

Abstract
Acetabular chondral carpet delamination is a frequent finding at hip arthroscopy. The cartilage is macroscopically normal but deboned from the subchondral bone, without a disruption at the chondrolabral junction. Arthroscopic anatomic repair of delaminated cartilage is challenging. We propose that a combination of microfracture and use of stitches to press the delaminated cartilage against the subchondral bone using a suture limb offers an effective method to provide an environment for cartilage repair. This article describes the technique of bridging suture repair for carpet delamination in detail; the technique enables the surgeon to stabilize the delaminated acetabular cartilage. Intra-articular soft anchors and an acetabular rim knotless anchor footprint provide a stable repair for delaminated cartilage. This technique is especially helpful in cases with acetabular cartilage carpet delamination.
Acetabular chondral carpet delamination is a frequent finding at hip arthroscopy.1 This debonding injury presents as a wave sign without a disruption at the chondrolabral junction. The cartilage is macroscopically normal but disrupted from the subchondral bone.2 Carpet delamination in the hip is believed to be one of the sources of hip pain and the earliest visible sign of osteoarthritis.3, 4 Histologic studies of delaminated hyaline cartilage have shown the presence of viable chondrocytes.2 Therefore it is logical to attempt to repair the delaminated cartilage from the standpoints of both pain relief and prevention of osteoarthritis. However, arthroscopic anatomic repair of delaminated cartilage is technically difficult.
Although successful surgical treatment of femoroacetabular impingement has been described in reports from several centers,5, 6, 7 acetabular cartilage delamination is often associated with failure.6 Thus there remains a strong motivation to develop an effective surgical procedure for acetabular chondral carpet delamination. Villar and colleagues3, 4 reported excellent early clinical results for arthroscopic repair of carpet delamination using fibrin glue.
We report a bridging suture technique to repair acetabular cartilage carpet delamination. Our technique involves a combination of microfracture and use of stitches to press the delaminated cartilage firmly against the subchondral bone. This provides an environment for repair and regeneration of cartilage at an early stage in an attempt to retain and salvage native tissue.
Surgical Procedure
Operating Room Preparation
Hip arthroscopy is performed in the usual fashion. Our preference is to perform this with the patient in the supine position. A standard fluoroscope is used during portal placement, labral repair, and bony debridement. Proper anesthesia with paralysis is necessary for safe distraction of the hip joint and prevention of complications during hip arthroscopy. The patient is placed on a fracture table with a well-padded perineal post. The operative extremity is positioned in adduction, with the hip flexed to 10° and the femur internally rotated.
Portal Placement
Traction is applied to the hip. A 14-gauge needle and nitinol wire are then used to create an anterolateral portal. A 70° arthroscope is introduced into the hip joint through the anterolateral portal. Dry arthroscopy of the hip is used to create a midanterior portal by use of an outside-in technique. The midanterior portal is placed at an approximately 45° angle anterior to the anterolateral portal. The 14-gauge needle and nitinol wire are then advanced into the joint, adjacent to the labrum, through the anterior capsule. A 5-mm cannula is used to introduce a Beaver blade (Smith & Nephew, Andover, MA), and a capsulotomy is performed. After the portals have been established, the surgeon performs diagnostic arthroscopy, switching portals frequently to access all parts of the joint.
