

Abstract
Tenodesis of the long head of the biceps (LHB) is a frequently performed procedure during shoulder arthroscopy for the treatment of degenerative, traumatic, or inflammatory lesions of the LHB tendon. Arthroscopic techniques for LHB tenodesis using knotless screw techniques offer the advantage of circumventing the need for arthroscopic knot tying. In 2012 Song and Williams described a novel tenodesis technique that does not require any knot-tying procedures by using a knotless anchor. However, a single-anchor configuration may not offer adequate stabilization of the LHB tendon. Therefore we propose a modified method that uses a double knotless anchor that offers advantages over the single knotless anchor, such as an increase in the contact area between the tendon and bone to facilitate tendon-to-bone healing and strengthening of the tenodesis construct.
The biceps tenodesis procedure has been shown to be an appropriate surgical treatment for various pathologies related to the long head of the biceps (LHB) tendon.1, 2, 3 In 2012 Song and Williams4 described a novel tenodesis technique that does not require any knot-tying procedures by using a knotless anchor. This technique was reported to be a safe, effective, and reliable method to treat LHB tendinopathy with respect to pain relief, strength maintenance, and avoidance of cosmetic deformity. However, a single-anchor configuration may not offer adequate stabilization of the LHB tendon. Therefore we propose a modified method that uses a double knotless anchor that offers advantages over the single knotless anchor, such as an increase in the contact area between the tendon and bone to facilitate tendon-to-bone healing and strengthening of the tenodesis construct (Table 1, Table 2, Table 3, Table 4).
Table 1.
Key Points
| Knotless anchor tenodesis that does not require any knot-tying procedures is a quicker and simpler technique; however, a single-anchor configuration may not adequately stabilize the LHB. |
| Our double–knotless anchor technique increases the contact area between the tendon and bone, which may facilitate tendon-to-bone healing and subsequent strengthening of the tenodesis construct. |
LHB, long head of biceps.
Table 2.
Summary of Double–Knotless Anchor Tenodesis
| A modified winding stitch is used to wrap circumferentially around the tendon. |
| The first anchor is placed 15 mm distal to the articular entrance of the bicipital groove. |
| The second anchor is placed at the articular entrance of the bicipital groove. |
Table 3.
Advantages and Pitfalls
| Advantages |
| The technique is relatively safe and reproducible. |
| Rotational movement of the tendon is prevented. |
| Tendon grip is improved. |
| The tenodesis construct is strengthened. |
| The technique may provide higher healing potential given the increased contact between tendon and bone. |
| Pitfalls |
| Cost is increased with the use of double anchors. |
| The technique is time-consuming because of the use of double anchors. |
| Pain in the bicipital groove may theoretically occur. |
| Supination weakness is possible. |
Table 4.
Tips
| To aid in accomplishment of the modified winding stitch, the surgeon should use a suture-passing instrument (BirdBeak Penetrator) and the suture shuttle technique. |
| To prevent sutures from becoming entangled, the anterior cannula must always be kept empty to facilitate the placement of 2 winding stitches and double anchors. |
| The distance between the 2 modified winding stitches is 10 mm, whereas the distance between the anchor placements is >10 mm; as a result, a firmer attachment of the tendon to the bicipital groove is achieved. |
Surgical Technique
In most instances the supraspinatus tendon has experienced a full-thickness tear. In the few instances without such tears, a percutaneous needle and monofilament suture (No. 1 polydioxanone [PDS]) were used to mark positions that enabled the bicipital groove to be easily located. All surgical procedures were performed with the patient in the lateral decubitus position with traction on the affected limb under general anesthesia and an adjunctive interscalene block.
