

Abstract
Background
Duloxetine has been approved in the United States, European Union and some Asian countries for the treatment of diabetic peripheral neuropathic pain (DPNP). We assessed the efficacy and safety of duloxetine (60 mg once daily) compared with placebo in Chinese patients suffering from DPNP.
Methods
This was a phase 3, multicenter, randomised, double-blind, parallel, placebo-controlled, 12-week trial of the treatment of DPNP with duloxetine. Subjects were male and female outpatients ≥ 18 years of age with DPNP, as assessed by the Michigan Neuropathy Screening Instrument, and had a rating of ≥ 4 on the Brief Pain Inventory-Modified Short Form-Severity weekly average pain item. The primary efficacy measure was the reduction in pain severity from baseline to 12 weeks, as measured by the weekly mean of 24-h average pain ratings recorded in the patient’s diary. Mean changes from baseline in efficacy measures were analysed by a restricted maximum likelihood-based, mixed-effects model repeated measures approach and by analysis of covariance.
Results
Of the 405 patients randomised, 203 patients were assigned to duloxetine 60 mg once daily and 202 patients were assigned to placebo. Duloxetine-treated patients showed significantly greater pain relief on 24-h average pain ratings compared with placebo-treated patients each week of the 12-week study period [week 12: least squares (LS) mean change duloxetine: −2.40, placebo: −1.97; LS mean change difference (95% confidence interval) = −0.43 (−0.82, −0.04), p = 0.030]. Compared with placebo, patients treated with duloxetine experienced higher rates of nausea (p = 0.010), somnolence (p < 0.001) and asthenia (p = 0.002).
Conclusions
Duloxetine-treated patients showed significantly greater pain relief compared with placebo-treated patients over the 12-week study period. Duloxetine was shown in Chinese patients to have a safety profile similar to that found in previous duloxetine trials.
What’s known
The efficacy of duloxetine for the treatment of diabetic peripheral neuropathic pain (DPNP) is well-documented. This treatment has been approved in the United States, Europe and some Asian countries.
What’s new
The present study is the first positive registration study of the use of duloxetine in the treatment of Chinese patients with DPNP. Patients treated with duloxetine had significantly greater reduction in weekly means of 24-h average pain, 24-h worst pain and 24-h night pain relative to placebo-treated patients. A greater proportion of patients treated with duloxetine experienced 30% and 50% reductions in weekly means of 24-h average pain, compared with the placebo group. More patients treated with duloxetine (compared with placebo) reported feeling ‘much better.’ The safety profile in Chinese patients was similar to that in other duloxetine studies.
Introduction
Diabetic peripheral neuropathic pain (DPNP) is a condition resulting from nerve damage after a prolonged period of suboptimal glycemic control 1. A complication of diabetes, DPNP is associated with variable pain described as aching, tingling and burning in the feet or lower legs, and is often worse at night and therefore frequently affects sleep 2,3. A recent meta-analysis indicates that the prevalence of diabetes in China is between 4.6% and 8.0%, depending on the region, and has been sharply increasing over the last three decades 4. Up to 50% of patients with diabetes develop peripheral neuropathy 5.
The neurotransmitters serotonin and norepinephrine have been implicated in the mediation of endogenous analgesic mechanisms through the descending inhibitory pain pathways in the brain and spinal cord 6,7. Dysfunction within the endogenous pain inhibitory mechanisms may contribute to the sensitisation and hyperexcitability of pain-transmitting pathways, resulting in persistent pain 8. Duloxetine is a selective and relatively balanced reuptake inhibitor of serotonin and norepinephrine 9 and has previously been found to be effective in the management of musculoskeletal pain 10,11 and fibromyalgia 12. For the treatment of DPNP, the efficacy of duloxetine has been established in four placebo-controlled trials 13–16. Tanenberg et al. 17 showed that duloxetine was non-inferior to pregabalin for the treatment of DPNP. In addition, maintenance of effect of duloxetine in patients with DPNP has been shown in a 6-month open-label study by Skljarevski et al. 18. Two 52-week studies 19,20 also provided evidence that duloxetine was superior to routine care for the long-term management of DPNP. A third 52-week study 21 found that duloxetine was safe and well-tolerated compared with routine care.
Currently, there is no acknowledged standard of treatment in China for DPNP. However, results from recent studies of the pharmacokinetic properties of duloxetine in healthy Chinese volunteers 22,23 are consistent with those of a previous study of duloxetine comparing Japanese and Caucasian subjects 24. Therefore, it is hypothesised that duloxetine should be effective for the treatment of DPNP in Chinese patients as it is for other studied populations.
The primary objective of this study was to assess the efficacy of duloxetine at a dose of 60 mg once daily compared with placebo in Chinese patients suffering from DPNP. This objective was assessed by using the change in pain severity from baseline to 12 weeks, as measured by the weekly mean of the daily pain ratings based on an 11-point Likert scale reported by the patient. Secondary objectives included further assessments of the reduction in DPNP over the 12-week treatment period, the study of patient-reported health outcomes, and the evaluation of the safety of duloxetine 60 mg once daily.
