

Abstract
Objective
Examine policymakers’ public policy priorities related to physical activity and the built environment, identify classes of policymakers based on priorities using latent class analysis (LCA), and assess factors associated with class membership.
Design
Cross-sectional survey data from municipal officials in 94 cities and towns across six U.S. states were analyzed.
Participants
Participants (N=423) were elected or appointed municipal officials spanning public health, planning, transportation/public works, community and economic development, parks and recreation, and city management.
Main Outcome Measures
Participants rated the importance of 11 policy areas (public health, physical activity, obesity, economic development, livability, climate change, air quality, natural resource conservation, traffic congestion; traffic safety, and needs of vulnerable populations) in their daily job responsibilities. LCA was used to determine response patterns and identify distinct classes based on officials’ priorities. Logistic regression models assessed participant characteristics associated with class membership.
Results
Four classes of officials based on policy priorities emerged: 1) economic development and livability; 2) economic development and traffic concerns; 3) public health; and 4) general (all policy areas rated as highly important). Compared to class 4, officials in classes 1 and 3 were more likely to have a graduate degree; officials in class 2 were less likely to be in a public health job/department, and officials in class 3 were more likely to be in a public health job/department.
Conclusions
Findings can guide public health professionals in framing discussions with policymakers to maximize physical activity potential of public policy initiatives, particularly economic development.
Keywords: physical activity, public policy, policymakers, built environment
Introduction
The built environment is a major driver of physical activity patterns.1 Efforts to restructure communities to promote physical activity as part of daily life are needed to combat the current trends of physical inactivity in the U.S.2 Public health authorities recommend community designs that enable and promote daily walking and bicycling as the most sustainable approach to increasing population physical activity.3 However, re-structuring the built environment typically requires considerable time, money, and political engagement.4
Much policymaking occurs at the local level,5 with local health officials often competing with other policymakers’ non-health priorities in advocating for policies and environments that promote physical activity. Scientific articles call for public health professionals to appeal to policymakers on the basis of evidence to support physical activity initiatives6 or recommend that policymakers “implement” findings from research.7 However, multiple issues influence policymaker decisions, including budget, policy compatibility, and stakeholder interests.8, 9 Understanding policymaker priorities and how to better target messages for this audience is critical for translating scientific findings into policy actions10, 11 and identifying leverage points in the policy process. Previous studies have explored issues important to local policymakers that could impact obesity12, 13 or active living14–16 but have not addressed ways for public health professionals to strategically engage with policymakers to implement active living initiatives.
Latent class analysis (LCA) is an analytic approach that illuminates patterns of responses based on a set of observed variables with a finite number of mutually exclusive and exhaustive classes. An individual is assigned to a latent class based on his/her response patterns.17 This paper aimed to utilize LCA to: 1) identify distinct classes of policymakers based on policy areas related to physical activity and the built environment; and 2) assess characteristics associated with class membership. We hypothesized that policymakers’ job department would be associated with class membership.
Methods
This study used data gathered from a multi-site study led by institutions participating in the Centers for Disease Control and Prevention-funded Physical Activity Policy Research Network (PAPRN). The study was coordinated by the University of Massachusetts Medical School with investigators from seven other PAPRN–affiliated universities across the U.S. All study procedures were approved by the institutional review boards at each of these institutions.
Study sample and recruitment
The target population consisted of elected and appointed municipal officials from U.S. cities with ≥ 50,000 residents (based on the 2010 U.S. Census) across eight states (CO, GA, HI, KS, MA, MO, NC, WV). Elected officials included mayors and municipal legislators (city councilors, aldermen, commissioners, selectmen, policy staff). Appointed officials included city/town managers, and heads of departments of planning, community development, economic development, public works, transportation, engineering, parks and recreation, neighborhood services, and public health. Eligible officials were identified from the Municipal Yellow Book (www.leadershipdirectories.com) and municipality websites.
Survey development and administration
A web-based survey was developed based on key informant interviews with municipal officials and academicians and a comprehensive literature review of relevant constructs.18 Investigators convened to achieve consensus on selection of measures, modification of items from existing validated surveys, and development of new items. Cognitive interviews were conducted to pilot test the survey with municipal officials (n=4). The final 43-item survey (available upon request) was programmed in Qualtrics and underwent usability testing.
A standardized survey administration protocol was followed.18 Participants were emailed personalized invitations including a description of the study purpose and links to the consent form and survey. Participants were assured confidentiality and provided with investigator contact information. Non-responders who did not actively refuse participation received an email reminder after one week. Subsequent non-responders received up to three telephone reminders over a 5-week period. Participants from six states were invited to enter a raffle for one of ten $25 gift cards following survey completion (two institutions did not allow raffles). All responses were obtained via self-report web-based survey and completed in 2012.
