that subject fatigue and learning effects were not significant factors. One curious result (Fig. 4) was the fact that maximum reach to the left was greater than the maximum reach to the right or center. This is deceptive however, since subjects twisted the trunk, which rotated the shoulder closer to the target. Subjects also found reaching to the left to be least favorable.
1) COP Trace Boundaries Follow Consistent Patterns for Modified Tandem Stance
Individual COP trace boundaries displayed a “birdlike” pattern for the side-by-side and wide stances and an ellipse along the base of support for the modified tandem stance (Fig. 5). The subjects shifted their weight differently for each reach direction when using the side-by-side and wide stances. For these foot placements, the COP followed a path that was approximately parallel to the line of action for the particular reaching task. In addition, the wide stance may allow ‘sloppier’ control [9] for reaching to the right and left, since the COP trace boundaries were similar in area to self-selected stance, but a smaller percent of the maximum. When using the modified tandem stance, participants demonstrated a similar strategy for shifting their weight regardless of the reach direction. Each subject showed a distinct transfer of weight to their front foot, especially during reaching tasks to the right and center. This is of interest since it indicates that the weight shifting strategy with the modified tandem stance was more generalized and could be used for multiple tasks.
Increased A/P COP excursions with the modified tandem stance for the targeted right reach and the targeted center reach can be attributed to a base of support that was more closely aligned to the reach directions (Fig. 6). These findings were consistent with the hypothesis that the modified tandem stance would enhance a person’s ability to shift their weight forward and back. In contrast, decreased M/L COP excursions with the modified tandem stance for the targeted left reach were likely due to a base of support alignment that was nearly perpendicular to the reach direction. Contrary to expectations, the wide stance did not result in significantly greater M/L COP excursions as compared to the side-by-side stance. This may simply be an indication that the reaching tasks did not require additional medial/lateral shifting of weight beyond the capabilities available with the side-by-side stance. There may also be additional stiffness present in the ankle and hip joints during the wide stance as a result of additional baseline ankle inversion and hip abduction involved with this foot placement. Outer stability boundaries were rarely approached with any stance, which was consistent with prior reports that COP excursions were restricted to 89% of the theoretical maximum when handling a load [19].
2) Modified Tandem Stance Allowed a Translational Shift of the Pelvis
Hip to ankle angle excursion ratios averaged from 3 to 6 for the sagittal joint planes in all targeted reach directions for each foot placement. The lower range of these values were in agreement with a previous study that simulated A/P perturbations and found an optimal hip to ankle ratio of 3 [29]. During the targeted reaches, the modified tandem stance resulted in right ankle dorsiflexion, which was consistent with shifting of weight from the back to front foot (Table I). Therefore, the modified tandem stance increased the available range of movement of the pelvis that could be utilized during reaching. In agreement with expectations, increases in A/P COP excursions with the modified tandem stance were a function of directionally consistent ankle (dorsiflexion) and hip (flexion) joint rotations. This finding has potential benefit when using an FNS standing system, since rotations at these joints may be superimposed to result in the required weight shift to complete a reaching task. This is in contrast to the side-by-side and wide stances, where opposing ankle and hip joint rotations would have to be balanced in an FNS standing system.
In general, the joint moment requirements were similar during the targeted center reach for the side-by-side and wide foot placements (Fig. 7). However, the modified tandem stance resulted in additional knee and hip stiffness requirements for both the initial and final reaching postures. In the initial upright posture, higher left-knee abduction and left-hip extension moments were consistent with the subject’s weight being preferentially shifted back on the left foot. Similarly, higher right knee flexion and right hip abduction moments in the targeted center reach posture were indicative of the subject’s weight being shifted to the front foot as the reaching target was attained. For all foot placements, large trunk extension moments were associated with small trunk extension angle excursions for the targeted center reach, which indicates stiffening rather than rotation of the trunk. Therefore, as the COP shifted anteriorly during reaching, trunk extension moments stiffened the trunk to counteract the effects of gravity. The increased joint moment requirements for the initial posture when using the modified tandem stance are of particular concern for the FNS standing system user. A stable quiet stance will be essential before the FNS user can be expected to reach, and the modified tandem stance may be inappropriate for those with insufficient hip stiffness.
The upper extremities would likely be used for partial support during reaching for FNS standing system users, which may alter the postural adjustments observed with able-bodied subjects. However, the able-bodied data is consistent with the goal of FNS standing with minimal hand support or hands-free standing. Nondominant hand support may be advantageous for all stances in terms of providing extension moments to the trunk and hips, thereby reducing the requirements for trunk and hip stiffness. Use of the upper extremity may also be particularly beneficial during the modified tandem stance since the base of support would be increased by forming a tripod.
