

Abstract:
There is a considerable amount of literature published on the detrimental effects of banked blood exposure in cardiac surgery. Likewise, in an effort to minimize blood exposure, many of these articles involve modifications to the heart-lung machine or its components to reduce priming volumes, therefore decreasing the need for banked blood administration caused by hemodilution. In this study, using Terumo’s System 1 Advanced Heart-Lung machine, all the pump heads were remotely mounted off the pump base closer to the patient and to all the pump components. For example, cardioplegia, ultrafiltration, and vent and cardiotomy lines are now close to the oxygenator and to the patient, minimizing any excess tubing length. Cardiopulmonary bypass (CPB) blood use and priming volumes were compared before and after changing from a fixed perfusion system to a remote-mounted perfusion system using the same disposables and protocols. The mean differences of pump prime and CPB blood use were compared in four weight classes. In the 8- to 12-kg class, blood use was reduced from 1.84 ± 0.55 to 1.10 ± 0.36 units. Priming volume was reduced from 751.2 ± 68.4 to 360.4 ± 51.7 mL. In the 13- to 20-kg class, blood use was reduced from 1.80 ± 0.42 to 1.04 ± 0.28 units. Priming volume was reduced from 829.6 ± 69.6 to 476.± 81.4 mL. In the 21- to 40-kg class, blood use was reduced from 1.60 ± 0.57 to 0.92 ± 0.49 units. Priming volume was reduced from 994.0 ± 137.2 to 713.6 ± 121.8 mL. In the 41+-kg class, blood use was reduced from 1.62 ± 0.88 to 0.42 ± 0.54 units. Priming volume reduced from 1306.3 ± 112.9 to 875.5 ± 96.6 mL. In conclusion, using a remote-mounted perfusion system resulted in reducing priming volumes and also significantly decreased the need for banked blood, subsequently saving the patient excessive exposure to banked blood.
Keywords: cardiopulmonary bypass, cardiopulmonary bypass equipment, blood conservation, blood transfusion, pediatric
The current trend in perfusion and cardiac surgery is focusing on cardiopulmonary bypass (CPB) circuit miniaturization and blood conservation. The scientific literature has well documented the inherent adverse effects of the CPB circuit, such as increased inflammatory response, harmful hemodilutional effects, coagulopathies, and systemic organ dysfunction, in its relation to the patient being exposed to a large foreign surface area and subsequent sizable priming volume (1–4). Blood conservation is also being supported because of a considerable amount of literature published on the detrimental effects of banked blood exposure during cardiac surgery, such as impairing microcirculation, limited oxygen release, and, most recently, decreased patent survival (5–8). Therefore, in an effort to minimize blood exposure and the adverse effects of being exposed to the CPB circuit, many scientific articles involving modifications to the heart-lung machine and its CPB circuit components have been published (9–12). This study describes the advantage of changing the physical setup of a remote-mounted CPB circuit, not only to cut down on the tubing surface area from pump to patient (Figures 1 and 2) but also between the individual components of the setup (Figure 3). The focus of this study is to show the difference in priming volume and blood use between the Sarns 9000 fixed pump head configuration (fixed group) and the Terumo System 1 remote-mounted pump head configuration (remote group).
Figure 1.
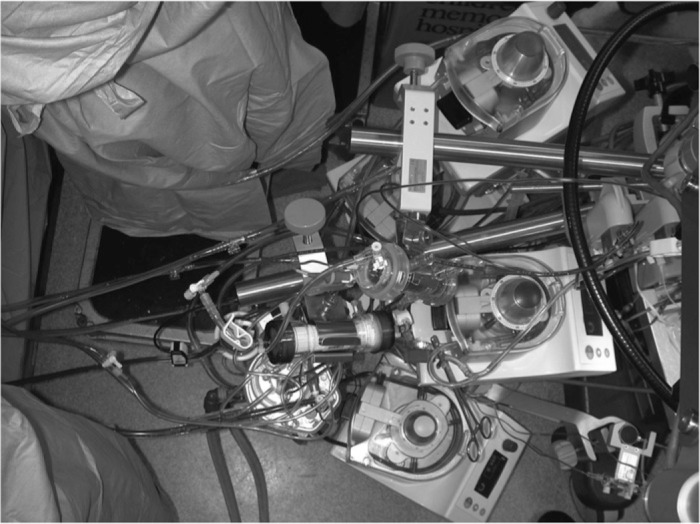
Remote-mounted pump system in close proximity to patient.
Figure 2.