Materials and methods
Study design
This phase 3, multicenter, randomised, double-blind, parallel, placebo-controlled trial consisted of three study periods (Figure1). In Study Period I, an assessment and screening period of up to 3-week duration, patients were evaluated for study eligibility. Patients who met entry criteria were enrolled in the treatment phase (Study Period II). Randomised (1:1) to one of two treatment groups, patients received either duloxetine 60 mg once daily or placebo once daily. Those patients randomised to duloxetine were initially treated with 30 mg once daily, then, increased to 60 mg once daily after 1 week. During this study period, patients were evaluated on efficacy and safety measures. Study Period III was a 1-week, double-blind tapering period after the 12-week treatment phase. Patients who were treated with duloxetine were given 30 mg once daily and patients treated with placebo remained on placebo for the duration of the study period.
Figure 1.
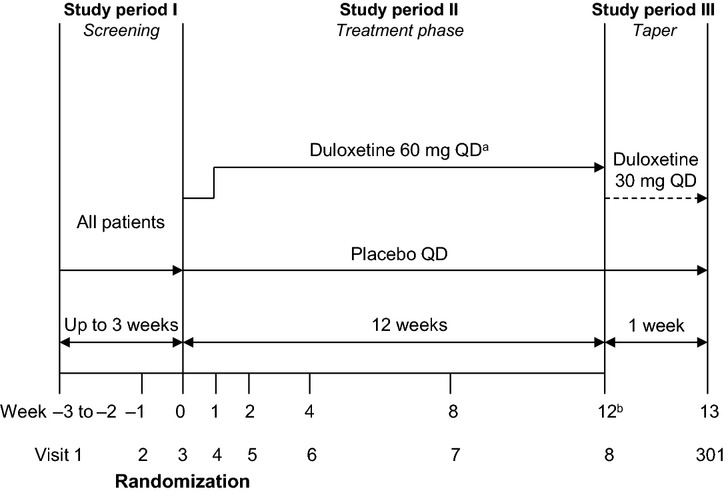
Study design. QD, once daily. aPatients randomised to duloxetine started treatment at 30 mg QD for the first week. bStudy Period III was a required taper and began either at the patient’s final visit for Study Period II (visit 8), or if a patient discontinued early after visit 4 (provided the patient was not discontinued due to suicide risk).
Patients were allowed to take up to 3 g of acetaminophen daily as rescue treatment. Other analgesic agents were not allowed during the screening period. However, after the screening period, episodic use of some analgesics was allowed for pain unrelated to diabetic neuropathy (e.g. for the treatment of injuries). ‘Episodic use’ was defined as no more than 3 consecutive days, not to exceed 14 total days during the study. Patients were not allowed to take analgesics within 3 days prior to a scheduled visit. Any patient who exceeded the allotted use of analgesics during the study would have been discontinued. Patients taking herbal remedies/medicines started taking them at least 1 month prior to the study and continued taking them throughout the study. No changes in frequency of use, changes in dose or addition of other compounds were allowed.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and its guidelines. The Ethical Review Boards at each investigative site provided written approval of the study protocol and the informed consent document. No protocol-related procedures were performed before patients signed the informed consent document.
Study population
Subjects included male and female outpatients, at least 18 years of age, who presented with bilateral DPNP that began in the feet with relatively symmetrical onset. Daily pain had to be present for at least 6 months. The diagnosis was confirmed at study entry by a score of at least three on the Michigan Neuropathy Screening Instrument. A rating of at least 4 on the Brief Pain Inventory-Modified Short Form-Severity (BPI-Severity) weekly average pain item at both screening visits was also required. Patients were excluded from the study if they had any medical or other condition that could have compromised participation in the study. These criteria included unstable glycemic control (glycosylated haemoglobin > 12%), major depressive disorder, mania, bipolar disorder, dysthymia, anxiety disorders (excluding phobias), alcohol or eating disorders, psychosis, risk for suicide, serious or unstable cardiovascular, hepatic, renal, respiratory, or haematological illness, symptomatic peripheral vascular disease, or the presence of other serious medical conditions. The first patient was enrolled in May 2011 and last patient completed the study in August 2013.
Efficacy measures
Severity of DPNP is reported here as the weekly mean of the daily pain ratings (average pain, worst pain and night pain) recorded in the patient’s diary (a self-assessment of the past 24 h, based on an 11-point Likert scale, from 0 (no pain) to 10 (worst possible pain). In addition, the BPI-Severity scale 25 was reported/collected at weekly visits. Questions assessed the severity of worst pain (previous 24 h), least pain (previous 24 h), average pain (no timeframe specified) and ‘pain right now.’ Like the patient’s pain diary, the severity ratings for the BPI-Severity scale range from 0 (no pain) to 10 (pain as bad as you can imagine). The Patient Global Impression of Improvement (PGI-Improvement) scale, a 7-point scale, was completed by the patient to measure the degree of symptom improvement at the time of assessment. A rating of 1 indicates that the patient is ‘very much improved,’ a rating of 4 indicates that the patient has experienced ‘no change,’ and a rating of 7 indicates that the patient is ‘very much worse.’
Health outcomes measures
To assess patient-reported health outcomes, this study utilised the Brief Pain Inventory-Short Form-Interference (BPI-Interference) scale and the Sheehan Disability Scale (SDS) 26. The BPI-Interference was completed by patients to measure the degree to which DPNP interfered with several activities of their daily living. Seven questions assessing the interference of pain for general activity, mood, walking ability, normal work, relations with other people, sleep, and enjoyment of life were scored, ranging from 0 (does not interfere) to 10 (completely interferes). The SDS, a patient-rated instrument used to assess the functional impact of symptoms on several inter-related domains, asked patients to rate the extent to which work or school, social life and home life or family responsibilities are impaired by their symptoms. Ranging from 0 (not at all) to 10 (extremely), scores of 5 and above are associated with significant functional impairment. Patients were also asked to provide their impression of how many days were lost or rendered unproductive during the past week because of their symptoms.