Measures
Participants were asked to rate the importance of 11 public policy areas (economic development/revitalization; livability/smart growth; traffic congestion; traffic safety; air quality; needs of vulnerable populations; public health; obesity; physical activity; energy conservation/climate change; and natural resource conservation) in the “day-to-day responsibilities of [their] current position.” Response categories included not at all, somewhat, or very important. The concept of livability, though undefined on the survey, was intended to capture physical and social aspects of the environment,19 with the Australian Major Cities Unit’s definition of urban livability (cities that are “socially inclusive, affordable, accessible, healthy, safe and resilient to the impacts of climate change”) serving as a comprehensive definition.20, 21
Position was assessed with two items that classified job department (e.g., planning, community or economic development, public works or transportation, parks and recreation, public health) and job function (e.g., title or position). Job departments and positions were combined into one variable (job department/position) for the final models due to small cell sample sizes; categories included: planning, community or economic development, public works or transportation, parks and recreation, public health, mayor or city or town manager, or local elected official). Gender, race/ethnicity, highest level of education completed, and political ideology (liberal, moderate, or conservative) on social and fiscal issues were assessed.
Statistical analysis
Descriptive analyses of sample characteristics and the distribution of perceived importance of public policy areas to participants’ job responsibilities were conducted. A series of independently estimated LCAs was used to identify classes based on perceived importance of policy areas to job responsibilities. For the LCA, responses were dichotomized as very important or somewhat/not at all important. A series of models with number of classes ranging from two to five were estimated. Model selection and class size were determined using Akaike information criteria (AIC), Bayesian information criteria (BIC), sample size adjusted BIC, and the Lo-Mendell-Rubin likelihood ratio test. Participant sociodemographics by classes were compared using chi-square tests. A series of bivariate multinomial logistic regression models comparing classes 1, 2, and 3 (classes that prioritized specific issues) to class 4 (all issues highly prioritized) were used to examine sociodemographics associated with class membership. LCA were completed using Mplus version 6.1, and descriptive statistics and regression models were conducted using SAS version 9.3.
Results
Study Sample
Of the 1,773 municipal officials invited to complete the survey, 461 (26%) participated. Of the 461 respondents, 38 (8.2%) were excluded from analysis due to missing data on one or more measures. The final analytic sample comprised 423 municipal officials across 84 cities and towns. The majority of the sample were male (69.7%), of White ethnicity (79.9%), and had a graduate degree (57.7%). The distribution of job department/position was as follows: local elected officials (not mayor) (30.3%); community or economic development department (13.7%); public works or transportation department (13.2%); parks and recreation department (12.5%); planning department (10.4%); mayor or city or town manager (9.2%); public health department (8.7%); and job position spanning multiple departments (1.9%). Nearly one-third (32.1%) of the sample identified as conservative in social affiliation; 53.4% identified as conservative in fiscal affiliation. Further details on response rate, comparison of non-respondents to respondents, and sample demographics are described elsewhere.18
Importance to Job Responsibilities
Municipal officials’ perceptions of the importance of public policy areas in their daily job responsibilities varied across the 11 areas (Table 1). The majority rated economic development/revitalization (73.8%), livability/smart growth (67.8%), and needs of vulnerable populations (65.5%) as very important to their daily job responsibilities. Over half reported traffic safety (55.8%), public health (55.8%), and air quality (50.1%) as very important issues. Less than half of participants viewed obesity, physical activity, energy conservation/climate change, natural resource conservation, and traffic congestion as very important to their job (response rates ranging from 40.7% to 48.9%).
Table 1.
Importance of Various Public Policies in Current Position (N = 423)
| Importance of _______in Daily Responsibilities | N | % |
|---|---|---|
| Economic development/revitalization | ||
| Not at all | 9 | 2.1 |
| Somewhat | 102 | 24.1 |
| Very | 312 | 73.8 |
| Livability/Smart growth | ||
| Not at all | 12 | 2.8 |
| Somewhat | 124 | 29.3 |
| Very | 287 | 67.8 |
| Traffic congestion | ||
| Not at all | 40 | 9.5 |
| Somewhat | 185 | 43.7 |
| Very | 198 | 46.8 |
| Traffic safety | ||
| Not at all | 35 | 8.3 |
| Somewhat | 152 | 35.9 |
| Very | 236 | 55.8 |
| Air quality | ||
| Not at all | 35 | 8.3 |
| Somewhat | 176 | 41.6 |
| Very | 212 | 50.1 |
| Needs of vulnerable populations | ||
| Not at all | 12 | 2.8 |
| Somewhat | 134 | 31.7 |
| Very | 277 | 65.5 |
| Public health | ||
| Not at all | 15 | 3.6 |
| Somewhat | 172 | 40.7 |
| Very | 236 | 55.8 |
| Obesity | ||
| Not at all | 67 | 15.8 |
| Somewhat | 184 | 43.5 |
| Very | 172 | 40.7 |
| Physical activity | ||
| Not at all | 38 | 9.0 |
| Somewhat | 178 | 42.1 |
| Very | 207 | 48.9 |
| Energy conservation/climate change | ||
| Not at all | 31 | 7.3 |
| Somewhat | 214 | 50.6 |
| Very | 177 | 41.8 |
| Natural resource conservation | ||
| Not at all | 22 | 5.2 |
| Somewhat | 215 | 50.8 |
| Very | 186 | 44.0 |
Latent Class Analysis
The LCA fit indices for responses to the perceived importance of public policy areas in daily job responsibilities supported a 4-class solution, depicted in Figure 1. The four latent classes were of roughly comparable size and interpreted to conceptualize public policy areas as follows: 1) economic development/revitalization and livability/smart growth (23.2% of the sample); 2) economic development/revitalization, traffic safety, and traffic congestion (30.3% of the sample); 3) public health, physical activity, obesity, and needs of vulnerable populations (25.8% of the sample); and 4) general (high probability (>0.7) of rating an issue as somewhat or very important for all of the 11 areas identified) (20.8% of the sample). Compared to a 3-class model, the 4-class model had lower AIC, BIC and sample size adjusted BIC. Additionally, the Lo-Mendell-Rubin likelihood ratio test (p<.0001) suggested that the 4-class solution provided a better fit over a 3-class solution. A 5-class model did not provide significant improvement over a 4-class solution (Lo-Mendell-Rubin likelihood ratio test (p=0.2)).