An arthroscope was placed into the subacromial space through the posterolateral portal at the posterolateral edge of the acromion. Subsequently, a bursectomy was performed through the lateral portal. In cases in which the bicipital groove and transverse humeral ligament in the subacromial space were not evident, the marking suture was used. It should be noted that the tenodesis was performed in full before cutting of the intra-articular portion of the LHB tendon. The attachment of the LHB tendon makes it easier to pass a suture-passing instrument (BirdBeak Penetrator, 2.75 mm, 45° up-curved tip; Arthrex, Naples, FL) through the tendon. The first modified winding stitch commenced on the biceps tendon near the articular entrance of the bicipital groove and proceeded with passing of the tip of the BirdBeak device loaded with a No. 2 nonabsorbable braided suture (Ultrabraid; Smith & Nephew, Andover, MA) through the midportion of the LHB tendon through the anterior portal cannula (Threaded Cannula, 8.5 mm × 72 mm; Smith & Nephew) (Fig 1). A suture retriever (Arthrex) introduced through the lateral portal was used to grasp and pull 1 side of the suture limb from the tip of the BirdBeak. Then, the BirdBeak loaded with a PDS suture was placed through the anterior portal again and passed under the LHB tendon (Fig 2). A suture retriever introduced through the lateral portal was used to grasp and pull out 1 side of the PDS suture from the tip of the BirdBeak. The opposite side of the PDS suture still remaining in the anterior portal was to be used as a suture shuttle. The suture limb being held in the lateral portal was retrieved through the anterior portal by use of the suture retriever and was subsequently tied to the limb of the PDS suture outside the cannula of the anterior portal. Next, by pulling the other limb of the PDS suture, the permanent suture was pulled in a retrograde manner, passing over and then under the tendon, to wrap circumferentially around the tendon (Fig 3). Afterward, the 2 suture limbs were grasped and pulled through the anterior portal cannula. To aid in suture management, a switching stick was placed through the anterior cannula, after which the cannula was removed. Both suture limbs were then pulled out of the cannula, and a hemostat was affixed to them. The cannula was subsequently placed back over the stitching stick into the subacromial space, rendering the anterior cannula empty to facilitate the placement of the second winding stitch. After the deployment of the first modified winding stitch, the second stitch was placed at the LHB tendon 10 mm distal to the first winding stitch.
Fig 1.
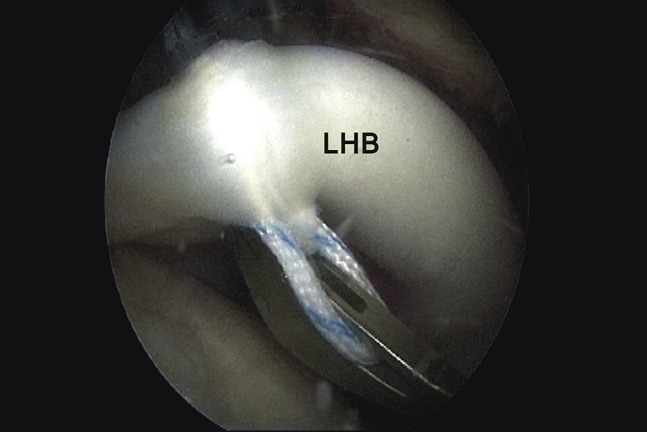
Arthroscopic image of a left shoulder in the lateral decubitus position from the posterolateral viewing portal. The biceps tendon in the subacromial space was displaced from the bicipital groove to facilitate passing of the tip of the BirdBeak loaded with a nonabsorbable suture through the midportion of the biceps tendon through the anterior portal. (LHB, long head of biceps.)
Fig 2.
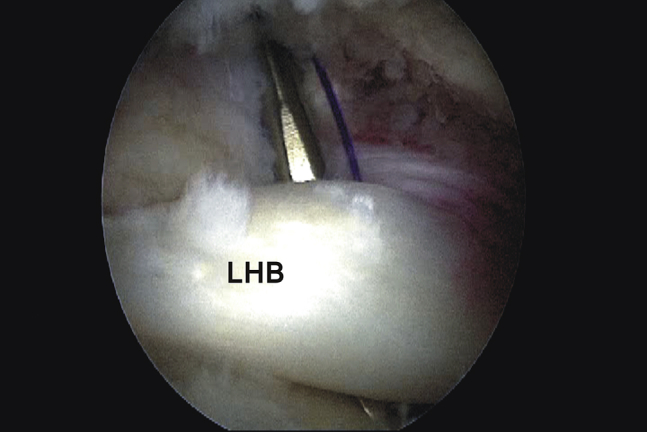
Arthroscopic image of a left shoulder from the posterolateral viewing portal showing the polydioxanone-loaded BirdBeak introduced again through the anterior portal and passed under the long head of the biceps (LHB) tendon.