Safety measures
The following safety parameters were evaluated during the study: discontinuations because of adverse events, adverse events (regardless of whether they were perceived to be related to the study drug), serious adverse events, treatment-emergent adverse events, vital signs (sitting blood pressure and pulse rate), weight, laboratory analyses, suicide-related events (behaviour and/or ideations) and the Quick Inventory of Depressive Symptomatology-Self-Rated (QIDS-SR) total scores 27.
Statistical analysis
Sample size was based on the primary objective to assess the efficacy of duloxetine compared with placebo, measured by the 12-week change on the weekly mean of the daily average pain. With a clinical difference of 0.6 and a likely standard deviation of 2.01, a total sample size of 400 patients (200 patients per group) was planned for 5% two-sided alpha and 90% power. An intent-to-treat principle was used in the analyses of all efficacy variables, i.e. patients were analysed based on their randomised treatment assignment, even if the patient did not take the assigned treatment, did not receive the correct treatment, or did not follow or complete the protocol. For each efficacy variable, the analysis included all randomised patients with a baseline and at least one postbaseline observation. All randomised patients who received at least one dose of a trial treatment were included in the safety analyses (Safety Set). Investigative sites with fewer than four patients with postbaseline data were pooled for statistical analysis purposes.
Mean changes from baseline in efficacy measures, including health outcomes measures, were analysed by a restricted maximum likelihood (REML)-based, mixed-effects model repeated measures approach (MMRM) with the terms of treatment, investigative site, visit, treatment-by-visit interaction, baseline pain severity rating and baseline rating-by-visit interaction included into the model, and by analysis of covariance with the terms of treatment, investigative site, treatment-by-investigative site interaction and baseline pain severity ratings included. Mean changes from baseline to 12 weeks in health outcomes measures were analysed by analysis of covariance. Also, Fisher’s exact test was used to compare the incidence rates of serious adverse events, reasons for discontinuation and treatment-emergent adverse events of duloxetine and placebo. A treatment-emergent adverse event was defined as an adverse event that first occurred or worsened during the acute treatment phase after baseline. Fisher’s exact test was also used to compare frequency of usage of concomitant medications and treatment compliance.
Analysis of proportions of patients experiencing ≥ 30% and ≥ 50% reductions 28,29 at end-point (last observation carried forward) were carried out on the BPI-Severity of average pain and weekly means of 24-h average pain from patient diaries. Cochran Mantel Haenszel tests stratified by investigative site were performed. Finally, the number needed to treat (NNT) and the number needed to harm (NNH) were calculated.
All tests of treatment effects were conducted at a two-sided alpha level of 0.05. Analyses were conducted with sas® Version 9.2 (The SAS Institute, Inc., Cary, NC) and run in the PC environment.
Results
Patient disposition
Figure2 summarises patient disposition during the screening and the 12-week treatment phase. Of the 405 patients randomised, 203 patients were assigned to duloxetine 60 mg qd and 202 patients were assigned to placebo. A total of 349 (86.2%) patients completed the 12-week treatment phase of this study, including 173 (85.2%) patients treated with once daily 60-mg duloxetine and 176 (87.1%) patients assigned placebo. At baseline, there were no statistically significant imbalances in demographics or disease characteristics between the two treatment groups (Table1).
Figure 2.
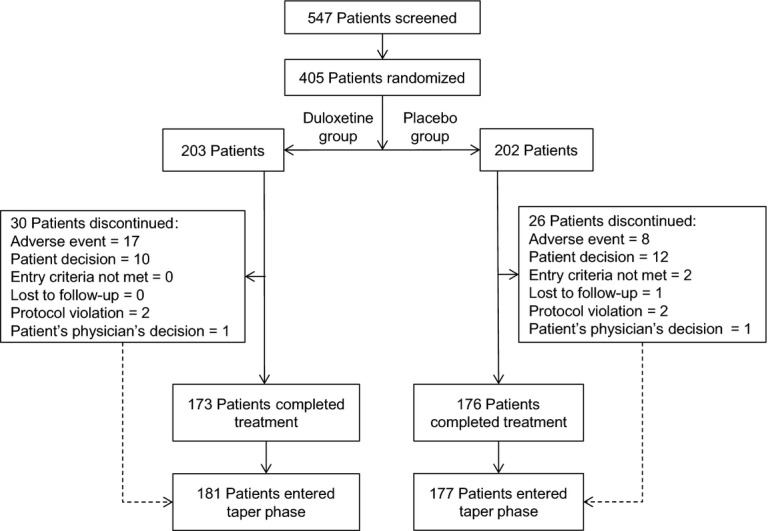
Subject disposition
Table 1.