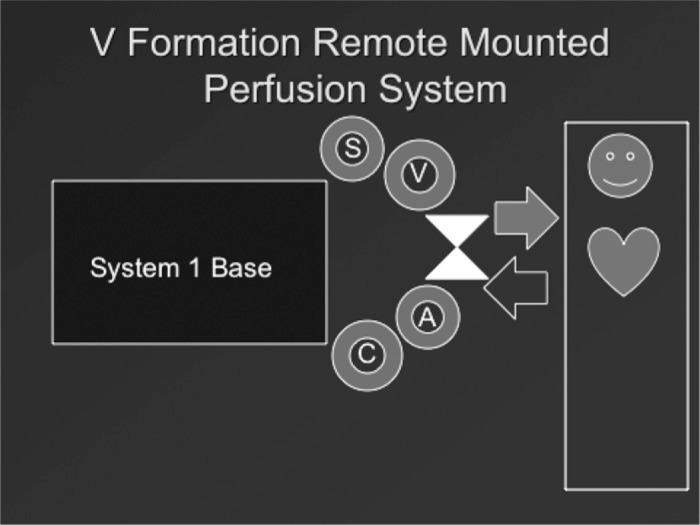
Drawing of remote-mounted perfusion system. A, arterial pump head; C, cardioplegia pump head; V, vent pump head; S, dual cardiotomy suction pump head.
Figure 3.

View of remote-mounted components.
MATERIALS AND METHODS
Equipment
The equipment compared were a Terumo System 1 Advanced Heart Lung Machine (Terumo Cardiovascular Systems, Ann Arbor, MI) vs. the Sarns 9000 Heart Lung Machine (Sarns 3M, Ann Arbor, MI). The four custom tubing sets and components used were as follows:
8- to 12-kg group: Capiox SX05W (Terumo Cardiovascular Systems), ¼ × ¼ custom tubing set (Terumo Cardiovascular Systems), CP-50 cardioplegia set (Terumo Cardiovascular Systems), HPH 400TS (Hemocor HPH; Minntech, Minneapolis, MN), and AF-02 arterial filter (Terumo Cardiovascular Systems).
13- to 20-kg group: Capiox 15W30RX (Terumo Cardiovascular Systems) ¼ × ⅜ custom tubing set (Terumo Cardiovascular Systems), CP-50 cardioplegia set (Terumo Cardiovascular Systems), HPH 400TS (Hemocor HPH; Minntech), and AF-02 arterial filter (Terumo Cardiovascular Systems).
21- to 40-kg group: Capiox 15W30RX (Terumo Cardiovascular Systems), ⅜ × ⅜ custom tubing set (Terumo Cardiovascular Systems), CP-50 cardioplegia set (Terumo Cardiovascular Systems), HPH 400TS (Hemocor HPH; Minntech), and AF-125 arterial filter (Terumo Cardiovascular Systems).
41+-kg group: Capiox 15W40RX (Terumo Cardiovascular Systems), ⅜ × ½ custom tubing set (Terumo Cardiovascular Systems), CP-50 cardioplegia set (Terumo Cardiovascular Systems), HPH 400TS (Hemocor HPH, Minntech), and AF-125 arterial filter (Terumo Cardiovascular Systems).
All remote pumps were mounted on Terumo roller pump pole mounts and brackets (Terumo Cardiovascular Systems). Adaptations to component holders were custom made by Bradley Kulat, CCP, LP, and Neale Zingle, CCP, LP (Children’s Memorial Hospital, Chicago, IL).
Description of Technique
Using remote mounting plates, all of the pump heads were placed in a V-shaped pattern off the left side of the System 1 heart-lung machine (Figures 1 and 2). The apex of the V pattern, which is formed by the remotely mounted pump heads, is where the oxygenator and arterial filter would be in the center of each of the “wings” of the V pattern. The “wings” of the V pattern are formed by two pump heads on each side of the oxygenator. The left arm of the V pattern would house the arterial pump head and cardioplegia pump head and the right arm of the V pattern would house the vent and double cardiotomy pump heads (Figures 1 and 2). Creative adaptations were needed to suspend disposable components, such as the cardioplegia and hemoconcentrator close to the remote-mounted circuit and pump heads. This was done by cutting a mast in half and fixing it horizontally to the vertical mast of the heart-lung machine (Figure 1). Our cardioplegia and hemoconcentrator were mounted close to the circuit with minimum tubing length. The oxygenator bracket was slightly modified to extend this unit further out from the pump. The heart-lung machine will be pulled up at a right angle to the surgical table with the tip of the V pattern as close to the table as possible (Figures 1 and 2).