3) Modified Tandem Stance Produces Consistent Upper/Lower Body Coordination Patterns
The use of online readings from sensors in an FNS standing system is of interest to correct imperfections in a feedforward control system and to detect unforeseen perturbations that a user might encounter. Sensor measurements could also be used in adaptive control systems to indicate day-to-day differences in muscle response to stimulation and to detect the onset of fatigue. When examining the biomechanics of reach for potential sources of online information in an FNS standing system, A/P COP was highly correlated with wrist displacement (Fig. 8). For all foot placements, the subject shifted their weight forward as their wrist displacement increased toward a targeted or maximal reach. This relationship was particularly strong during reaches to the right and to the center. In order to incorporate A/P COP feedback into an FNS standing system, force platforms can be used in a laboratory setting or pressure sensors placed in the shoes could be used in a portable system. Questions remain about the durability of pressure sensors placed in the shoes and, therefore, a second sensor measurement, A/P sacral marker position, was also explored.
In three of five subjects using the side-by-side and wide stances, the A/P sacral marker position was inversely related to the wrist displacement. These findings were consistent with a postural strategy of ankle plantarflexion combined with hip flexion, which results in the pelvis moving posteriorly as the subject reaches anteriorly. For the other two subjects, the A/P sacral marker position was directly, but weakly correlated to the wrist displacement when using the side-by-side and wide stances. In contrast, four out of the five subjects resulted in high correlations between A/P sacral marker position and wrist displacement when using the modified tandem stance. For the remaining subject using the modified tandem stance, the correlation was also positive, though lower than the other four subjects. Therefore, the modified tandem stance resulted in translational shifting of the pelvis in the anterior direction as the subject reached forward. To implement the A/P pelvic position in an FNS standing system, there are several laboratory-based systems for kinematic tracking as well as potentially viable options for portable sensors that use accelerometers, gyroscopes, and/or goniometers. Such a system may be more difficult to implement if the side-by-side or wide stances are utilized during reaching due to the varying postural strategies utilized (pelvis backward or pelvis forward) with these foot placements. The amplitude of the signals were also larger with the tandem stance, which would put lower demands on the resolution and signal to noise ratio of a sensor system.
4) Concluding Remarks
The capability to shift weight and the postural mechanisms involved in shifting weight during reaching differed according to foot placement. The foot placements tested in this study represented the outer limits of what a person might naturally assume, and one would likely receive graded benefits from assuming an intermediate stance. For example, a FNS user who has difficulty shifting their weight forward might be aided by assuming a modified tandem posture where the feet are shifted a quarter foot length anteriorly and posteriorly. Moreover, reaching to the left was problematical when using the modified tandem stance. This may prove to be a less important issue in FNS standing when the left hand is used to provide an additional point of support.
An important implication of this study is that the modified tandem stance resulted in postural benefits during reaching and should be further investigated as a means of improving the capabilities of FNS system users. One potential advantage of the modified tandem stance may be that a consistent control strategy can be used in which weight is shifted from the back to the front foot. A second potential advantage may be the more predictable and useful readings from a pelvic-based position sensor during reaching. When using the modified tandem stance, one potential disadvantage is that more active and more precise control of hip moments may be required. In preliminary studies with an SCI subject using surface electrode stimulation, no difficulties were detected in maintaining quiet standing posture when using the modified tandem stance [30]. If needed, additional hip control could be achieved by modulating stimulation to the hip musculature or by adjusting support from the left hand during a right hand reach. The ultimate test of these foot placements will be implementation with multiple FNS users, where a mix of hand support and muscle stimulation will have to replace voluntary control.
Acknowledgment
The authors would like to thank J. Resig for her assistance.
This work was supported in part by the National Center for Medical Rehabilitation Research of the National Institute for Child Health and Development (NIH-RO1-HD-38 570) and in part by the Center for Biomedical Engineering, University of Kentucky, Lexington. This work was performed at the Center for Biomedical Engineering, University of Kentucky.
Biography
Jason C. Gillette received the B.S. degree in engineering science, the M.E. degree in engineering mechanics, and the Ph.D. degree in biomedical engineering/engineering mechanics from Iowa State University, Ames, in 1991, 1993, and 1999, respectively.
From 1999 to 2002, he was a Postdoctoral Scholar with the Center for Biomedical Engineering, the University of Kentucky, Lexington. He is currently an Assistant Professor with the Department of Health and Human Performance, Iowa State University, Ames. His research interests include biomechanics, motor control, neuromuscular electrical stimulation, and rehabilitation engineering.

James J. Abbas (S’87-M’92) received the Sc.B. degree in bioelectrical engineering from Brown University, Providence, RI, in 1982 and the M.S. and Ph.D. degrees in biomedical engineering from Case Western Reserve University, Cleveland, OH, in 1989 and 1992, respectively.