Demographics and baseline assessments
| Duloxetine (N = 203) | Placebo (N = 202) | Total (N = 405) | p-Value | |
|---|---|---|---|---|
| Age, years, mean (SD) | 61.6 (9.7) | 61.2 (9.4) | 61.4 (9.5) | 0.431 |
| Gender,n (%) | 1.000 | |||
| Female | 112 (55.2) | 111 (55.0) | 223 (55.1) | |
| Male | 91 (44.8) | 91 (45.0) | 182 (44.9) | |
| BMI, kg/m2, mean (SD) | 24.6 (3.6) | 24.5 (3.2) | 24.6 (3.4) | 0.746 |
| Type of diabetes mellitus,n (%) | 1.000 | |||
| Type I | 3 (1.5) | 3 (1.5) | 6 (1.5) | |
| Type II | 200 (98.5) | 199 (98.5) | 399 (98.5) | |
| Duration of diabetes, years, mean (SD) | 11.5 (6.8) | 11.4 (7.5) | 11.5 (7.1) | 0.943 |
| Duration of diabetic neuropathy, years, mean (SD) | 3.5 (3.9) | 3.1 (3.1) | 3.3 (3.6) | 0.345 |
| Weekly mean of 24-h average pain severity, mean (SD) | 5.7 (1.7) | 5.6 (1.7) | 5.7 (1.7) | 0.328 |
| BPI-Severity average pain in the last week, mean (SD) | 6.0 (1.7) | 5.9 (1.6) | 5.9 (1.7) | 0.296 |
| BPI-Interference average score, mean (SD) | 4.4 (2.3) | 4.1 (2.3) | 4.2 (2.3) | 0.129 |
| SDS total score, mean (SD) | 11.2 (7.6) | 10.5 (7.3) | 10.9 (7.5) | 0.441 |
| QIDS-SR16 total score, mean (SD) | 5.6 (4.3) | 4.7 (3.9) | 5.2 (4.1) | 0.122 |
Frequencies were analysed using Fisher’s exact test; means were analysed using a type III sum of squares analysis of variance (investigator and treatment). BMI, body mass index; BPI-Interference, Brief Pain Inventory-Modified Short Form-Interference; BPI-Severity, Brief Pain Inventory-Modified Short Form-Severity; N, number of patients in group; n, number of affected patients; QIDS-SR16, 16-item Quick Inventory of Depressive Symptomatology-Self-Rated; SD, standard deviation; SDS, Sheehan Disability Scale.
Efficacy
Figure3 displays the change from baseline in weekly mean of 24-h average pain severity (from patient diaries) for both treatment groups after 12 weeks of therapy. Duloxetine-treated patients showed significantly greater pain relief (as measured by the weekly mean of the daily pain ratings recorded in patients’ diaries) compared with placebo-treated patients beginning 1 week after randomisation and continuing through the 12-week treatment phase [week 12: LS mean change (SE) duloxetine: −2.40 (0.14), placebo: −1.97 (0.14); LS mean change difference (95% confidence interval) = −0.43 (−0.82, −0.04), p = 0.030] (Table2). In addition, a greater proportion of patients treated with duloxetine experienced a reduction in the weekly mean of their 24-h average pain at end-point compared with patients treated with placebo (≥ 30% reduction: 61.5% vs. 49.0%, p = 0.014, NNT=8.0; ≥ 50% reduction: 42.0% vs. 28.8%, p = 0.006, NNT=7.6). The other weekly mean ratings of 24-h pain [‘worst pain’ (p = 0.017) and ‘night pain’ (p = 0.008)] were significantly more improved (decreased) during the 12-week treatment with duloxetine compared with placebo-treated patients (Table2) as well.
Figure 3.
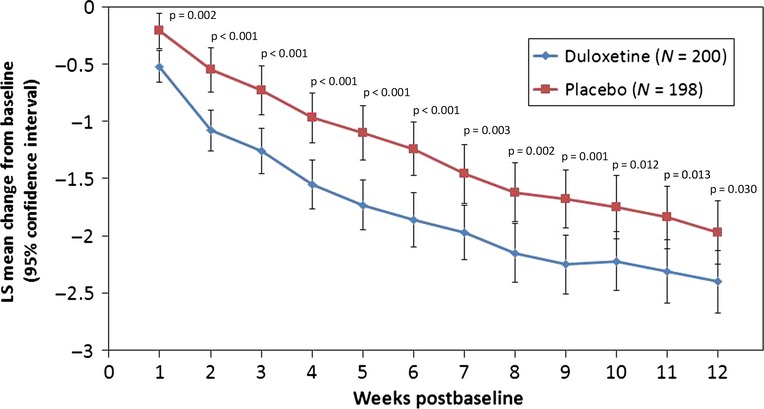
Change from baseline in weekly mean of 24-h average pain severity for all randomised patients over 12 weeks of double-blind therapy. LS, least squares; N, number of patients in group. Repeated measures analysis model: Variable = Treatment + Investigator + Week + Baseline + Treatment × Week + Baseline × Week
Table 2.
