

Abstract
Aim
To assess whether the introduction of episiotomy scissors specially designed to achieve a cutting angle of 60°, EPISCISSORS-60®, in two hospitals in the UK would result in a reduction in obstetric anal sphincter injuries (OASIS) in nulliparous women.
Methods
A structured training program for all doctors and midwives provided a theoretical framework around OASIS including risk factors and the role of episiotomies and a practical hands-on training element to use EPISCISSORS-60® correctly and to measure perineal body length and post-suturing angles. Data for perineal body length, post-suturing angles, user feedback, episiotomy use, and incidence of OASIS were collected through specifically designed forms and the general hospital data collection system.
Results
Data were available for 838 nulliparous vaginal deliveries. Mean perineal body length was 37 mm in spontaneous vaginal delivery group (standard deviation [SD] =8.3, 95% confidence interval [CI] =34–39) and 38 mm in the operative vaginal delivery group (SD=8, 95% CI=35–40). Post-suturing episiotomy angles were 53° (SD=6.5, 95% CI=50.7–55.8) in spontaneous vaginal deliveries and 52° (SD=9.6, 95% CI=49–54) in operative vaginal deliveries. EPISCISSORS-60® were rated as “good” to “very good” by 84% of users. There was a 47% increase in the number of episiotomies in nulliparous spontaneous vaginal deliveries at Poole (P=0.007) and a 16.5% increase in the number of episiotomies in nulliparous operative vaginal deliveries in Hinchingbrooke (P=0.003). There was an overall 11% increase in episiotomy numbers in nulliparous vaginal deliveries (P=0.08). There was a statistically significant OASIS reduction of 84% in nulliparous spontaneous vaginal deliveries in women who received an episiotomy (P=0.003).
Conclusion
Initial results after introduction of EPISCISSORS-60® show that the majority of health care professionals achieve post-suturing episiotomy angles between 40° and 60°. The results also show a significant increase in the use of episiotomies in the delivery of nulliparous women. There has been a statistically significant reduction in OASIS in nulliparous spontaneous vaginal deliveries.
Keywords: EPISCISSORS-60®, episiotomy, obstetric anal sphincter injury, perineal body length, post-episiotomy suturing angle, nulliparous women
Introduction
The incidence of obstetric anal sphincter injuries (OASIS) in the UK is 6.1%1 and has tripled between 2000 and 2012.2 More importantly, OASIS are the most common risk factor for anal incontinence in women, which may affect up to 25% of women in the year following delivery.3 It has been shown that 30% of women are symptomatic for anal incontinence and urgency after 1 year.4
There are significant costs associated with OASIS. With 40,000 women affected per annum,5 the main cost is of course related to quality of life for the women involved. In financial terms, there are major cost implications for both primary and secondary repairs of OASIS. In addition, the National Health Service Litigation Authority (2012) in their report of 10 years of claims cite OASIS being the fourth largest cause for litigation in obstetrics.6
Research into the causes for OASIS has identified a number of risk factors. The Royal College of Obstetricians and Gynaecologists has listed the following risk factors for OASIS in its guideline for the management of third and fourth degree tears: Asian ethnicity, nulliparity, birth weight greater than 4 kg, shoulder dystocia, occipito-posterior position, prolonged second stage of labor, and instrumental delivery in which forceps carries a higher risk for OASIS than ventouse.7
Another factor not described in the Royal College of Obstetricians and Gynaecologists guideline but identified by a number of studies as a risk factor for OASIS is perineal body length (PBL).8–10 Measured as the length from the posterior fourchette to the midpoint of the anal canal, Deering et al11 found that patients with a PBL ≤25 mm had a significantly increased risk of having a delivery resulting in OASIS (40% versus 5.6%, P=0.004).
The ultimate aim of identifying risk factors is to reduce the incidence of OASIS. However, most risk factors are either not modifiable or have no alternative. For this reason, researchers have looked into other ways of reducing OASIS and the use of episiotomies has been one of the most prominent among these.