Repair of Acetabular Cartilage Carpet Delamination
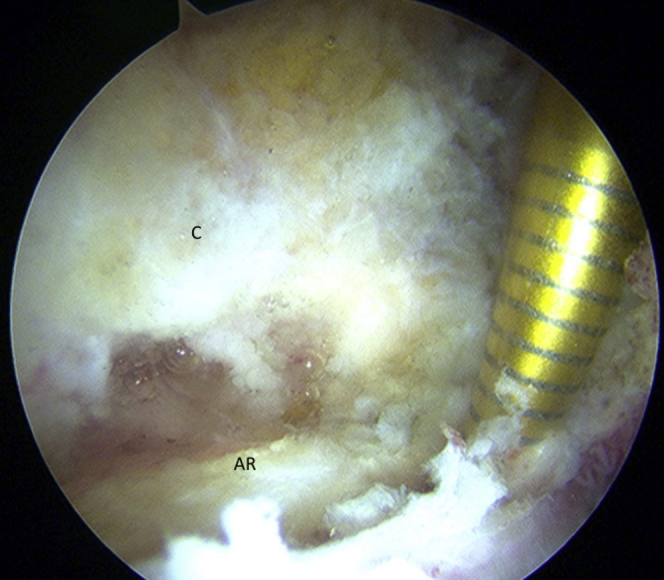
A positive “carpet phenomenon” or “wave sign” at the chondrolabral junction indicates delamination of the articular cartilage from the subchondral bone (Video 1). To gain access to the area behind the delaminated cartilage, we make a small incision on the outer part of the acetabular labrum, immediately at the acetabular margin, and then develop the sulcus using a liberator but are careful not to further damage the overlying delaminated cartilage (Fig 1). An awl can then be passed through this incision to the pocket, and microfracture is performed (Fig 2).
Fig 1.

The surgeon creates a sulcus using a liberator, ensuring not to further damage the overlying delaminated cartilage. View of right hip, with camera positioned in anterolateral portal. (AL, acetabular labrum; AR, acetabular rim; C, capsule.)
Fig 2.
Microfracture is performed using an awl to generate an environment for repair and regeneration of cartilage. View of right hip, with camera positioned in anterolateral portal. (AR, acetabular rim; C, capsule.)
Two soft anchors are placed at the peripheral ends of the delaminated cartilage in the medial acetabulum (Fig 3). We use a 1.4-mm single-loaded JuggerKnot suture anchor (Biomet, Warsaw, IN). A curved drill guide is used to gain access to the lesion. Four limbs of suture are then passed through the labrum in a piercing fashion with a small suture passer (Arthropierce; Smith & Nephew, Andover, MA) (Fig 4). Next, a pilot hole for a 4.75-mm fully threaded SwiveLock anchor (Arthrex, Naples, FL) is drilled in the planned location. Pilot holes should be drilled 1 to 2 mm proximal to the acetabular rim, which prevents acetabular penetration but still allows for re-creation of a smooth transition between the articular cartilage and the labrum. A pilot hole is drilled while the surgeon is directly visualizing the acetabular articular cartilage and then is double-checked for penetration (acetabular or intrapelvic) and for correct positioning by palpation with a nitinol wire and by fluoroscopy. A SwiveLock anchor is then used to secure both limbs of the JuggerKnot into the predrilled pilot hole. Tensioning of each suture limb independently during SwiveLock anchor placement controls the ultimate tension within the repaired labrum, as well as the orientation of the labrum on the acetabular rim (Fig 5). It is important not to overtension the suture because this may significantly evert the labrum and prevent formation of a suction seal once the femoral head is reduced. Once the labral repair is completed, the traction is released and the apposition between the repaired labrum and the femoral head is evaluated while the surgeon is viewing from the peripheral compartment (Fig 6). The capsulotomy is then closed using an Accu-Pass device (Smith & Nephew) by passing a No. 2 Vicryl suture (Ethicon, Somerville, NJ) and tying a racking half-hitch knot. Table 1 presents the key points of the intra-articular soft anchor fixation for acetabular chondral carpet delamination.
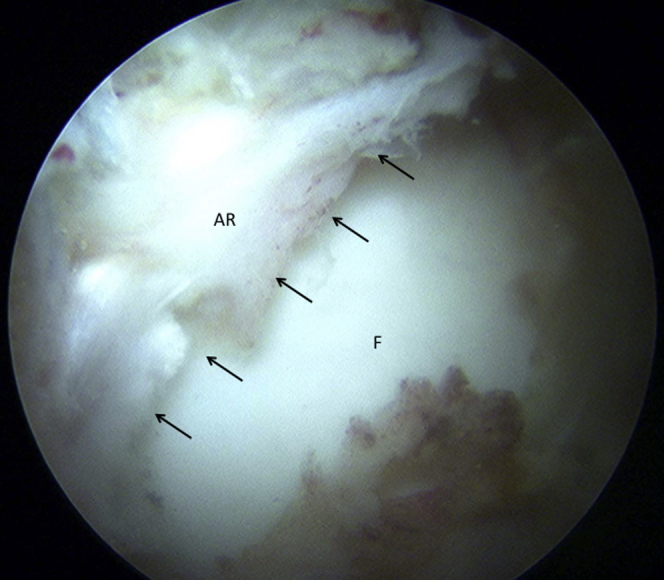
Fig 3.