Least squares mean or mean change (week 12) in efficacy and health outcome measures
| Duloxetine | Placebo | LS mean difference (95% CI) | Between-groups p-value | |||
|---|---|---|---|---|---|---|
| N | LS mean or change (SE) | N | LS mean or change (SE) | |||
| Weekly mean score from patient’s diary | ||||||
| 24-h average pain* | 172 | −2.40 (0.14) | 173 | −1.97 (0.14) | −0.43 (−0.82, −0.04) | 0.030 |
| 24-h worst pain | 172 | −2.80 (0.16) | 173 | −2.25 (0.17) | −0.55 (−1.00, −0.10) | 0.017 |
| 24-h night pain | 172 | −2.65 (0.15) | 173 | −2.11 (0.15) | −0.54 (−0.95, −0.14) | 0.008 |
| BPI-Severity | ||||||
| Average pain | 173 | −2.50 (0.15) | 175 | −2.00 (0.15) | −0.50 (−0.90, −0.09) | 0.016 |
| Worst pain | 173 | −2.86 (0.17) | 175 | −2.36 (0.17) | −0.51 (−0.97, −0.04) | 0.032 |
| Least pain | 173 | −1.97 (0.14) | 175 | −1.41 (0.14) | −0.55 (−0.94, −0.17) | 0.004 |
| Pain right now | 173 | −2.76 (0.16) | 175 | −2.35 (0.16) | −0.41 (−0.84, 0.02) | 0.061 |
| BPI-Interference | ||||||
| Average score | 173 | −2.42 (0.13) | 176 | −1.82 (0.14) | −0.60 (−0.96, −0.24) | 0.001 |
| General activity | 173 | −2.80 (0.17) | 176 | −2.35 (0.18) | −0.45 (−0.91, 0.01) | 0.054 |
| Mood | 173 | −2.32 (0.15) | 176 | −1.77 (0.16) | −0.55 (−0.96, −0.13) | 0.010 |
| Walking ability | 173 | −2.76 (0.17) | 176 | −1.94 (0.17) | −0.82 (−1.26, −0.37) | <0.001 |
| Normal work | 173 | −2.50 (0.16) | 176 | −1.97 (0.17) | −0.53 (−0.97, −0.10) | 0.016 |
| Relations with people | 173 | −1.63 (0.14) | 176 | −1.24 (0.14) | −0.39 (−0.76, −0.02) | 0.037 |
| Sleep | 173 | −2.63 (0.17) | 176 | −2.04 (0.17) | −0.59 (−1.04, −0.14) | 0.011 |
| Enjoyment of life | 173 | −2.20 (0.15) | 176 | −1.69 (0.16) | −0.50 (−0.91, −0.10) | 0.016 |
| PGI-Improvement | 173 | 2.44 (0.07) | 176 | 2.65 (0.07) | −0.21 (−0.40, −0.02) | 0.034 |
| SDS total score | 172 | −6.36 (0.40) | 175 | −5.09 (0.42) | −1.26 (−2.33, −0.20) | 0.020 |
Repeated measures analysis model: Variable = Treatment + Investigator + Week (or Visit) + Baseline + Treatment × Week (or Visit) + Baseline × Week (or Visit). BPI-Interference, Brief Pain Inventory-Modified Short Form-Interference; BPI-Severity, Brief Pain Inventory-Modified Short Form-Severity; LS, least squares; N, number of patients in group; PGI-Improvement, Patient’s Global Impression of Improvement; SDS, Sheehan Disability Scale; SE, Standard Error.
See also Figure3, Week 12.
The BPI-Severity measures of ‘average pain’ [LS mean change (SE) for duloxetine: −2.50 (0.15); placebo: −2.00 (0.15) p = 0.016], ‘worst pain’ (p = 0.032), and ‘least pain’ (p = 0.004) were also significantly more improved (decreased) compared with placebo, while improvement in ‘pain right now’ was not statistically different between the two groups (Table2). A greater proportion of patients treated with duloxetine (compared with patients treated with placebo) experienced a reduction in pain as measured on the BPI-Severity average pain at end-point (≥ 30% reduction: 63.0% vs. 46.7%, p = 0.003, NNT=6.1; ≥ 50% reduction: 46.0% vs. 29.4%, p = 0.001, NNT = 6.0).
Significant improvements for patients treated with duloxetine (compared with placebo) were also shown in PGI-Improvement (p = 0.034). Categorical analysis of patient responses on the PGI-Improvement scale indicated an overall statistically significant difference between treatment groups (p = 0.0084; Figure4). More duloxetine-treated patients (47.2%) responded with ‘much better’ than placebo-treated patients (33.9%), while more placebo-treated patients (18.2%) responded with ‘the same’ than duloxetine-treated patients (7.1%). Patients in both treatment groups had similar proportionate responses for ‘very much better,’ ‘a little better,’ ‘a little worse’ and ‘much worse.’
Figure 4.
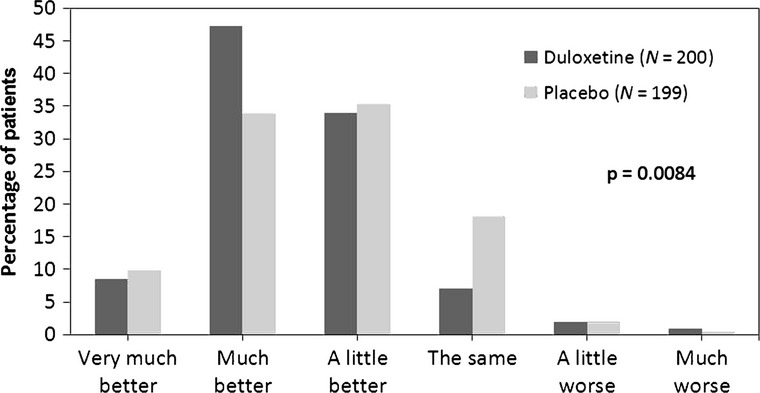
Categorical analysis of patient responses on the Patient Global Impression of Improvement scale (duloxetine vs. placebo). N, number of patients in group. Frequencies were analysed using Fisher’s exact test
Health outcomes
Health outcomes results are shown in Table2. The improvement in the BPI-Interference average score was significantly greater in the duloxetine-treated vs. the placebo-treated group (p = 0.001). All of the BPI-Interference individual items showed a statistically significantly decrease with duloxetine patients (compared with placebo) except for ‘general activity.’ Significant improvements for patients treated with duloxetine (compared with placebo) were also shown in the SDS total score (p = 0.020).