The role of episiotomy for prevention of OASIS is conflicting12–14 and is currently not routinely recommended for all deliveries. However, Gurol-Urganci et al2 looking at the Hospital Episode Statistics data for England over a 12-year period found that episiotomies were protective for OASIS. This effect was particularly present for instrumental deliveries but there was also a statistically significant OASIS reduction in primigravidas who had a normal vaginal delivery with an episiotomy.
A possible explanation for the conflicting evidence surrounding episiotomy may be related to operator technique. The type of episiotomy favored in England is a mediolateral episiotomy versus the midline episiotomy often used in the USA. It has long been known that mediolateral episiotomy has a significantly lower OASIS rate than midline episiotomies, 2% versus 12%–20%.15,16 Unfortunately, there is a lack of definition of the ideal angle of a mediolateral episiotomy and it is usually determined by the operator’s intent. However, the angle of mediolateral episiotomy turns out to be of crucial importance. It is important to notice here that, due to the way the perineum expands, there is a difference between the angle at which the episiotomy is cut and the post-suturing angle. Evidence has shown that incidence of OASIS is 10% with a post-suturing angle of 25° and reduces by 50% for every 6° the post-suturing angle is away from the midline. With a suture angle of 45°, the overall incidence is reduced to 0.5%.17 However, if the post-suturing angle is more than 60°, there is no protective effect as the episiotomy will have failed to relieve pressure from the perineum.18 In its 2007 guideline for intrapartum care, the National Institute for Health and Care Excellence states operators should aim to achieve an episiotomy angle between 45° and 60° at time of cutting. However, a 45° episiotomy angle at time of cutting achieves a post-suturing angle of 22°–24°. To achieve a post-suturing angle of 43°, the episiotomy needs to be cut at 60°.19 In addition, Stedenfeldt et al18 found that episiotomies are more effective when the cut is started away from the midline from posterior fourchette to the anal margin. For each 4.5 mm the episiotomy is started away from this line, OASIS reduce by 56%.
Hence, for an episiotomy to be effective, the angle and starting point are of critical importance. In view of this evidence, the recently published Royal College of Obstetricians and Gynaecologists Green Top Guideline 29 unequivocally recommends a 60° angled episiotomy at the time of cutting. The current method used by most clinicians is “eyeballing”. However, Andrews et al20 found that 0% midwives and 22% of doctors cut a truly mediolateral episiotomy between 40° and 60°. The inability to estimate angles accurately has been demonstrated in model situations as well with only 12%–15% clinicians cutting an episiotomy at the recommended angle.21,22
To avoid human error in estimating the angle required for mediolateral episiotomies, a team led by Professor Robert Freeman developed EPISCISSORS-60™ (Medinvent Ltd, Romsey, UK): episiotomy scissors especially designed to attain a post-suturing angle between 40° and 60° and achieve post-suture episiotomy 4.5 mm away from the midline. This patented product has a guide-limb that points toward the anus in the vertical plane and the scissors maintain a constant angle of 60° and 4.5 mm starting point away from the midline. In an initial trial of 17 women, Freeman et al19 demonstrated that the scissors consistently achieved a 43° post-suturing angle. Two subsequent studies have confirmed the efficacy of EPISCISSORS-60® in achieving these post-delivery suture angles.23,24
As part of a wider strategy to reduce OASIS, EPISCISSORS- 60® were introduced to clinical practice through a structured practical training program. This training program provides all midwives and doctors with a specific set of knowledge and skills to reduce OASIS. It includes teaching of the evidence based theoretical framework, practical teaching of measuring PBL, and training to cut true mediolateral episiotomies on a model using EPISCISSORS-60®. The decision when to perform an episiotomy lies with the operator. Two hospitals in the UK applied for an innovation fund grant to introduce and evaluate the effect of EPISCISSORS-60® on the incidence of OASIS through this program. Both hospitals are acute general hospitals with Hinchingbrooke Hospital in Cambridgeshire supporting 2,300 deliveries per annum and Poole hospital in Dorset just under 5,000. In the initial phase of this program, we focused on collecting and analyzing the data with regard to primigravidas as this is the group most at risk.
In this paper, we present our results with regard to PBL, uptake of episiotomy, post-suturing angles, and effect on OASIS based on our initial evaluation after 4 months of usage.