Figure 1.
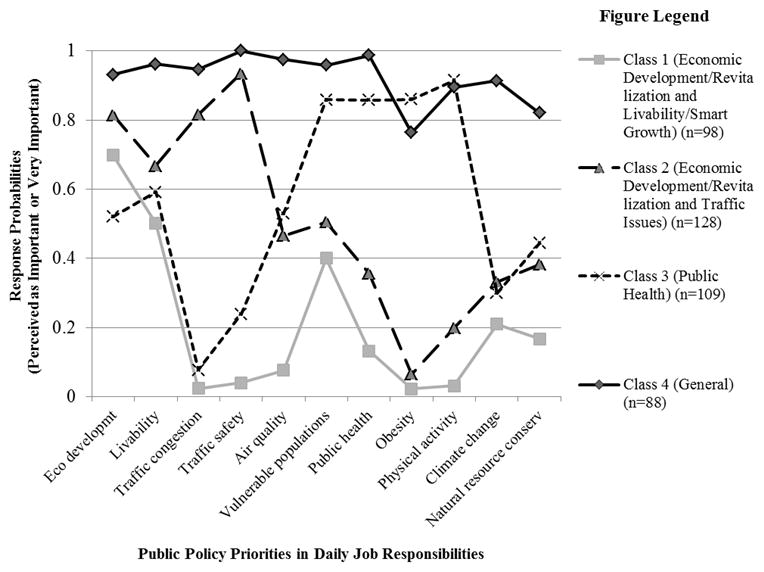
Results of the 4-Class Latent Class Analyses: Response Probabilities of Perceived Importance of Various Public Policy Priorities in Daily Job Responsibilities among U.S. Municipal Officials (2012) (N=423)
Sample Characteristics and Latent Class Membership
Table 2 presents the distribution of participant characteristics by the four classes identified. Class membership differed by type of job department/position (p<0.0001), with 55.1% of participants in class 1 (economic development/revitalization and livability/smart growth) having positions in planning or community or economic development departments; 35.9% of participants in class 2 (economic development/revitalization and traffic issues) were elected officials and 27.3% worked in public works or transportation departments; 60.6% of participants in class 3 (public health) working in parks and recreation or public health departments; and 50.0% of participants in class 4 (general) holding a local elected official position (not mayor).
Table 2.
Distribution of Sample Characteristics According to Latent Classes (N = 423)
| Class 1 (n = 98) Economic development/revitalization and livability/smart growth |
Class 2 (n = 128) Economic development/revitalization and traffic- related issues |
Class 3 (n=109) Public health |
Class 4 (n=88) General |
p-value* | |
|---|---|---|---|---|---|
| Gender, % | 0.332 | ||||
| Male | 66.3 | 75.8 | 68.8 | 65.9 | |
| Race/ethnicity | 0.283 | ||||
| White, % | 83.7 | 83.6 | 79.8 | 72.7 | |
| Highest level of education, % | 0.082 | ||||
| ≤ College degree | 36.7 | 43.0 | 37.6 | 53.4 | |
| Graduate degree | 63.3 | 57.0 | 62.4 | 46.6 | |
| Job department/position, % | <0.0001 | ||||
| Multiple departments | 2.0 | 3.9 | 0.9 | 0 | |
| Local elected official (not mayor) | 16.3 | 35.9 | 20.2 | 50.0 | |
| Planning | 20.4 | 10.9 | 2.7 | 7.9 | |
| Community or economic development | 34.7 | 10.9 | 7.3 | 2.3 | |
| Public works or transportation | 5.1 | 27.3 | 3.7 | 13.6 | |
| Mayor or city or town manager | 12.2 | 10.2 | 4.6 | 10.2 | |
| Parks and recreation | 7.1 | 0 | 35.8 | 8.0 | |
| Public health | 2.0 | 0.8 | 24.8 | 8.0 | |
| Social affiliation, % | 0.098 | ||||
| Liberal | 46.9 | 28.9 | 44.0 | 43.2 | |
| Moderate | 24.5 | 30.5 | 28.4 | 27.3 | |
| Conservative | 28.6 | 40.6 | 27.5 | 29.5 | |
| Fiscal affiliation, % | 0.133 | ||||
| Liberal | 22.4 | 10.2 | 21.1 | 19.3 | |
| Moderate | 32.7 | 31.2 | 24.8 | 26.1 | |
| Conservative | 44.9 | 58.6 | 54.1 | 54.6 |
p-values are from chi-squared tests
Table 3 presents estimates of participant characteristics associated with class membership from bivariate multinomial logistic regression models. Compared to municipal officials in class 4 (general), those in class 1 (economic development/revitalization and livability/smart growth) and class 3 (public health) were nearly twice as likely to have a graduate degree (OR=1.97; 95% confidence interval (CI): 1.10 to 3.55; OR = 1.90; 95% CI: 1.07–3.36, respectively). Municipal officials in class 2 (economic development/revitalization and traffic-related issues) were less likely than those in class 4 to be in a public health job or department (OR=0.09; 95% CI: 0.01 to 0.75), whereas officials in class 3 (public health) were more likely than those in class 4 to be in a public health job or department (OR=3.81; 95% CI: 1.57–9.24).