Safety and tolerability
Overall, there were few significantly different rates of serious adverse events between the two treatment groups. No deaths occurred during the study. A total of five (1.2%) patients experienced five serious adverse events during treatment phase, which included three (1.5%) duloxetine-treated patients (one asthenia, one diabetes mellitus, one nodal arrhythmia), and two (1.0%) placebo-treated patients (one cholecystitis chronic, one non-Hodgkin’s lymphoma). Asthenia was possibly related to blinded study drug, but not related to protocol procedures; others were not related to the blinded study drug or protocol procedures at the investigators’ discretion. Of 202 patients treated with duloxetine, 17 (8.4%) discontinued because of adverse events and of 202 patients treated by placebo, 8 (4.0%) discontinued because of adverse events (p = 0.097).
In addition, there were no suicide-related events (behaviour or ideation) reported. Compared with placebo, patients treated with duloxetine experienced statistically significantly higher rates of the following treatment-emergent adverse events: nausea (p = 0.010, NNH = 14.5), somnolence (p < 0.001, NNH = 12.7) and asthenia (p = 0.002, NNH=20.0) (Table3). Nausea associated with duloxetine was most often characterised as ‘mild’ [n = 19 (two patients experienced nausea twice)], but there were also cases of ‘moderate nausea’ (n = 4). All of the instances of nausea associated with placebo were characterised as ‘mild’ (n = 7). For the duloxetine group, two patients (1.0%) discontinued because of nausea, zero patients discontinued because of somnolence, and two patients (1.0%) discontinued because of asthenia. No placebo-treated patients discontinued because of these adverse events. Although not statistically significant, more duloxetine-treated patients (8.4%) discontinued the study because of any adverse event compared with placebo-treated patients (4.0%) in this study.
Table 3.
Adverse events (treatment phase) in ≥ 5% of duloxetine-treated patients or that were statistically different between duloxetine and placebo
| Duloxetine (N = 202), n (%) | Placebo (N = 202), n (%) | p-Value | |
|---|---|---|---|
| Patients with ≥ 1 TEAE | 94 (46.5) | 72 (35.6) | 0.034 |
| Nausea | 21 (10.4) | 7 (3.5) | 0.010 |
| Dizziness | 17 (8.4) | 9 (4.5) | 0.155 |
| Decreased appetite | 11 (5.4) | 8 (4.0) | 0.639 |
| Somnolence | 17 (8.4) | 1 (0.5) | < 0.001 |
| Constipation | 10 (5.0) | 4 (2.0) | 0.172 |
| Fatigue | 10 (5.0) | 4 (2.0) | 0.172 |
| Asthenia | 10 (5.0) | 0 | 0.002 |
Frequencies were analysed by Fisher’s exact test. N, number of patients in group; n, number of affected patients; TEAE, treatment-emergent adverse event.
There were no significant LS mean changes from baseline for duloxetine for blood pressure, heart rate or weight. Also, QIDS-SR16 total scores (LS mean change, week 12) were not significantly different between treatment groups.
Concomitant medications
Almost all of the patients in this study (97.3%) were taking concomitant medications. The most commonly used drugs (≥ 10% of patients) were metformin (37.8%), acarbose (31.9%), mecobalamin (17.5%), Chinese medicine (16.5%), human mixtard (15.6%), insulin glargine (14.6%), acetylsalicylic acid (13.6) and repaglinide (10.6%). The only drug used by at least 5% of patients and whose rate of use was different between treatment groups was glimepiride (duloxetine: 11.3%; placebo: 5.4%; p = 0.047). No more than 2.7% of patients had taken paracetamol on any visit (duloxetine group, no more than 3.5%; placebo group, no more than 2.8%), and no statistically significant differences between treatment groups in use of paracetamol were observed on any visit (Table4).
Table 4.
Percentage use of concomitant paracetamol, by visit
| Duloxetine | Placebo | Total | p-Value | |
|---|---|---|---|---|
| Paracetamol (visit 3 – baseline) | ||||
| N | 202 | 202 | 404 | 0.543 |
| Yes, n (%) | 7 (3.5) | 4 (2.0) | 11 (2.7) | |
| No, n (%) | 195 (96.5) | 198 (98.0) | 393 (97.3) | |
| Paracetamol (visit 4) | ||||
| N | 200 | 198 | 398 | 0.371 |
| Yes, n (%) | 1 (0.5) | 3 (1.5) | 4 (1.0) | |
| No, n (%) | 199 (99.5) | 195 (98.5) | 394 (99.0) | |
| Paracetamol (visit 5) | ||||
| N | 191 | 191 | 382 | 1.000 |
| Yes, n (%) | 2 (1.0) | 3 (1.6) | 5 (1.3) | |
| No, n (%) | 189 (99.0) | 188 (98.4) | 377 (98.7) | |
| Paracetamol (visit 6) | ||||
| N | 184 | 187 | 371 | 0.724 |
| Yes, n (%) | 3 (1.6) | 5 (2.7) | 8 (2.2) | |
| No, n (%) | 181 (98.4) | 182 (97.3) | 363 (97.8) | |
| Paracetamol (visit 7) | ||||
| N | 178 | 181 | 359 | 0.215 |
| Yes, n (%) | 1 (0.6) | 5 (2.8) | 6 (1.7) | |
| No, n (%) | 177 (99.4) | 176 (97.2) | 353 (98.3) | |
| Paracetamol (visit 8) | ||||
| N | 174 | 176 | 350 | 1.000 |
| Yes, n (%) | 2 (1.1) | 3 (1.7) | 5 (1.4) | |
| No, n (%) | 172 (98.9) | 173 (98.3) | 345 (98.6) | |
Frequencies were analysed by Fisher’s exact test. N, number of patients in group; n, number of affected patients.