Methods
The Strategy for Using Practical aids for Prevention of OASIS, Recording episiotomies and clinician Training (SUPPORT©) program of all doctors and midwives at two sites commenced in December 2014. In January 2015, training of all medical staff had been completed and training of midwives continued until May 2015. Data were collected between January and May 2015. As part of the training program, whenever an episiotomy was deemed clinically indicated, EPISCISSORS-60® would be used. All episiotomies performed by trained operators in nulliparous women were included. The indication for episiotomy was left to the operators’ judgment. All deliveries were recorded onto the hospital record system immediately after the delivery. In addition, as part of the data collection, a standardized form was used for all deliveries on which the following would be recorded immediately after delivery: previous obstetric history, mode of delivery, first stage PBL, use of episiotomy, post-suturing episiotomy angle as measured from the midline, hands-on or hands-off delivery, occurrence of OASIS and which grade, type of operator, and feedback on EPISCISSORS-60® on a scale from 1 to 5 (very poor to very good). EPISCISSORS-60® were used for all deliveries and data with regard to use of episiotomy and OASIS were collected through the hospitals’ general data collection system and this database was used for the assessment of effect on OASIS. The results were compared with previous results obtained for the year 2014 from the hospitals’ database. This program was registered as a service evaluation and quality improvement process and approved by the audit and R&D department. Hence, no ethics approval was needed.
Results
Data were available for 197 nulliparous vaginal deliveries in Hinchingbrooke Hospital of which 137 were spontaneous vaginal deliveries (SVDs) and 60 operative vaginal deliveries (OVDs) and 641 nulliparous vaginal deliveries in Poole Hospital of which 452 were SVDs and 189 were OVDs (Table 1). Data collection forms were completed for 100 nulliparous vaginal deliveries and these formed the basis for our PBL measurements, post-episiotomy suturing angles, and user feedback.
Table 1.
Overview for 2014 and 2015 of total births, first births, episiotomy rates, and obstetric anal sphincter injuries (OASIS) rates for both spontaneous vaginal deliveries (SVDs) and operative vaginal deliveries (OVDs) in nulliparous (NP) women
| Hinchingbrooke 2014 |
Hinchingbrooke 2015 |
Poole 2014 |
Poole 2015 |
Combined 2014 |
Combined 2015 |
|
|---|---|---|---|---|---|---|
| Total births | 2,342 | 633 | 4,972 | 1,947 | 7,314 | 2,580 |
| All first births | 991/2,342 (42.3%) | 273 (43.1%) | 2,165 (43.5%) | 885 (45.4%) | 3,156 | 1,158 |
| NP (SVD + OVD) | 726 | 197 | 1,512 | 641 | 2,238 | 838 |
| OASIS in NP (SVD + OVD) | 52/726 (7.1%) | 12/197 (6%); 14% reduction | 107/1,512 (7%) | 37/641 (5.7%); 19% reduction | 159/2,238 (7.1%) | 49/838 (5.8%); 18% reduction; P=0.22 |