Fig 3.
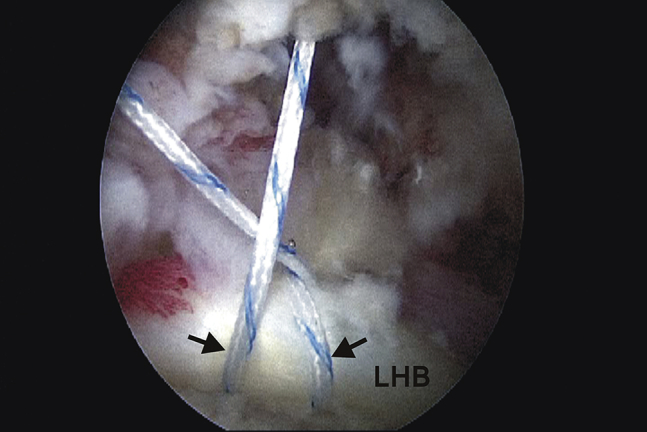
Arthroscopic image of a left shoulder from the posterolateral viewing portal showing the modified winding suture deployed by passing 1 limb of the suture over and under the tendon (arrows). (LHB, long head of biceps.)
A hole was punched 15 mm distal to the articular entrance of the bicipital groove with a 3.8-mm-diameter awl through the anterior portal for the knotless anchor screw (Footprint PK, 4.5 mm; Smith & Nephew). Then, with the assistance of the suture threading loop, the 2 ends of the suture were passed through the eyelet of the anchor, with the eyelet and tip of the loaded suture anchor subsequently placed into the prepared hole. Thereafter, the suture anchor was implanted approximately 1 mm below the bone surface using a mallet to tap the inserter handle until the laser mark was flush with the cortical bone. A slight downward pressure was maintained on the inserter handle as the sutures were manually pulled until the appropriate tension was achieved. The torque limiter knob located on the proximal end of the inserter handle was rotated in a clockwise manner to advance the inner anchor plug and lock the sutures. The sutures were checked to ensure adequate tension, after which any excess suture was cut. Then, both suture limbs of the first winding stitch located outside the anterior cannula were retrieved back into the anterior cannula. The same process was repeated for the deployment of the second anchor placed at the articular entrance of the bicipital groove (Fig 4). It is critical to place both anchors more than 10 mm apart to achieve optimal fixation. Because placement of the second winding stitch was 10 mm from the first, a firmer attachment of the LHB tendon to the bicipital groove was obtained with tensioning and locking of the suture (Fig 5).
Fig 4.
Arthroscopic image of a left shoulder from the posterolateral viewing portal showing the suture anchor loaded with 2 suture limbs and implanted into the bone hole from the anterior portal. (LHB, long head of biceps.)
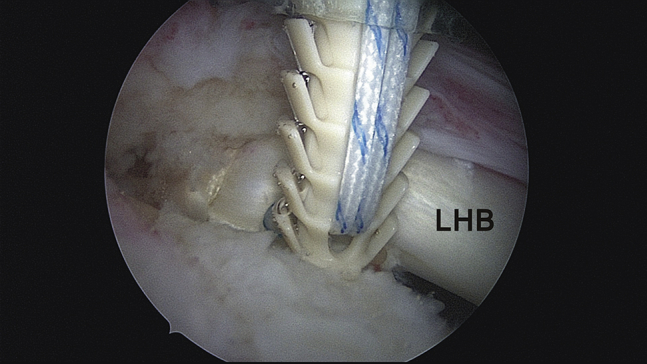
Fig 5.