Methods
Circuit volumes and CPB blood use were compared in the Sarns 9000 fixed roller pump heart-lung machine and the Terumo System 1 remote-mounted pump head heart-lung machine. Two hundred similar weight class patients (50 patients per group) were randomly and retrospectively sampled using the Sarns 9000 fixed roller pump, and 200 similar weight class patients (50 patients per group) using the remote-mounted Terumo System 1 were also randomly and retrospectively sampled. The weight classes are broken into the four weight classes that follow tubing pack sizes. Volumes stated are from a static prime in milliliters. Blood use is reported for only CPB use in units. Surgical, anesthesia, perfusion protocols, and aprotinin use remained consistent throughout the study. Percent average changes, SD, and p values were calculated and are reported between each fixed pump group and remote pump group as shown in Table 1.
Table 1.
Comparison of blood use and priming volume by fixed and remote-mounted classes divided into similar weight groups.
| Blood in Units |
Prime (mL) |
|||||||
|---|---|---|---|---|---|---|---|---|
| Weight Group | Fixed | Remote | Percent Change | p | Fixed | Remote | Percent Change | p |
| 8–12 kg | 1.84 ± .55 | 1.1 ± .36 | −40 | 1.6 E–12 | 751.2 ± 68.4 | 360.4 ± 51.7 | −52 | 3.3 E–54 |
| 13–20 kg | 1.8 ± .42 | 1.04 ± .28 | −44 | 1.0 E–17 | 829.6 ± 69.6 | 476 ± 8.14 | −43 | 4.9 E–52 |
| 21–40 kg | 1.6 ± .57 | .92 ± .49 | −43 | 2.7 E–09 | 994 ± 137.2 | 713.6 ± 121.8 | −28 | 1.1 E–18 |
| ≥41 kg | 1.62 ± .88 | .42 ± .54 | −74 | 3.9 E–13 | 1306.3 ± 112.9 | 875.5 ± 96.6 | −33 | 1.6 E–37 |
RESULTS
There were 400 patients that were randomly and retrospectively reported in this study (Table 1). CPB blood use and priming volumes were compared before and after changing from a fixed perfusion system to a remote-mounted perfusion system using the same disposables and protocols. Because this remote-mounted system is being used in a pediatric institution, the differences of pump prime and CPB blood use were compared in four weight classes. In the 8- to 12-kg class of patients, blood use was decreased from a mean of 1.84 ± .55 units in the fixed group to a mean of 1.10 ± .36 units (p = 1.6) in the remote group, and priming volume was reduced from a mean of 751.2 ± 68.4 mL in the fixed group to a mean of 360.4 ± 51.7 mL (p = 3.3) in the remote gxroup. In the 13- to 20-kg class of patients, blood use was reduced from a mean of 1.80 ± 0.42 units in the fixed group to a mean of 1.04 ± 0.28 units (p = 1.0) in the remote-mounted group, and priming volume was reduced from a mean of 829.6 ± 69.6 mL in the fixed group to a mean of 476 ± 81.4 mL (p = 4.9) in the remote group of patients. In the 21- to 40-kg class of patients, blood use was reduced from a mean of 1.60 ± .57 units in the fixed group to a mean of .92 ± .49 units (p = 2.7) in the remote group, and priming volumes were reduced from 994.0 ± 137.2 mL in the fixed group to a mean of 713.6 ± 121.8 mL (p = 1.1) in the remote group of patients. Last, blood use was reduced from a mean of 1.62 ± .88 units in the fixed group to a mean of .42 ± .54 units (p = 3.9) in the remote group, and priming volume reduced from a mean of 1306.3 ± 112.9 mL in the fixed group to a mean of 875.5 ± 96.6 mL (p = 1.6) in the remote group for the 41+-kg patient class.
DISCUSSION
The current trend in cardiac surgery that requires the use of a CPB circuit is leading us into the era of circuit miniaturization and blood conservation. These trends have become very hot topics, not only in pediatric perfusion circles but also with the adult perfusion community. Current methods to miniaturize CPB circuits include using patient specific components and tubing, low prime/high efficiency oxygenators and components, and, to lesser extent, changing the physical setup of the CPB circuit by using a remote-mounted perfusion system. Manufacturers are listening to the perfusion communities’ needs and are becoming more aware of developing smaller and more efficient disposable products. However, manufacturers are still lagging behind in heart-lung machine design. With the exception of a few manufacturers, perfusionists are given no choice or flexibility to where the pump heads can be placed. Thus, this severely limits the clinician’s efforts to minimize the CPB circuit. In this study, using Terumo’s System 1 Advanced Heart-Lung machine, all of the pump heads were remotely mounted off the pump base closer to the patient. This method also allowed for all the pump components to move closer together; for example, the cardioplegia, ultrafiltration unit, and vent and cardiotomy lines are close to the oxygenator and patient, minimizing any excess tubing length. The manufacturer’s remote mounting plates were used for remotely mounting the pump heads; however, some creative adaptations were also used to modified component holders and masts to mount disposables closely to the remotely mounted circuit. Remote mounting of pump heads using the manufacturer’s mounting plates did require an additional expense to the cost of the perfusion system.