| OASIS in all NP | 52/991 (5.2%) | 12/273 (4.4%); 15.4% reduction; P=0.6 | 107/2,165 (4.9%) | 37/885 (4.2%); 16% reduction; P=0.4 | 159/3,156 (5%) | 49/1,158 (4.2%); 16% reduction; P=0.2 |
| Episiotomies in all NP | 289/991 (29.1%) | 83/273 (30%); ns | 503/2,165 (23%) | 238/885 (26.8%) | 792/3,156 (25%) | 321/1,158 (27.7%); 10.8% increase; P=0.08 |
| Episiotomies in NP (SVD + OVD) | 289/726 (39.8%) | 83/197 (42.1%) | 503/1,512 (33.3%) | 238/641 (37.1%) | 792/2,238 (35.3%) | 321/838 (38.3%); 8.5% increase; P=0.14 |
| OVD in NP | 239/991 (24%) | 60/273 (30.4%) | 428/2,165 (19.7%) | 189/885 (21.3%) | 667/3,156 (21.1%) | 249/838 (29.7%) |
| Episiotomies in OVD in NP | 203/239 (85%) | 59/60 (99%); 16.5% increase; ***P=0.003 | 380/428 (89%) | 164/189 (87%) | 583/667 (87.4%) | 223/249 (89.5%) |
| OASIS in OVD in NP | 18/239 (7.53%) | 4/60 (6.66%); 12% reduction; ns | 26/428 (6.07%) | 10/189 (5.29%); 12.8% reduction; P=0.85 | 44/667 (6.5%) | 14/249 (5.6%); 13.8% reduction; P=0.065 |
| OASIS in NP OVDs given episiotomies | 12/203 (5.9%) | 3/59 (5%); 15% reduction; P=1 | 25/380 (6.6%) | 9/164 (5.5%); 16.7% reduction; P=0.7 | 37/583 (6.3%) | 12/223 (5.4%); 14.2% reduction; P=0.7; RR=1.18 |
| OASIS in NP OVDs not given episiotomies | 6/36 (16.7%) | 1/1 (100%) | 1/48 (2%) | 1/25 (4%) | ||
| SVD in NP | 487 | 137 | 1,084 | 452 | 1,571 | 589 |
| OASIS in SVD in NP | 34 (7%) | 8 (5.8%); 17% reduction | 81 (7.47%) | 27 (5.97%); 20% reduction; P=0.32 | 115/1,571 (7.3%) | 35/589 (5.9%); 19% reduction in OASIS |
| OASIS in NP SVDs without episiotomy | 31/401 (7.7%) | 8/113 (7%); 9% reduction | 70/962 (7.27%) | 26/378 (6.87%); 5.5% reduction; ns | 101/1,363 (7.4%) | 34/491 (6.9%) |
| Episiotomies in NP SVDs | 86/487 (17.7%) | 24/137 (17.5%) | 122/1,084 (11.1%) | 74/452 (16.37%); 47% increase; ***P=0.007 | 208/1,571 (13.2%) | 98/589 (16.6%), 26% increase; ***P=0.04 |
| OASIS in NP SVDs given episiotomies | 2/86 (2.3%) | 0/24 (0%); 100% reduction; P=1 | 11/122 (9%) | 1/74 (1.35%); 85% reduction; ***P=0.03 | 13/208 (6.25%) | 1/98 (1%); 84% reduction; P=0.04 |
Notes: All P-values calculated by Fisher’s exact two-tailed test (GraphPad software, Inc., La Jolla, CA, USA). Bold values represent significant results.
Abbreviations: RR, risk ratio; ns, not significant.
PBL
PBL measurements are illustrated in Figure 1. Mean PBL was 37 mm in SVD (standard deviation [SD] =8.3, 95% confidence interval [CI] =34–39) and 38 mm in OVD (SD=8, 95% CI=35–40) groups. PBL in our sample showed a normal distribution and an average length which were very similar to that found in other studies.
Figure 1.
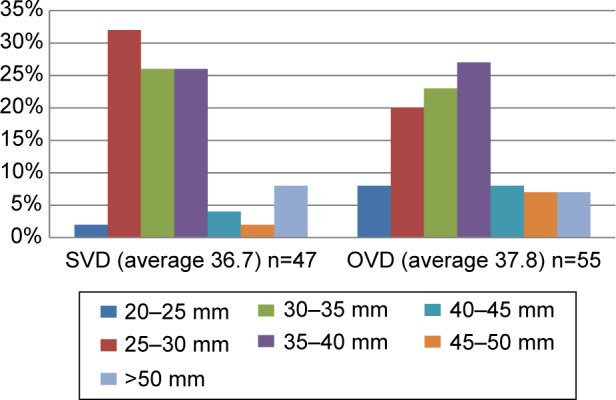
PBL distribution.
Abbreviations: PBL, perineal body length; SVD, spontaneous vaginal delivery; OVD, operative vaginal delivery.
Episiotomy angles
Post-suturing episiotomy angles were 53° (SD=6.5, 95% CI=50.7–55.8) in SVDs and 52° (SD=9.6, 95% CI=49–54) in OVDs. Post-episiotomy suturing angles are consistently within the safety zone between 40° and 60°. In all, 100% of midwives and 86% of doctors achieved a post-suture angle between 40° and 60° (Figure 2).