Discussion
Assessing the efficacy of duloxetine in Chinese patients with DPNP, the results of this double-blind, placebo-controlled trial show that duloxetine-treated patients reported significantly greater pain relief compared with placebo-treated patients over the 12-week study period. In support of this conclusion, a greater proportion of patients treated with duloxetine (compared with patients treated with placebo) experienced ≥ 30% and ≥ 50% reductions in weekly mean of 24-h average pain and BPI-Severity (average pain) at end-point. In addition, more duloxetine-treated patients indicated they were ‘much better’ on the PGI-Improvement scale, compared with placebo.
For response rates, as mentioned above, compared with placebo, a greater proportion of patients treated with duloxetine experienced ≥ 30% and ≥ 50% pain reductions. Improvements of ≥ 30% corresponded to patients feeling ‘a little better’ and improvements of ≥ 50% corresponded to patients feeling ‘a lot better’ 30 in previous duloxetine DPNP studies. These cut-offs are also consistent with the recommendation from IMMPACT (the Initiative on Methods, Measurement and Pain Assessment in Clinical Trials) 28. That is, ≥ 30% pain decrease indicates moderately important improvement, while ≥ 50% pain decrease indicates substantial improvement. NNT is a straightforward way to help physicians understand the likelihood that a patient will be helped by a medication. Smaller NNTs indicate greater efficacy. The NNTs for ≥ 30% and ≥ 50% pain reductions (range: 6–8) were similar. Thus, compared with a control group, for every 6–8 patients treated, one patient will achieve a ≥ 30% or ≥ 50% reduction in pain, which is clinically meaningful.
It is worth noting that pain relief occurs and is appreciated by individuals differently. Therefore, the magnitude of a statistically significant group mean change may bear little relation to an important improvement for the person with pain 28. In clinical practice, individual level assessment is very important to determine and adapt the individual treatment strategy. It is for these reasons that we included response rates as a secondary objective in this study.
For BPI-Severity average pain, the reduction in pain with duloxetine treatment was similar to other studies on DPNP with duloxetine treatment 13–16. Although this 12-week trial does not allow for assessment of long-term use of duloxetine for DPNP patients, one 6-month and three 52-week studies assessing the long-term management of DPNP and safety of duloxetine provide support for the use of duloxetine in the long-term management of DPNP 18–21.
A recent clinical trial of duloxetine for the treatment of DPNP in Chinese patients studied the efficacy of duloxetine for the management of DPNP in this population 31. Although the difference between treatment groups on the primary outcome measure of that study (mean change in BPI-Severity average pain) was not statistically significant, secondary results supported the efficacy of duloxetine in this patient population. The authors attributed the negative result possibly to a generally higher placebo response rate in Asian, compared with Western, studies using subjective outcome measures. They also cited the inclusion of patients with major depressive disorder in the study population as problematic, as 50% of antidepressant trials fail to demonstrate a difference between study drug and placebo 32. They also cited factors relating to subjective outcomes measures and pain fluctuation associated with DPNP. In the current study, measures were taken to address factors that may have influenced outcomes in previous studies. For example, the primary outcome measure of the present study was not used as an inclusion criterion. Instead, the BPI-Severity was used to screen patients for severity of DPNP. In addition, we excluded from the present study those patients with major depressive disorder.
The overall safety profile found in this study was similar to previous studies of duloxetine. Reasons for discontinuation were not significantly different between treatment groups. Adverse event was the most cited reason for discontinuation, but still accounted for only 8.4% of duloxetine-treated patients.
Conclusion
In this study conducted in China, duloxetine-treated patients showed significantly greater pain relief compared with placebo-treated patients over the 12-week study period. Duloxetine 60 mg once daily was shown to have a similar safety profile presented in other duloxetine trials. Results from this study showed Chinese patients have similar levels of pain reduction with duloxetine treatment for the management of DPNP to that observed in other countries.
Funding and acknowledgements
This research was funded by Eli Lilly and Company. The authors thank Dr. Tianhong Luo and Dr. Haibo Xue for their contributions to this project. The authors also thank the principal investigators who took part in this research: Dr. Zhangrong Xu (The 306th Hospital of PLA), Dr. Weigang Zhao (Peking Union Medical College Hospital), Dr. Zhimin Liu (Shanghai Changzheng Hospital), Dr. Yan Li (China Sun Yat-sen Memorial Hospital of Sun Yat-sen University), Dr. Yaoming Xue (Nanfang Hospital), Dr. Shaoxiong Zheng (The Second Hospital of Tianjin Medical University), Dr. Bingyin Shi (The First Affiliated Hospital of Xi’An Jiaotong University), Dr. Lixin Shi (The Affiliated Hospital of Guiyang Medical College), Dr. Jiajun Zhao (Shandong Provincial Hospital), Dr. Jing Yang (The First Affiliated Hospital of Shanxi Medical University) and Dr. Haipeng Xiao (The First Affiliated Hospital of Sun Yat-sen University). Assistance with manuscript development and editing was provided by inVentiv Health Clinical, LLC.