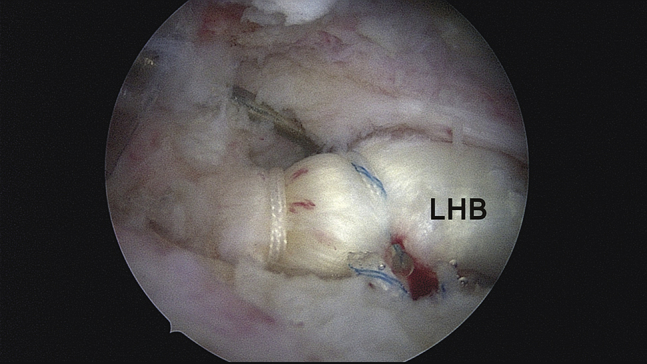
Arthroscopic image of a left shoulder from the posterolateral viewing portal showing that 2 modified winding suture stitches were placed on the biceps tendon at the bicipital groove. This technique was designed to improve biceps grip and simultaneously increase the contact area between the biceps tendon and the bone. (LHB, long head of biceps.)
After double–knotless anchor fixation of the tendon, a radiofrequency device (ArthroCare, Sunnyvale, CA) was used to sever the tendon at its attachment to the superior labrum by approaching the intra-articular space from the subacromial space through the torn site of the supraspinatus tendon. The remnant LHB tendon was pulled out of the glenohumeral joint to the subacromial space by a probe. After the radiofrequency device was used to cut the tendon at the site just proximal to the tenodesis, the grasper was introduced to grab and remove the remnant tendon (Video 1).
Postoperative rehabilitation can be adjusted according to the combined pathology. An abduction brace should be worn for 6 weeks after surgery.
Discussion
Knotless screw fixations are commonly used in shoulders for arthroscopic rotator cuff repairs, Bankart repairs, and SLAP repairs.5, 6 Thus the transition to arthroscopic biceps tenodesis seems like a logical progression, given the common practice of knotless screw fixation in the shoulder. In 2012 Song and Williams4 described an arthroscopic technique that uses a knotless screw in the fixation of the biceps tendon. In our pilot study, a single knotless screw alone provided an ultimate failure load of only 70 N and therefore could not sustain the reference ultimate failure load of 112 N, which was defined by Patzer et al.7 as the reference load that a biceps tenodesis construct should withstand to yield sufficient stability for tendon healing to the bone. Consequently, the second knotless screw was added to this technique to provide additional fixation strength.
The most attractive advantage of this technique is the use of the knotless screw. Various biceps tenodesis techniques such as the suture anchor fixation or percutaneous intra-articular transtendon technique use suture materials, where the sutures are passed through the LHB tendon and knotted over the tendon.1, 8 However, the knots tied over the tendon may cause irritation under the coracoid process and coracoacromial ligament. We believe that arthroscopic knot-tying procedures are often time-consuming and demanding; thus, easing the technically demanding portions of the procedure is highly desirable when evaluating various techniques with the same indication.
We modified the winding suture technique proposed by Song and Williams4 by using a suture shuttle approach to pass the suture over and under the tendon to ultimately wrap around the tendon, rather than the conventional under and over sequence, to prevent rotational movement of the tendon while punching in the anchor screw. Moreover, rotational motion may ultimately interfere with healing if the contact area between the tendon and bone is compromised.
One of the concerns with this technique is the requirement for the tendon to heal to the surface of the humeral cortex rather than within the intramedullary canal.9, 10 Lack of contact between the tendon and the cancellous bone may degrade the healing potential of an LHB tenodesis. However, the literature is replete with examples of suprapectoral or subpectoral biceps tenodesis procedures that have shown good to excellent results with the use of only suture anchors.11 Nevertheless, with our technique, such healing may be enhanced by the compensation that the double knotless anchor provides by increasing the tendon–bone surface contact area.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Arthroscopic biceps tenodesis with a double–knotless anchor technique in a left shoulder. The subacromial space was viewed through the posterolateral portal in the lateral decubitus position. The biceps tendon was fixed by 2 knotless anchors. One anchor was located at the entrance of the bicipital groove, and the second was placed 15 mm distal to the first after placement of 2 modified winding stitches on the tendon. This technique offers advantages over the single knotless anchor, such as increasing the contact area between the tendon and bone to facilitate tendon-to-bone healing and strengthening the tenodesis construct.