Figure 2.
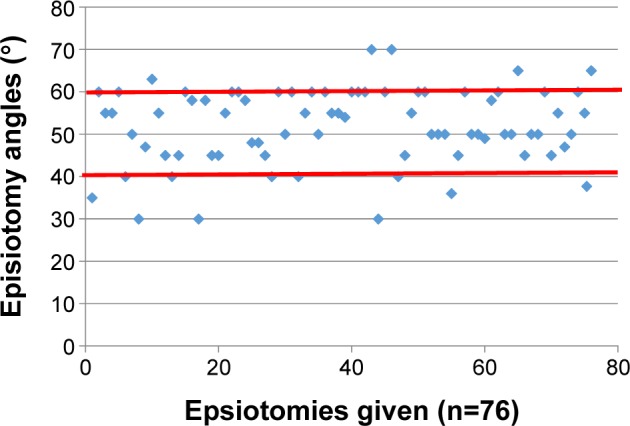
Distribution of post-suture episiotomy angles.
User feedback
User feedback with EPISCISSORS-60® was assessed on a scale from 1 to 5. Overall, 84% of users rated EPISCIS-SORS-60® as “good” to “very good” (Figure 3).
Figure 3.
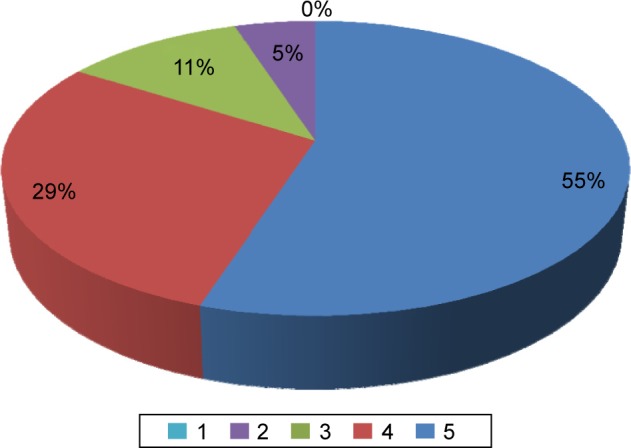
User feedback 1–5 (poor–very good), n=76.
Episiotomy usage
There was a 47% increase in the number of episiotomies in nulliparous SVDs at Poole compared to 2014 after the introduction of EPISCISSORS-60® (P=0.007) and a 16.5% increase in number of episiotomies in nulliparous OVDs in Hinchingbrooke compared to 2014 after introduction of EPISCISSORS-60® (P=0.003). There was an 11% increase in episiotomy numbers in nulliparous vaginal deliveries compared to 2014 after the introduction of EPISCISSORS-60® (P=0.08) (Figure 4).
Figure 4.
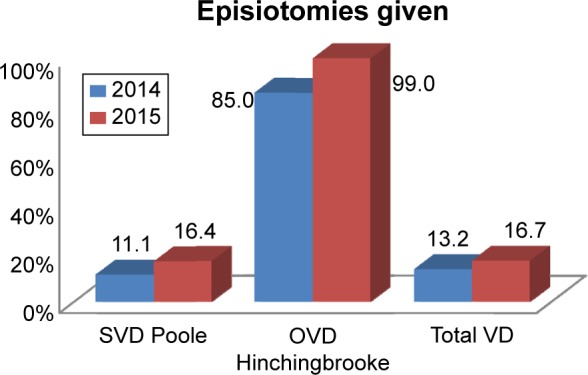
Significant changes in episiotomy numbers.
Abbreviations: SVD, spontaneous vaginal delivery; OVD, operative vaginal delivery; VD, vaginal delivery.
OASIS incidence
There was a 14.3% OASIS reduction in nulliparous OVDs given episiotomies compared to 2014 after the introduction of EPISCISSORS-60® (P=0.2, ns). There was an 84% OASIS reduction in nulliparous SVDs given episiotomies compared to 2014 after introduction of EPISCISSORS-60® (P=0.003). Overall, there was an 18% OASIS reduction in nulliparous vaginal deliveries compared to 2014 after the introduction of EPISCISSORS-60® (P=0.22, not significant). There was an 85% reduction in OASIS in nulliparous SVDs given episiotomy (1%) compared to those not given episiotomy (6.9%) in 2015 (P=0.01); risk ratio =0.15 (Figures 5 and 6).