Table 3.
Bivariate Multinomial Logistic Regression Models of Sociodemographics Associated with Class Membership (N=423)
| OR | 95% CI | p-value | |
|---|---|---|---|
| Class 1 (Economic development/revitalization and smart growth/livability) vs. Class 4 (General) | |||
|
| |||
| Gender (female vs. male) | 1.02 | 0.56–1.87 | 0.952 |
| Race/ethnicity (non-White vs. White) | 0.54 | 0.26–1.11 | 0.095 |
| Education (graduate degree vs. ≤ college degree) | 1.97 | 1.10–3.55 | 0.023* |
| Job department/position (public health vs. others) | 0.24 | 0.049–1.19 | 0.081 |
| Social affiliation | |||
| (Liberal vs. moderate) | 1.21 | 0.60–2.46 | 0.598 |
| (Conservative vs. moderate) | 1.08 | 0.50–1.93 | 0.852 |
| Fiscal affiliation | |||
| (Liberal vs. moderate) | 0.93 | 0.41–2.13 | 0.864 |
| (Conservative vs. moderate) | 0.66 | 0.34–1.29 | 0.225 |
|
| |||
| Class 2 (Economic development/revitalization and traffic-related issues) vs. Class 4 (General) | |||
|
| |||
| Gender (female vs. male) | 1.62 | 0.89–2.94 | 0.115 |
| Race/ethnicity (non-White vs. White) | 0.58 | 0.30–1.12 | 0.104 |
| Education (graduate degree vs. ≤ college degree) | 1.52 | 0.88–2.63 | 0.132 |
| Job department/position (public health vs. others) | 0.091 | 0.011–0.75 | 0.026* |
| Social affiliation | |||
| (Liberal vs. moderate) | 0.60 | 0.30–1.18 | 0.141 |
| (Conservative vs. moderate) | 1.23 | 0.62–2.46 | 0.557 |
| Fiscal affiliation | |||
| (Liberal vs. moderate) | 0.44 | 0.18–1.07 | 0.069 |
| (Conservative vs. moderate) | 0.90 | 0.48–1.68 | 0.738 |
|
| |||
| Class 3 (Public health) vs. Class 4 (General) | |||
|
| |||
| Gender | 1.14 | 0.63–2.08 | 0.666 |
| Race/ethnicity | 0.74 | 0.38–1.44 | 0.382 |
| Education (graduate degree vs. ≤ college degree) | 1.90 | 1.07–3.36 | 0.027* |
| Job department/position (public health vs. others) | 3.81 | 1.57–9.24 | 0.003* |
| Social affiliation | |||
| (Liberal vs. moderate) | 0.98 | 0.49–1.93 | 0.949 |
| (Conservative vs. moderate) | 0.89 | 0.42–1.89 | 0.767 |
| Fiscal affiliation | |||
| (Liberal vs. moderate) | 1.15 | 0.50–2.66 | 0.740 |
| (Conservative vs. moderate) | 1.05 | 0.53–2.06 | 0.894 |
Discussion
This study aimed to examine patterns among local policymakers’ priorities to better understand how collaborations promoting physical activity and built environment initiatives may be enhanced. To our knowledge, no other study has examined municipal officials’ perceptions of public policy issues in their daily job responsibilities regarding physical activity and the built environment using LCA. Overall, findings indicate that non-health rationales for changing the built environment to support active living may be more likely to appeal to municipal officials than health-oriented rationales.