{kind=link}
References
- 1.Lee H.I., Shon M.S., Koh K.H., Lim T.K., Heo J., Yoo J.C. Clinical and radiologic results of arthroscopic biceps tenodesis with suture anchor in the setting of rotator cuff tear. J Shoulder Elbow Surg. 2014;23:e53–e60. doi: 10.1016/j.jse.2013.06.004. [DOI] [PubMed] [Google Scholar]
- 2.Su W.R., Budoff J.E., Chiang C.H., Lee C.J., Lin C.L. Biomechanical study comparing biceps wedge tenodesis with other proximal long head of the biceps tenodesis techniques. Arthroscopy. 2013;29:1498–1505. doi: 10.1016/j.arthro.2013.06.013. [DOI] [PubMed] [Google Scholar]
- 3.Wu P.T., Jou I.M., Yang C.C. The severity of the long head biceps tendinopathy in patients with chronic rotator cuff tears: Macroscopic versus microscopic results. J Shoulder Elbow Surg. 2014;23:1099–1106. doi: 10.1016/j.jse.2013.11.013. [DOI] [PubMed] [Google Scholar]
- 4.Song H.S., Williams G.R., Jr. All-arthroscopic biceps tenodesis by knotless winding suture. Arthrosc Tech. 2012;1:e43–e46. doi: 10.1016/j.eats.2012.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.El-Azab H., Buchmann S., Beitzel K., Waldt S., Imhoff A.B. Clinical and structural evaluation of arthroscopic double-row suture-bridge rotator cuff repair: Early results of a novel technique. Knee Surg Sports Traumatol Arthrosc. 2010;18:1730–1737. doi: 10.1007/s00167-010-1257-3. [DOI] [PubMed] [Google Scholar]
- 6.Ng D.Z., Kumar V.P. Arthroscopic Bankart repair using knot-tying versus knotless suture anchors: Is there a difference? Arthroscopy. 2014;30:422–427. doi: 10.1016/j.arthro.2014.01.005. [DOI] [PubMed] [Google Scholar]
- 7.Patzer T., Rundic J.M., Bobrowitsch E., Olender G.D., Hurschler C., Schofer M.D. Biomechanical comparison of arthroscopically performable techniques for suprapectoral biceps tenodesis. Arthroscopy. 2011;27:1036–1047. doi: 10.1016/j.arthro.2011.03.082. [DOI] [PubMed] [Google Scholar]
- 8.Sekiya J.K., Elkousy H.A., Rodosky M.W. Arthroscopic biceps tenodesis using the percutaneous intra-articular transtendon technique. Arthroscopy. 2003;19:1137–1141. doi: 10.1016/j.arthro.2003.10.022. [DOI] [PubMed] [Google Scholar]
- 9.Brady P.C., Narbona P., Adams C.R. Arthroscopic proximal biceps tenodesis at the articular margin: Evaluation of outcomes, complications, and revision rate. Arthroscopy. 2015;31:470–476. doi: 10.1016/j.arthro.2014.08.024. [DOI] [PubMed] [Google Scholar]
- 10.Mazzocca A.D., Cote M.P., Arciero C.L., Romeo A.A., Arciero R.A. Clinical outcomes after subpectoral biceps tenodesis with an interference screw. Am J Sports Med. 2008;36:1922–1929. doi: 10.1177/0363546508318192. [DOI] [PubMed] [Google Scholar]
- 11.Koh K.H., Ahn J.H., Kim S.M., Yoo J.C. Treatment of biceps tendon lesions in the setting of rotator cuff tears: Prospective cohort study of tenotomy versus tenodesis. Am J Sports Med. 2010;38:1584–1590. doi: 10.1177/0363546510364053. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Arthroscopic biceps tenodesis with a double–knotless anchor technique in a left shoulder. The subacromial space was viewed through the posterolateral portal in the lateral decubitus position. The biceps tendon was fixed by 2 knotless anchors. One anchor was located at the entrance of the bicipital groove, and the second was placed 15 mm distal to the first after placement of 2 modified winding stitches on the tendon. This technique offers advantages over the single knotless anchor, such as increasing the contact area between the tendon and bone to facilitate tendon-to-bone healing and strengthening the tenodesis construct.