Figure 5.
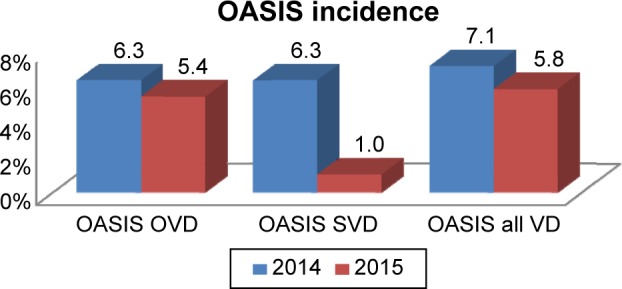
Incidence of OASIS before/after the introduction of EPISCISSORS-60®.
Abbreviations: OASIS, obstetric anal sphincter injuries; OVD, operative vaginal delivery; SVD, spontaneous vaginal delivery; VD, vaginal delivery.
Figure 6.
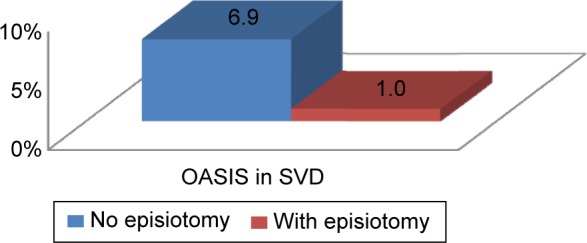
Obstetric anal sphincter injuries (OASIS) in spontaneous vaginal delivery (SVD): episiotomy versus no episiotomy.
Discussion
To the best of our knowledge, this is the first study to measure post-suture angles for episiotomies performed by a multidisciplinary cohort of health care professionals in a large group of primigravidas. After the introduction of EPISCISSORS-60®, we found that 86% of doctors and 100% of midwives were able to achieve post-suturing angles between 40° and 60°. This shows both a significant consistency and improvement over proportions reported in the literature. In addition, user feedback showed high rates of satisfaction in using EPISCISSORS-60® among all users.
In both hospitals, there was a significant increase in the usage of episiotomies in primigravidas. For Hinchingbrooke, there was a significant rise in episiotomies in OVD and in Poole, the main rise was seen in SVD. Of note is that episiotomy rates in SVD in Hinchingbrooke were higher to begin with and following the training, episiotomy rates are now comparable. It is not clear why in Hinchingbrooke the episiotomy rate in OVD has increased to a near 100% while in Poole there has been no further increase; perhaps, a larger data cohort will help us understand this increase.
The main objective of this entire program is to reduce OASIS. Despite the short period that the program has been in place and the relatively low number of cases, it is interesting that there has been a statistically significant reduction of 84% in OASIS in nulliparous SVDs given episiotomies compared to 2014 after the introduction of EPISCISSORS-60®. There has been a clinically significant OASIS reduction of 14.3% in nulliparous OVDs given episiotomies compared to 2014 and an overall reduction in OASIS in all vaginal deliveries of 18% compared to 2014 after the introduction of EPISCISSORS-60®. The program and data collection are ongoing and future analysis should show whether this reduction in OASIS is statistically significant. However, given the current incidences, it would take a sample size of 11,208 patients for it to reach statistical significance in nulliparous vaginal deliveries.
PBL was included as this is a factor known to be associated with OASIS and our data showed that population at both hospitals follow a normal distribution in keeping with findings from other studies and should therefore not be a factor in explaining any change in OASIS incidence.
The main limitation of this study is that the data presented were collected over a relatively short period of time of 4 months, and this may affect the statistical significance of some of our findings. However, some of the findings are felt to be clinically significant and worth sharing as part of our initial evaluation. We aim to continue long-term data collection and analyses with a view of reporting our findings in the future.