Among a set of issues that may positively impact community design for active living, economic development/revitalization ranked highest in importance to daily job responsibilities among municipal officials in our study, with obesity and physical activity ranking lower in importance. The prioritization of economic development is not surprising given theories from sociology and political science about the relation between economic development and political power at the local level. Regime theory, for instance, focuses on “collaborative arrangements through which local governments and private actors assemble the capacity to govern”22 in which business interests are considered key participants. Previous analyses of the data on which the current analysis is based revealed correlations between greater perceived importance of economic development and traffic congestion to job responsibilities and involvement in public works/transportation policy to increase bicycle and pedestrian accommodation.23
The finding that physical activity was of low priority among municipal officials aligns with previous research. Only 12% of Hawaii state and county officials rated physical activity as an important problem in 2009, with affordable housing, drug abuse, and quality education ranked as top concerns.12 Physical activity was a priority for only 27% of officials responsible for land use and community design.24 Although Kansas state legislators and appointed officials recognized obesity as a problem, they introduced legislation targeting budget, education, and jobs/economy.25 Among municipal planning directors whose communities had adopted innovative land use policies in support of active living, increasing physical activity was not a top priority, although a higher number of innovative policies related to active living were adopted within these communities.14 Lack of political will is frequently cited by officials as a barrier to greater consideration of physical activity in built environment decision making.14, 18, 24 These findings suggest that re-framing physical activity initiatives in terms of the impact on “livability, dynamic centers and economic development”14 may narrow the gap between priority and municipal action.
Livability/smart growth and needs of vulnerable populations emerged as other top priorities among municipal officials in our study, whereas energy conservation/climate change and natural resource conservation were of low priority. Encouragingly, local public health officials reported obesity and physical activity to be very important to their job responsibilities. However, the National Association of County and City Health Officials has reported severe and continuing budget cuts to the nation’s local health departments and has found low percentages reporting policy/advocacy activity in these areas,26 indicating a lack of resources to support active living initiatives at the local level. The importance of livability/smart growth to job responsibilities among municipal officials suggests that opportunities aligning physical activity-promoting initiatives with livability (e.g., provide a variety of transportation choices, invest in building healthy, safe and walkable neighborhoods) may be more likely to resonate with policymakers.
As expected, job department/position correlated with importance to job responsibilities on community design issues with potential impact on physical activity, with the majority of respondents who prioritized public health (class 3) working in parks and recreation or public health departments. Multinomial regression models indicated that job department/position predicted class membership, with those prioritizing economic development/revitalization and traffic-related issues (class 2) less likely to be in a public health job or department and those prioritizing public health (class 3) more likely to be in a public health job or department compared with officials who prioritized all issues (class 4). Interestingly, no differences in social or fiscal affiliations across classes were observed. One possible interpretation for this finding is that the patterns of policy priorities that emerged in this study are ubiquitous across social and fiscal affiliation, suggesting that the emphasis should be on targeting recommendations based on policymaker priorities.
Findings provide nuanced information health officials and advocates can use to tailor messages and relationship-building approaches with local officials depending on their place in the system. Officials in class 3 reported high job responsibility for health-related policy areas and low responsibility for traffic safety and congestion, with modest responsibility for economic development/revitalization and livability. These officials and health advocates must recognize potential gaps between their prioritization of issues and that of other officials, acknowledging the obligation of local officials to fulfill their mission as defined by local administration. Officials may find public health sources of information about the health value of walkability insufficient rationale to change from business as usual. One strategy is to emphasize the economic and livability benefits of active living approaches rather than focusing on health advantages alone. Health officials can also seek to justify resource allocation for active transportation approaches by making explicit connections between these areas and public health issues such as obesity, air quality, and injury prevention. One vehicle for this redefinition is the Public Health Accreditation Board (PHAB) process,27 through which health officials can include additional measures (e.g., walking and biking behaviors, environmental conditions) into Community Health Assessment and Community Health Improvement Plan metrics.
Officials in class 1 placed high priority on economic development/revitalization and livability/smart growth and low responsibility for traffic congestion and safety and public health issues. Messages for such officials should focus on the benefits of maximizing walkability and bikeability of development projects to create vibrant places where people can and want to live, work, and play and the economic impact of such measures. Health officials and advocates can support new definitions of economic success and livability that support active travel, using evidence such as higher retail spending by walkers and bicyclists and attraction of young talent to vibrant, walkable areas. Public health advocates who speak comfortably about return on investment, “placemaking” (planning, design and management of public spaces through capitalizing on community’s assets and potential)28, and smart growth can be powerful voices supporting innovative policy solutions. Examples of resources in these areas include LOCUS: Responsible Real Estate Developers and Investors,29 a program of Smart Growth America, and the Urban Land Institute (ULI),30 a research and education organization whose mission is leadership in responsible land use.
Officials in class 2 reported high responsibility for traffic safety and congestion and economic development and livability, with some responsibility for air quality and public health generally but low responsibility for physical activity or obesity. In addition to the economic development and livability approaches noted above, health officials and advocates can support efforts to improve safe active travel that are branded to meet other goals, such as the USDOT Safer Streets/Stronger Economies initiative.31 Health officials can support congestion mitigation strategies that emphasize demand reduction (e.g., promote bicycle and pedestrian travel over road widening).