From 1982 to 1984, he taught secondary school mathematics in Mzuzu, Malawi. His biomedical research has included work as a Biomedical Engineer at the Motion Study Laboratory, Cleveland Veterans Affairs Medical Center, Cleveland, OH, and as a Research Fellow at Shriners Hospital, Philadelphia, PA. From 1993 to 1995, he was an Assistant Professor of Biomedical Engineering in the Department of Mechanical Engineering, The Catholic University of America, Washington, DC. From 1995 to 2002, he was an Assistant, then Associate Professor in the Center for Biomedical Engineering and the Department of Physical Medicine and Rehabilitation, the University of Kentucky, Lexington. He is currently an Associate Professor with the Harrington Department of Bioengineering, Arizona State University, Tempe, and in the Department of Clinical Neurobiology and Bioengineering, Good Samaritan Rehabilitation Institute, Phoenix, AZ.
Contributor Information
Jason C. Gillette, Department of Health and Human Performance, Iowa State University, Ames, IA 50011 USA (gillette@iastate.edu).
James J. Abbas, Harrington Department of Bioengineering, Arizona State University, Tempe, AZ 85287 USA; Department of Clinical Neurobiology and Bioengineering, Good Samaritan Rehabilitation Institute, Phoenix, AZ 85278 USA..
References
- [1].Kralj A, Bajd T. Functional Electrical Stimulation: Standing and Walking After Spinal Cord Injury. CRC; Boca Raton, FL: 1989. pp. 49–122. [Google Scholar]
- [2].Yarkony GM, Roth EJ, Cybulski G, Jaeger RJ. Neuromuscular stimulation in spinal chord injury I: Restoration of functional movement of the extremities. Arch. Phys. Med. Rehab. 1992;73:78–86. [PubMed] [Google Scholar]
- [3].Triolo RJ, Kobetic R, Betz RR. Standing and walking with functional neuromuscular stimulation. In: Harris G, editor. Human Motion Analysis. IEEE Press; New York: 1996. pp. 318–350. [Google Scholar]
- [4].Quintern J. Application of functional electrical stimulation in paraplegic patients. NeuroRehab. 1998;10:205–250. [Google Scholar]
- [5].Kobetic R, Triolo RJ, Uhlir JP, Bieri C, Wibowo M, Polando G, Marsolais EB, Davis JA, Ferguson KA, Sharma M. Implanted functional electrical stimulation system for mobility in paraplegia: A follow-up case report. IEEE Trans. Rehab. Eng. 1999 Dec.7:390–398. doi: 10.1109/86.808942. [DOI] [PubMed] [Google Scholar]
- [6].Uhlir JP, Triolo RJ, Kobetic R. The use of selective electrical stimulation of the quadriceps to improve standing function in paraplegia. IEEE Trans. Rehab. Eng. 2000 Dec.8:514–522. doi: 10.1109/86.895955. [DOI] [PubMed] [Google Scholar]
- [7].Abbas JJ, Gillette JC. Using electrical stimulation to control standing posture. IEEE Control Syst. Mag. 2001 Aug.21:80–90. [Google Scholar]
- [8].Winter DA, Prince F, Frank JS, Powell C, Zabjek KF. Unified theory regarding A/P and M/L balance in quiet stance. J. Neurophysiol. 1996;75:2334–2343. doi: 10.1152/jn.1996.75.6.2334. [DOI] [PubMed] [Google Scholar]
- [9].Winter DA, Patla AE, Prince F, Ishac M, Gielo-Perczak K. Stiffness control of balance in quiet standing. J. Neurophysiol. 1998;80:1211–1221. doi: 10.1152/jn.1998.80.3.1211. [DOI] [PubMed] [Google Scholar]
- [10].Nashner LM, Cordo PJ. Relation of automatic postural responses and reaction-time voluntary movements of human leg muscles. Exp. Brain Res. 1981;43:395–405. doi: 10.1007/BF00238382. [DOI] [PubMed] [Google Scholar]
- [11].Maki BE, Holliday PJ, Fernie GR. A posture control model and balance test for the prediction of relative postural stability. IEEE Trans. Biomed. Eng. 1987 Oct.34:797–810. doi: 10.1109/tbme.1987.325922. [DOI] [PubMed] [Google Scholar]
- [12].Horak FB, Diener HC, Nashner LM. Influence of central set on human postural responses. J. Neurophysiol. 1989;62:841–853. doi: 10.1152/jn.1989.62.4.841. [DOI] [PubMed] [Google Scholar]