Finally, there appears to be reluctance among some midwives to perform episiotomies in general. Our data show that there is an 85% reduction in OASIS in nulliparous SVDs given episiotomy compared to those not given episiotomy. In terms of relative risk, this means nulliparous women not having an episiotomy at the time of delivery have a seven times increased risk of sustaining OASIS.
Conclusion
Initial results after the introduction of EPISCISSORS-60® in two hospitals in the UK show that the majority of health care professionals achieve appropriate post-suturing episiotomy angles between 40° and 60°. The user feedback has been very positive in the majority of cases. The results also show a significant increase in the use of episiotomies in the delivery of nulliparous women. Most importantly, there has been a statistically significant reduction in OASIS in nulliparous SVDs and a clinically significant reduction in OASIS in nulliparous operative deliveries. The data set is currently too small to achieve clinical significance and although data collection is ongoing, it may prove a challenge to achieve the numbers needed for statistical significance in the current setup. However, in a clinical sense, these findings are very encouraging. We acknowledge that a randomized controlled trial would provide the ultimate analysis of the effectiveness of EPISCISSORS-60®. However, the number of cases needed to achieve adequate power is over 21,000. This would cause substantial delay in addressing the clinically acute problem of ever rising OASIS rates. Finally, it has been shown that PBL, a possible cofounding factor for OASIS, follows a normal distribution in our population and does not account for the reduction of OASIS.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Thiagamoorthy G, Johnson A, Thakar R, Sultan AH. National survey of perineal trauma and its subsequent management in the United Kingdom. Int Urogynecol J. 2014;25(12):1621–1627. doi: 10.1007/s00192-014-2406-x. [DOI] [PubMed] [Google Scholar]
- 2.Gurol-Urganci I, Cromwell DA, Edozien LC, et al. Third- and fourth-degree perineal tears among primiparous women in England between 2000 and 2012: time trends and risk factors. BJOG. 2013;120:1516–1525. doi: 10.1111/1471-0528.12363. [DOI] [PubMed] [Google Scholar]
- 3.Zetterstrom J, López A, Anzén B, Norman M, Holmström B, Mellgren A. Anal sphincter tears at vaginal delivery: risk factors and clinical outcome of primary repair. Obstet Gynecol. 1999;94(1):21–28. [PubMed] [Google Scholar]
- 4.Oberwalder M, Connor J, Wexner SD. Meta-analysis to determine the incidence of obstetric anal sphincter damage. Br J Surg. 2003;90:1333–1337. doi: 10.1002/bjs.4369. [DOI] [PubMed] [Google Scholar]
- 5.Glazener CMA, Lang G, Wilson PD, Herbison GP, Macarthur C, Gee H. Postnatal incontinence: a multicentre randomised controlled trial of conservative management. Br J Obstet Gynaecol. 1998;105:47. [Google Scholar]
- 6.National Health Service Litigation Authority . Ten Years of Maternity Claims: An Analysis of NHS Litigation Authority Data. NHSLA; 2012. [Google Scholar]
- 7.RCOG Greentop guideline 29: The Management of Third- and Fourth-Degree Perineal tears: RCOG June 2015. Available from: www.rcog.org.uk.