Officials in class 4 reported high responsibility for most policy areas investigated in this analysis, although low responsibility specifically for physical activity. These officials, notably elected officials, may respond best to comprehensive community mobilization approaches that call for walkable and bikeable environments as part of a larger, integrated effort for community improvement. Elected officials’ need for stories in public forums may make narrative approaches especially useful in communicating the need for physical activity and built environment initiatives.32 Additionally, collaboratives and coalitions are critical to achieving policy, systems, and environmental changes to improve community physical activity through engaging elected officials33 and targeting built environment change.34 Prior research indicates that coalitions with members from sectors of interest scored higher on “strategic alignment,” which is in turn associated with higher perceived coalition success.35 Previous analysis of the current study’s data indicated that membership in a community partnership or coalition to create environments that support physical activity was positively associated with policy participation in community design, active transportation, and park access.36 These findings suggest that beyond educating policy makers, establishing collaboratives may strengthen capacity to support the “co-benefit” areas investigated in this study.
The public health community should recognize that communicating the health or economic benefits of local policy changes, or even supporting changes in policy mechanisms, will not assure implementation. Voicing a set of policy priorities often does not guarantee policy engagement, adoption, and/or implementation. The limited existing public policy and political science scholarship focused on the local level suggests that a rational or linear model of the process is less accurate than a “recursive,” or iterative, relationship between policy and action.37 Policy development is one of the core functions of public health,38 although policy involvement by local officials is low,39 and researchers often lack expertise and skills in understanding the policy process.40 While the public health field has increasingly embraced models such as Kingdon’s Multiple Streams over a linear policy model41 and support for Health in All Policies42 appears to be growing, officials and advocates must infuse public health concerns into community dialogue on these other topics by participating in existing processes. This will require investing time and effort in learning about and responding to officials’ priorities by applying methods of relationship building long employed with community partners.18 For example, providing communication trainings for public health professionals to address varied audiences, including policymakers, is an important skill to promote trans-disciplinary and cross-sector collaborations. Such strategies can move public health beyond traditional education and encouragement approaches towards participation in placemaking and other policy-based solutions.28 Public health, with its focus on equity for vulnerable populations, can help ensure the benefits of placemaking are enjoyed by the many and not limited to a privileged few.
Strengths and Limitations
Study strengths include the sample of municipal officials across multiple disciplines representing numerous states and urban areas across the U.S. Findings should be considered in light of the following limitations. Survey response rate was low (26%), although several study protocol measures were implemented to encourage participation, including sending personalized email invitations and reminders via email and telephone, assurance of confidentiality, and provision of raffle prizes. Only municipal officials from urban areas (>50,000 residents) were identified for inclusion; thus, findings may not be generalizable to rural and suburban areas. All data were obtained via self-report, and the survey instrument was not extensively tested for reliability and validity. Livability was not defined on the survey. As several definitions of livability exist,20, 21, 43, 44 participants may have had different interpretations of the construct. The item assessing perceived importance of public policy priorities focused on importance of issues for daily job responsibilities; results may have been different if importance was rated for other considerations, such as priority for action and importance for the community. While informed by formative research, the list of policy areas was not exhaustive to minimize respondent burden.
Conclusion
Study findings suggest that effective strategies to engage local policymakers and garner their support for physical activity-friendly built environment policy may benefit from adopting a targeted messaging approach. Emphasizing benefits to other policy priorities (e.g. economic development and transportation) through initiatives that also promote physical activity and built environment may be a promising approach to achieving policy change.
Acknowledgments
Source of Funding
This study was funded in part by the Centers for Disease Control and Prevention (CDC) Cooperative Agreement Number U48/DP001903 from the CDC, Prevention Research Centers Program, Special Interest Project 9-09, and the Physical Activity Policy Research Network. The content is solely the responsibility of the authors and does not necessarily represent the official views of the CDC. Support was also provided by a grant from the National Cancer Institute at the National Institutes of Health entitled: “Mentored Training for Dissemination and Implementation Research” (grant no. R25 CA171994).
Footnotes
Conflict of Interests
The authors declare no conflicts of interest.
References
- 1.Heath GW, Brownson RC, Kruger J, Miles R, Powell KE, Ramsey LT, et al. The effectiveness of urban design and land use and transport policies and practices to increase physical activity: a systematic review. Journal of Physical Activity and Health. 2006;3(Supp 1):S55–S76. doi: 10.1123/jpah.3.s1.s55. [DOI] [PubMed] [Google Scholar]
- 2.Brown BB, Smith KR, Hanson H, Fan JX, Kowaleski-Jones L, Zick CD. Neighborhood design for walking and biking: physical activity and body mass index. American Journal of Preventive Medicine. 2013;44(3):231–8. doi: 10.1016/j.amepre.2012.10.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Centers for Disease Control and Prevention (CDC) CDC recommendations for improving health through transportation policy. 2010 Available from: http://www.cdc.gov/transportation/recommendation.htm.