Two soft anchors are placed at the peripheral ends of the delaminated cartilage (arrows) in the medial acetabulum. A curved drill guide is used to gain access to the lesion. View of right hip, with camera positioned in anterolateral portal. (AL, acetabular labrum; CD, carpet delamination; F, femoral head.)
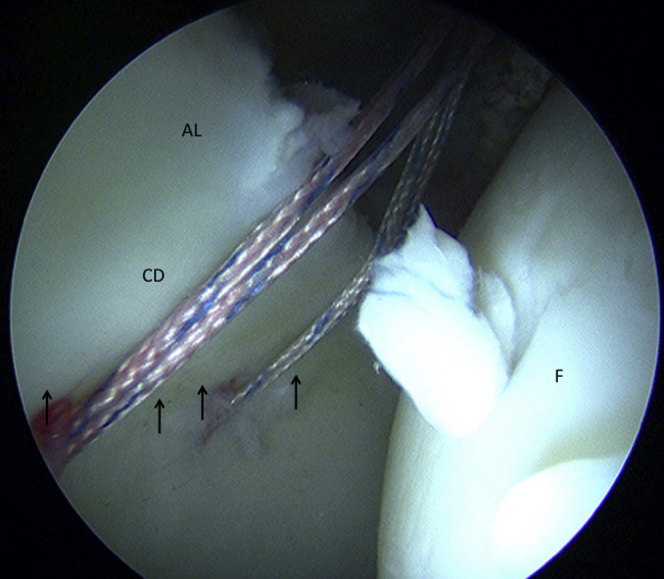
Fig 4.

Four limbs of suture are passed through the labrum in a piercing fashion with a suture passer. The arrows indicate the peripheral ends of the delaminated cartilage. View of right hip, with camera positioned in anterolateral portal. (CD, carpet delamination; F, femoral head).
Fig 5.

A threaded knotless anchor is used to secure both limbs of the sutures into a predrilled pilot hole on the extra-articular side of the acetabular rim. View of right hip, with camera positioned in anterolateral portal.
Fig 6.
Without traction, the hip is taken through a dynamic examination to verify that the labrum sits on the femoral head to provide a suction seal (arrows). View of right hip, with camera positioned in midanterior portal. (AR, acetabular labrum; F, femoral head.)
Table 1.
Pearls and Key Points
| Adequate distraction of the hip joint is necessary to ensure safe insertion of soft anchors in the medial acetabulum. |
| The surgeon should appropriately select patients with carpet delamination without chondrolabral disruption. |
| Microfracture is performed to provide an environment for repair and regeneration of cartilage. |
| Soft anchors are placed at the peripheral ends of the delaminated cartilage in the medial acetabulum. |
| A threaded knotless anchor is used to secure the suture limb, which enables the delaminated cartilage to be pressed against the subchondral bone. |
Postoperative Rehabilitation
In general, patients are advised to maintain 50% partial weight bearing for 4 weeks. Extreme external hip rotation and passive hip extension are limited in the first 2 weeks postoperatively, primarily to protect the capsular repair, but no braces or rotational control boots are used. When the patient is fully weight bearing and achieves a full range of motion, therapy is advanced. Gentle strengthening exercises begin with a stationary bicycle and isometrics. As strengthening progresses, patients start using an elliptical machine and slide board and perform hip girdle strengthening. When the range of motion and strength are satisfactory, patients begin sport-specific training.