- 8.Aytan H, Tapisiz OL, Tuncay G, Avsar FA. Severe perineal lacerations in nulliparous women and episiotomy type. Eur J Obstet Gynecol Reprod Biol. 2005;121:46–50. doi: 10.1016/j.ejogrb.2004.10.013. [DOI] [PubMed] [Google Scholar]
- 9.Rizk DE, Abadir MN, Thomas LB, Abu-Zidan F. Determinants of the length of episiotomy or spontaneous perineal lacerations during vaginal birth. Int Urogynecol J. 2005;16:395–400. doi: 10.1007/s00192-004-1273-2. [DOI] [PubMed] [Google Scholar]
- 10.Geller EJ, Robinson BL, Matthews CA. Perineal body length as a risk factor for ultrasound-diagnosed anal sphincter tear at first delivery. Int Urogynecol J. 2014;25:631–636. doi: 10.1007/s00192-013-2273-x. [DOI] [PubMed] [Google Scholar]
- 11.Deering SH, Carlson N, Stitely M, Allaire AD, Satin AJ. Perineal body length and lacerations at delivery. J Reprod Med. 2004;49:306–310. [PubMed] [Google Scholar]
- 12.Fritel X, Schaal JP, Fauconnier A, Bertrand V, Levet C, Pigné A. Pelvic floor disorders 4 years after first delivery: a comparative study of restrictive versus systematic episiotomy. BJOG. 2008;115:247–252. doi: 10.1111/j.1471-0528.2007.01540.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.De Vogel J, van der Leeuw-van Beek A, Gietelink D, et al. The effect of a mediolateral episiotomy during operative vaginal delivery on the risk of developing obstetrical anal sphincter injuries. Am J Obstet Gynecol. 2012;206:404.e1–e5. doi: 10.1016/j.ajog.2012.02.008. [DOI] [PubMed] [Google Scholar]
- 14.Räisänen S, Vehviläinen-Julkunen K, Heinonen S. Need for and consequences of episiotomy in vaginal birth: a critical approach. Midwifery. 2010;26:348–356. doi: 10.1016/j.midw.2008.07.007. [DOI] [PubMed] [Google Scholar]
- 15.Coats PM, Chan KK, Wilkins M, Beard RJ. A comparison between midline and mediolateral episiotomies. Br J Obstet Gynaecol. 1980;87:408–412. doi: 10.1111/j.1471-0528.1980.tb04569.x. [DOI] [PubMed] [Google Scholar]
- 16.Signorello LB, Harlow BL, Chekos AK, Repke JT. Midline episiotomy and anal incontinence: retrospective cohort study. BMJ. 2000;320(7227):86–90. doi: 10.1136/bmj.320.7227.86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Eogan M, Daly L, O’Connell PR, O’Herlihy C. Does the angle of episiotomy affect the incidence of anal sphincter injury? BJOG. 2006;113:190–194. doi: 10.1111/j.1471-0528.2005.00835.x. [DOI] [PubMed] [Google Scholar]
- 18.Stedenfeldt M, Pirhonen J, Blix E, Wilsqaard T, Vonen B, Qian P. Episiotomy characteristics and risks for obstetric anal sphincter injury: a case-control study. BJOG. 2012;119:724–730. doi: 10.1111/j.1471-0528.2012.03293.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Freeman RM, Hollands HJ, Barron LF, Kapoor DS. Cutting a mediolateral episiotomy at the correct angle: evaluation of a new device: the episcissors-60. Med Devices (Auckl) 2014;7:23–28. doi: 10.2147/MDER.S60056. eCollection 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Andrews V, Thakar R, Sultan AH, Jones PW. Are mediolateral episiotomies actually mediolateral? BJOG. 2005;112:1156–1158. doi: 10.1111/j.1471-0528.2005.00645.x. [DOI] [PubMed] [Google Scholar]
- 21.Naidu M, Kapoor DS, Evans S, Vinayakarao L, Thakar R, Sultan AH. Cutting an episiotomy at 60 degrees: how good are we? Int Urogynecol J. 2015;26(6):813–816. doi: 10.1007/s00192-015-2625-9. Epub 2015 Feb 6. [DOI] [PubMed] [Google Scholar]
- 22.Silf K, Woodhead N, Kelly J, Fryer A, Kettle C, Ismail KM. Evaluation of accuracy of mediolateral episiotomy incisions using a training model. Midwifery. 2015;31(1):197–200. doi: 10.1016/j.midw.2014.08.009. Epub 2014 Sep 2. [DOI] [PubMed] [Google Scholar]
- 23.Patel RP, Ubale SM. Evaluation of the angled Episcissors-60® epi-siotomy scissors in spontaneous vaginal deliveries. Med Devices (Auckl) 2014;7:253–256. doi: 10.2147/MDER.S66901. Published online 2014 Jul 31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sawant G, Kumar D. Randomized trial comparing episiotomies with Braun-Stadler episiotomy scissors and EPISCISSORS-60®. Med Devices (Auckl) 2015;8:251–254. doi: 10.2147/MDER.S83360. Published online 2015 Jun 1. [DOI] [PMC free article] [PubMed] [Google Scholar]