- 4.Dobson NG, Gilroy AR. From partnership to policy: the evolution of active living by design in Portland, Oregon. American Journal of Preventive Medicine. 2009;37(6 Suppl 2):S436–44. doi: 10.1016/j.amepre.2009.09.008. [DOI] [PubMed] [Google Scholar]
- 5.Brownson RC, Ballew P, Dieffenderfer B, Haire-Joshu D, Heath GW, Kreuter MW, et al. Evidence-based interventions to promote physical activity: what contributes to dissemination by state health departments. American Journal of Preventive Medicine. 2007 Jul;33(1 Suppl):S66–73. doi: 10.1016/j.amepre.2007.03.011. quiz S4–8. [DOI] [PubMed] [Google Scholar]
- 6.Institute of Medicine (US) and National Research Council (US) Committee on Childhood Obesity Prevention Actions for Local Governments. Local government actions to prevent childhood obesity. Washington, D.C: National Academies Press (US); 2009. [Google Scholar]
- 7.Murphy K, Fafard P. Taking power, politics, and policy problems seriously: the limits of knowledge translation for urban health research. Journal of Urban Health. 2012;89(4):723–32. doi: 10.1007/s11524-012-9694-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Liu X, Lindquist E, Vedlitz A, Vincent K. Understanding local policymaking: policy elites’ perceptions of local agenda setting and alternative policy selection. Policy Studies Journal. 2010;38(1):69–91. [Google Scholar]
- 9.Dodson EA, Stamatakis KA, Chalifour S, Haire-Joshu D, McBride T, Brownson RC. State legislators’ work on public health-related issues: what influences priorities? Journal of Public Health Management & Practice. 2013;19(1):25–9. doi: 10.1097/PHH.0b013e318246475c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bernier NF, Clavier C. Public health policy research: making the case for a political science approach. Health Promotion International. 2011;26(1):109–16. doi: 10.1093/heapro/daq079. [DOI] [PubMed] [Google Scholar]
- 11.Rütten A, Abu-Omar K, Gelius P, Schow D. Physical inactivity as a policy problem: applying a concept from policy analysis to a public health issue. Health Research Policy and Systems. 2013;11(1):9. doi: 10.1186/1478-4505-11-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Maddock JE, Reger-Nash B, Heinrich K, Leyden KM, Bias TK. Priority of activity-friendly community issues among key decision makers in Hawaii. Journal of Physical Activity and Health. 2009;6(3):386–90. doi: 10.1123/jpah.6.3.386. [DOI] [PubMed] [Google Scholar]
- 13.Leyden KM, Reger-Nash B, Bauman A, Bias T. Changing the hearts and minds of policy makers: an exploratory study associated with the West Virginia Walks campaign. American Journal of Health Promotion. 2008;22(3):204. doi: 10.4278/ajhp.22.3.204. [DOI] [PubMed] [Google Scholar]
- 14.Dill J, Howe D. The role of health and physical activity in the adoption of innovate land use policy: findings from surveys of local governments. Journal of Physical Activity and Health. 2011;8(Suppl 1):S116–24. doi: 10.1123/jpah.8.s1.s116. [DOI] [PubMed] [Google Scholar]
- 15.Clark MI, Berry TR, Spence JC, Nykiforuk C, Carlson M, Blanchard C. Key stakeholder perspectives on the development of walkable neighbourhoods. Health Place. 2010;16(1):43–50. doi: 10.1016/j.healthplace.2009.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Allender S, Gleeson E, Crammon B, Sacks G, Lawrence M, Peeters A, et al. Policy change to create supportive environments for physical activity and healthy eating: which options are the most realistic for local government? Health Promotion International. 2012;27(2):261–74. doi: 10.1093/heapro/dar018. [DOI] [PubMed] [Google Scholar]
- 17.Nylund KL, Asparouhov TA, Muthen BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo Simulation Study. Structural Equation Modeling. 2007;14(4):535–69. [Google Scholar]
- 18.Goins KV, Schneider KL, Brownson R, Carnoske C, Evenson KR, Eyler A, et al. Municipal officials’ perceived barriers to consideration of physical activity in community design decision making. Journal of Public Health Management & Practice. 2013;19(3 Suppl 1):S65–73. doi: 10.1097/PHH.0b013e318284970e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hankins KB, Powers EM. The Disappearance of the State from “Livable” Urban Spaces. Antipode. 2009;41(5):845–66. [Google Scholar]
- 20.Infrastructure Australia - Major Cities Unit. State of Australian cities 2010: Infrastructure Australia, Major Cities Unit. 2010. [Google Scholar]
- 21.Badland H, Whitzman C, Lowe M, Davern M, Aye L, Butterworth I, et al. Urban liveability: emerging lessons from Australia for exploring the potential for indicators to measure the social determinants of health. Social Science & Medicine. 2014;111:64–73. doi: 10.1016/j.socscimed.2014.04.003. [DOI] [PubMed] [Google Scholar]
- 22.Mossberger K, Stoker G. The evolution of urban regime theory: The challenge of conceptualization. Urban Affairs Review. 2001;36(6):810–35. [Google Scholar]
- 23.Zwald ML, Eyler AA, Goins KV, Brownson RC, Schmid TL, Lemon SC. Understanding Municipal Officials’ Involvement in Transportation Policies Supportive of Walking and Bicycling. Journal of public health management and practice: JPHMP. 2014 Oct 14; doi: 10.1097/PHH.0000000000000152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hollander M, Martin SL, Vehige T. The surveys are in! The role of local government in supporting active community design. Journal of Public Health Management & Practice. 2008 May-Jun;14(3):228–37. doi: 10.1097/01.PHH.0000316481.27017.07. [DOI] [PubMed] [Google Scholar]
- 25.Heinrich KM, Stephen MO, Vaughan KB, Kellogg M. Kansas legislators prioritize obesity but overlook nutrition and physical activity issues. Journal of Public Health Management & Practice. 2013 Mar-Apr;19(2):139–45. doi: 10.1097/PHH.0b013e318254cc57. [DOI] [PubMed] [Google Scholar]
- 26.National Association of County & City Health Officials (NACCHO) 2013 National Profile of Local Health Departments. 2014 [cited 2014 October 20]; Available from: http://nacchoprofilestudy.org/wp-content/uploads/2014/02/2013_National_Profile021014.pdf.