- [13].Brown LA, Frank JS. Postural compensations to the potential consequences of instability: Kinematics. Gait Posture. 1997;6:89–97. [Google Scholar]
- [14].Henry SM, Fung J, Horak FB. Control of stance during lateral and anterior/posterior surface translations. IEEE Trans. Rehab. Eng. 1998 Mar.6:32–42. doi: 10.1109/86.662618. [DOI] [PubMed] [Google Scholar]
- [15].Rietdyk S, Patla AE, Winter DA, Ishac MG, Little CE. Balance recovery from medio-lateral perturbations of the upper body during standing. J. Biomech. 1999;32:1149–1158. doi: 10.1016/s0021-9290(99)00116-5. [DOI] [PubMed] [Google Scholar]
- [16].Popovic MR, Pappas IPI, Nakazawa K, Keller T, Morari M, Dietz V. Stability criterion for controlling standing in able-bodied subjects. J. Biomech. 2000;33:1359–1368. doi: 10.1016/s0021-9290(00)00123-8. [DOI] [PubMed] [Google Scholar]
- [17].Aruin AS, Latash MF. Directional specificity of postural muscles in feed-forward postural reactions during fast voluntary arm movements. Exp. Brain. Res. 1992;103:323–332. doi: 10.1007/BF00231718. [DOI] [PubMed] [Google Scholar]
- [18].Moynahan M. Postural responses during standing in subjects with spinal-cord injury. Gait Posture. 1995;3:156–165. [Google Scholar]
- [19].Holbein MA, Chaffin DB. Stability limits in extreme postures: Effects of load positioning, foot placement, and strength. Hum. Factors. 1997;39:456–468. doi: 10.1518/001872097778827160. [DOI] [PubMed] [Google Scholar]
- [20].Gottlieb GL, Corcos DM, Agarwal GC, Latash ML. Principles underlying single-joint movement strategies. In: Winters JM, Woo SL, editors. Multiple Muscle Systems: Biomechanics and Movement Organization. Springer-Verlag; New York: 1990. pp. 236–250. [Google Scholar]
- [21].Zhang X, Kuo AD, Chaffin DB. Optimization-based differential kinematic modeling exhibits a velocity-control strategy for dynamic posture determination in seated reaching movements. J. Biomech. 1998;31:1035–1042. doi: 10.1016/s0021-9290(98)00117-1. [DOI] [PubMed] [Google Scholar]
- [22].Matjacic Z, Bajd T. Arm-free paraplegic standing—Part II: Experimental results. IEEE Trans. Rehabil. Eng. 1998 Jun;6:139–150. doi: 10.1109/86.681179. [DOI] [PubMed] [Google Scholar]
- [23].Munih M, Donaldson NN, Hunt KJ, Barr FMD. Feedback control of unsupported standing in paraplegia—Part II: Experimental results. IEEE Trans. Rehabil. Eng. 1997 Dec.5:341–352. doi: 10.1109/86.650288. [DOI] [PubMed] [Google Scholar]
- [24].Delp SL, Loan JP. A graphics-based software system to develop and analyze models of musculoskeletal structures. Comput. Biol. Med. 1995;25:21–34. doi: 10.1016/0010-4825(95)98882-e. [DOI] [PubMed] [Google Scholar]
- [25].Cappozzo A, Cappello A, Croce UD, Pensalfini F. Surface-marker cluster design criteria for 3-D bone movement reconstruction. IEEE Trans. Biomed. Eng. 1997 Dec.44:1165–1174. doi: 10.1109/10.649988. [DOI] [PubMed] [Google Scholar]
- [26].Zatsiorsky V, Seluyanov V. The mass and inertia characteristics of the main segments of the human body. In: Matsui H, Kobayashi K, editors. Biomechanics VIII-B. Human Kinetics; Champaign, IL: 1983. pp. 1152–1159. [Google Scholar]
- [27].de Leva P. Adjustments to Zatsiorsky-Seluyanov’s segment inertia parameters. J. Biomech. 1996;29:1223–1230. doi: 10.1016/0021-9290(95)00178-6. [DOI] [PubMed] [Google Scholar]
- [28].Kingma I, de Looze MP, Toussaint HM, Klijnsma HG, Bruijnen TBM. Validation of a full body 3-D dynamic linked segment model. Hum. Mov. Sci. 1996;15:833–860. [Google Scholar]
- [29].Kuo AD, Zajac FE. Human standing posture: Multi-joint movement strategies based on biomechanical constraints. Prog. Brain Res. 1993;97:349–358. doi: 10.1016/s0079-6123(08)62294-3. [DOI] [PubMed] [Google Scholar]
- [30].Gillette JC, Riess J, Abbas JJ. Comparison of FNS-assisted and able-bodied quiet stance. In: Triolo RJ, editor. Proc. 6th Annu. Conf. Int. Functional Electrical Stimulation Soc.; Cleveland, OH: 2001. pp. 268–270. [Google Scholar]