The focus of this study was to show that a remote-mounted perfusion system could be used to reduce exposure to an excessive CPB surface area and therefore reduce pump priming volumes and blood use. As this study shows, the flexibility and versatility of a remote-mounted perfusion system can be another tool for the clinician to use in decreasing the surface area of their CPB circuit, thus decreasing the patient’s exposure to the foreign CPB circuit, decreasing priming volume, and decreasing the dependence on banked blood. This study also reflects that, without changing any other CPB priming variable, a remotely mounted perfusion system made a considerable impact on priming volume and banked blood use. The smallest weight class of patients (1.6–7 kg) was excluded from this study because of a tubing pack change not used with the fixed Sarns 9000 group. Priming volumes and blood use significantly decreased in all weight groups without compromising user friendliness and, most importantly, patient safety.
ACKNOWLEDGMENTS
This project could not have been completed without the clinical input and the statistical advice of Steven Moss, CCP. We thank the surgical staff of the Division of Cardiovascular-Thoracic Surgery at Children’s Memorial Hospital and Drs Constantine Mavroudis, Carl Backer, and Sunjay Kaushal for their patience and trust. We also thank Sean McKenna and Melanie Gevitz for their technical support and wisdom.
REFERENCES
- 1.Kirklin JK, Westaby SS, Blackstone EH, Kirklin JW, Chenoowith DE, Pacifico AD.. Complement and the damaging effects of cardiopulmonary bypass. J Thorac Cardiovasc Surg. 1983;86:845–57. [PubMed] [Google Scholar]
- 2.Kozik DJ, Tweddell JS.. Characterizing the inflammatory response to cardiopulmonary bypass in children. Ann Thorac Surg. 2006;81(Suppl):S2347–54. [DOI] [PubMed] [Google Scholar]
- 3.Shann KG, Likosky DS, Murkin JM, et al. An evidence-based review of the practice of cardiopulmonary bypass in adults: a focus on neurologic injury, glycemic control, hemodilution, and the inflammatory response. J Thorac Cardiovasc Surg. 2006;132:283–90. [DOI] [PubMed] [Google Scholar]
- 4.Habib RH, Zacharias A, Schwann TA, Riordan CJ, Durham SJ, Shah A.. Adverse effects of low hematocrit during cardiopulmonary bypass in the adult: should current practice be changed? J Thorac Cardiovasc Surg. 2003;125:1438–50. [DOI] [PubMed] [Google Scholar]
- 5.The Society of Thoracic Surgeons Blood Conservation. Perioperative blood transfusion and blood conservation in cardiac surgery: The Society of Thoracic Surgeons and The Society of Cardiovascular Anesthesiologists Clinical Practice Guideline. Ann Thorac Surg. 2007;83(5 Suppl):S27–86. [DOI] [PubMed] [Google Scholar]
- 6.Koch CG, Li L, Duncan AI, et al. Transfusion in coronary artery bypass grafting is associated with reduced long-term survival. Ann Thorac Surg. 2006;81:1650–7. [DOI] [PubMed] [Google Scholar]
- 7.Koch CG, Khandwala F, Li L, Estafanous FG, Loop FD, Blackstone EH.. Persistent effect of red cell transfusion on health-related quality of life after cardiac surgery. Ann Thorac Surg. 2006;82:13–20. [DOI] [PubMed] [Google Scholar]
- 8.Speiss BD.. Transfusion and outcome in heart surgery. Ann Thorac Surg. 2002;74:986–7. [DOI] [PubMed] [Google Scholar]
- 9.Ando M, Takahashi Y, Suzuki N.. Open heart surgery for small children without homologous blood transfusion by using remote pump head system. Ann Thorac Surg. 2004;78:1717–22. [DOI] [PubMed] [Google Scholar]
- 10.Abdel-Rahman U, Özaslan F, Risteski PS, et al. Initial experience with a minimized extracorporeal bypass system: Is there a clinical benefit? Ann Thorac Surg. 2005;80:238–43. [DOI] [PubMed] [Google Scholar]
- 11.Hickey E, Karamlou T, You J, Ungerleider RM.. Effects of circuit miniaturization in reducing inflammatory response to infant cardiopulmonary bypass by elimination of allogeneic blood products. Ann Thorac Surg. 2006;81:S2367–72. [DOI] [PubMed] [Google Scholar]
- 12.Immer FF, Ackermann A, Gygax E, et al. Minimal extracorporeal circulation is a promising technique for coronary artery bypass grafting. Ann Thorac Surg. 2007;84:1515–21. [DOI] [PubMed] [Google Scholar]