- 27.Public Health Acreditation Board. Public Health Accreditation Board: Advancing Public Health Performance. 2013 [cited 2015 April 22]; Available from: http://www.phaboard.org/
- 28.National Prevention Council. National Prevention Strategy. Washington, D.C: U.S. Department of Health & Human Services, Office of the Surgeon General; 2011. [Google Scholar]
- 29.Smart Growth America. LOCUS: Smart Growth America. 2014 [cited 2014 October 23]; Available from: http://www.smartgrowthamerica.org/locus/
- 30.Urban Land Institute. 2014 [cited 2014 October 23]; Available from: http://uli.org/research/centers-initiatives/building-healthy-places-initiative/
- 31.Smart Growth America. Safer Streets, Stronger Economies. 2015 [cited 2015 April 23]; Available from: http://www.smartgrowthamerica.org/documents/safer-streets-stronger-economies.pdf.
- 32.Stamatakis KA, McBride TD, Brownson RC. Communicating prevention messages to policy makers: the role of stories in promoting physical activity. Journal of Physical Activity and Health. 2010 Mar;7( Suppl 1):S99–107. doi: 10.1123/jpah.7.s1.s99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Litt JS, Reed HL, Tabak RG, Zieff SG, Eyler AA, Lyn R, et al. Active living collaboratives in the United States: understanding characteristics, activities, and achievement of environmental and policy change. Preventing Chronic Disease. 2013;10:E19. doi: 10.5888/pcd10.120162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gustat J, Healy I, Litt J, Reed H, Tabak RG, Goins KV, et al. Lessons in promoting active living: the collaborative perspective. Journal of Public Health Management & Practice. 2013 May-Jun;19(3 Suppl 1):S58–64. doi: 10.1097/PHH.0b013e318284b3c6. [DOI] [PubMed] [Google Scholar]
- 35.Bornstein DB, Pate RR, Beets MW, Ortaglia A, Saunders RP, Blair SN. New Perspective on Factors Related to Coalition Success: Novel Findings From an Investigation of Physical Activity Coalitions Across the United States. Journal of public health management and practice: JPHMP. 2015 Feb 12; doi: 10.1097/PHH.0000000000000190. [DOI] [PubMed] [Google Scholar]
- 36.Lemon SC, Goins KV, Schneider KL, Brownson RC, Valko CA, Evenson KR, et al. Municipal Officials’ Participation in Built Environment Policy Development in the United States. American Journal of Health Promotion. 2014 Nov 5; doi: 10.4278/ajhp.131021-QUAN-536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hill M. Policy Process: A Reader. 2. London: Routledge; 2014. [Google Scholar]
- 38.Institute of Medicine. The Future of the Public’s Health in the 21st Century. Washington, DC: 2002. [Google Scholar]
- 39.Thompson A, Boardley D, Kerr D, Greene T, Jenkins M. Public policy involvement by health commissioners. Journal of community health. 2009 Aug;34(4):239–45. doi: 10.1007/s10900-009-9158-4. [DOI] [PubMed] [Google Scholar]
- 40.Brownson RC, Royer C, Ewing R, McBride TD. Researchers and policymakers: travelers in parallel universes. American Journal of Preventive Medicine. 2006 Feb;30(2):164–72. doi: 10.1016/j.amepre.2005.10.004. [DOI] [PubMed] [Google Scholar]
- 41.Lyn R, Aytur S, Davis TA, Eyler AA, Evenson KR, Chriqui JF, et al. Policy, systems, and environmental approaches for obesity prevention: a framework to inform local and state action. Journal of Public Health Management & Practice. 2013 May-Jun;19(3 Suppl 1):S23–33. doi: 10.1097/PHH.0b013e3182841709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Rudolph L, Caplan J, Ben-Moshe K, Dillon L. Health in All Policies: A Guide for State and Local Governments. Washington, D.C., Oakland, C.A: American Public Health Association, Public Health Institute; 2013. [Google Scholar]
- 43.Chazal J. A systems approach to livability and sustainability: defining terms and mapping relationships to link desires with ecological opportunities and constraints. Systems Research and Behavioral Science. 2010;27(5):585–97. [Google Scholar]
- 44.Pacione M. Urban liveability: a review. Urban Geography. 1990;11(1):1–30. [Google Scholar]