Discussion
The described technique provides a safe and simplified method for arthroscopic repair of acetabular chondral carpet delamination. Cartilage delamination in the hip is a source of hip pain. Generally, anatomic repair of delaminated cartilage is not a common procedure. Persistent hip pain is often observed even after hip arthroscopy in patients with acetabular cartilage delamination. The described intervention is intended to achieve rigid stability of the delaminated acetabular cartilage. Using the stitches to press the delaminated cartilage enables stabilization of the delaminated acetabular cartilage against the subchondral bone. This is one of the main advantages of our technique, and the early clinical results have shown excellent pain relief. It is also logical to attempt to repair the delaminated cartilage to prevent the progression of osteoarthritis. The main disadvantage of this method is the necessity of inserting the suture anchors in the medial acetabulum, which may induce iatrogenic damage to the acetabular cartilage (Table 2). To minimize the risk of iatrogenic cartilage injury, we used soft anchors. A curved drill guide also helps to reduce the risk of cartilage injury.
Table 2.
Risks and Avoidance Pitfalls
| The technique is technically demanding. |
| There is a theoretical risk of iatrogenic injury to the acetabular cartilage. |
| Soft anchors are useful to reduce the risk of iatrogenic cartilage injury. |
| Caution must be used while drilling to generate the anchor hole and placing the soft anchor. A curved guide is helpful. |
We advocate the use of bridging suture repair for carpet delamination where possible because of the strong mechanical and biological advantage offered in the repair of acetabular cartilage delamination. In our experience with this technique, we have not encountered any complications. This technique is especially helpful to the surgeon when trying to repair acetabular cartilage carpet delamination.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Technique for bridging suture repair for acetabular cartilage carpet delamination. The patient is in the prone position. A right hip is shown, with the camera positioned in the anterolateral portal.
{kind=link}
References
- 1.Larson C.M., Stone R.M., Wulf C.A. Hip arthroscopy: Management of chondral injuries. In: Byrd J.W.T., editor. Operative hip arthroscopy. Springer Science + Business Media; New York: 2013. pp. 185–196. [Google Scholar]
- 2.Hembree W.C., Ward B.D., Furman B.D. Viability and apoptosis of human chondrocytes in osteochondral fragment following joint trauma. J Bone Joint Surg Br. 2007;89:1388–1395. doi: 10.1302/0301-620X.89B10.18907. [DOI] [PubMed] [Google Scholar]
- 3.Stafford G.H., Bunn J.R., Villar R.N. Arthroscopic repair of delaminated acetabular articular cartilage using fibrin adhesive. Results at one to three years. Hip Int. 2011;21:744–750. doi: 10.5301/HIP.2011.8843. [DOI] [PubMed] [Google Scholar]
- 4.Tzaveas P., Villar R.N. Arthroscopic repair of acetabular chondral delamination with fibrin glue adhesive. Hip Int. 2010;20:115–119. doi: 10.1177/112070001002000117. [DOI] [PubMed] [Google Scholar]
- 5.Philippon M.J., Weiss D.R., Kuppersmith D.A., Briggs K.K., Hay C.J. Arthroscopic labral repair and treatment of femoroacetabular impingement in professional hockey players. Am J Sport Med. 2012;38:99–104. doi: 10.1177/0363546509346393. [DOI] [PubMed] [Google Scholar]
- 6.Byrd L.W.T., Jones K.S. Arthroscopic management of femoroacetabular impingement in athletes. Am J Sport Med. 2011;9:7S–13S. doi: 10.1177/0363546511404144. (suppl) [DOI] [PubMed] [Google Scholar]
- 7.Nho S.J., Magennis E.M., Singh C.K., Kelly B.T. Outcomes after the arthroscopic treatment of femoroacetabular impingement in a mixed group of high-level athletes. Am J Sport Med. 2011;39:14S–19S. doi: 10.1177/0363546511401900. (suppl) [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Technique for bridging suture repair for acetabular cartilage carpet delamination. The patient is in the prone position. A right hip is shown, with the camera positioned in the anterolateral portal.