Author contributions
Authors VS and JR were critical in the design of the study. Authors YG, XHG, PH, QML, GYY and SQ were involved in data acquisition. C-NW performed the statistical analysis. All authors participated in analysis and interpretation of the data and drafting and/or critical revision of the manuscript. All authors approved the final version of the manuscript.
References
- Dworkin RH. An overview of neuropathic pain: syndromes, symptoms, signs, and several mechanisms. Clin J Pain. 2002;18:343–9. doi: 10.1097/00002508-200211000-00001. [DOI] [PubMed] [Google Scholar]
- Krause SJ, Backonja MM. Development of a neuropathic pain questionnaire. Clin J Pain. 2003;19:306–14. doi: 10.1097/00002508-200309000-00004. [DOI] [PubMed] [Google Scholar]
- Galer BS, Gianas A, Jensen MP. Painful diabetic polyneuropathy: epidemiology, pain description, and quality of life. Diabetes Res Clin Pract. 2000;47:123–8. doi: 10.1016/s0168-8227(99)00112-6. [DOI] [PubMed] [Google Scholar]
- Zuo H, Shi Z, Hussain A. Prevalence, trends and risk factors for the diabetes epidemic in China: a systematic review and meta-analysis. Diabetes Res Clin Pract. 2014;104:63–72. doi: 10.1016/j.diabres.2014.01.002. [DOI] [PubMed] [Google Scholar]
- Boulton AJ, Malik RA, Arezzo JC, Sosenko JM. Diabetic somatic neuropathies. Diabetes Care. 2004;27:1458–86. doi: 10.2337/diacare.27.6.1458. [DOI] [PubMed] [Google Scholar]
- Basbaum AI, Fields HL. Endogenous pain control systems: brainstem spinal pathways and endorphin circuitry. Annu Rev Neurosci. 1984;7:309–38. doi: 10.1146/annurev.ne.07.030184.001521. [DOI] [PubMed] [Google Scholar]
- Clark FM, Proudfit HK. The projections of noradrenergic neurons in the A5 catecholamine cell group to the spinal cord in the rat: anatomical evidence that A5 neurons modulate nociception. Brain Res. 1993;616:200–10. doi: 10.1016/0006-8993(93)90210-e. [DOI] [PubMed] [Google Scholar]
- Coderre TJ, Katz J. Peripheral and central hyperexcitability: differential signs and symptoms in persistent pain. Behav Brain Sci. 1997;20:404–19. doi: 10.1017/s0140525x97251484. [DOI] [PubMed] [Google Scholar]
- Bymaster FP, Dreshfield-Ahmad LJ, et al. Comparative affinity of duloxetine and venlafaxine for serotonin and norepinephrine transporters in vitro and in vivo, human serotonin receptor subtypes, and other neuronal receptors. Neuropsychopharmacology. 2001;25:871–80. doi: 10.1016/S0893-133X(01)00298-6. [DOI] [PubMed] [Google Scholar]
- Chappell AS, Desaiah D, Liu-Seifert H, et al. A double-blind, randomized, placebo-controlled study of the efficacy and safety of duloxetine for the treatment of chronic pain due to osteoarthritis of the knee. Pain Pract. 2011;11:33–41. doi: 10.1111/j.1533-2500.2010.00401.x. [DOI] [PubMed] [Google Scholar]
- Skljarevski V, Zhang S, Desaiah D, et al. Duloxetine versus placebo in patients with chronic low back pain: a 12-week, fixed-dose, randomized, double-blind trial. J Pain. 2010;11:1282–90. doi: 10.1016/j.jpain.2010.03.002. [DOI] [PubMed] [Google Scholar]
- Chappell AS, Bradley LA, Wiltse C, et al. A six-month double-blind, placebo-controlled, randomized clinical trial of duloxetine for the treatment of fibromyalgia. Int J Gen Med. 2008;1:91–102. doi: 10.2147/ijgm.s3979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldstein DJ, Lu Y, Detke MJ, Lee TC, Iyengar S. Duloxetine vs. placebo in patients with painful diabetic neuropathy. Pain. 2005;116:109–18. doi: 10.1016/j.pain.2005.03.029. [DOI] [PubMed] [Google Scholar]
- Raskin J, Pritchett YL, Wang F, et al. A double-blind, randomized multicenter trial comparing duloxetine with placebo in the management of diabetic peripheral neuropathic pain. Pain Med. 2005;6:346–56. doi: 10.1111/j.1526-4637.2005.00061.x. [DOI] [PubMed] [Google Scholar]
- Wernicke JF, Pritchett YL, D’Souza DN, et al. A randomized controlled trial of duloxetine in diabetic peripheral neuropathic pain. Neurology. 2006;67:1411–20. doi: 10.1212/01.wnl.0000240225.04000.1a. [DOI] [PubMed] [Google Scholar]
- Yasuda H, Hotta N, Nakao K, et al. Superiority of duloxetine to placebo in improving diabetic neuropathic pain: results of a randomized controlled trial in Japan. J Diabetes Investig. 2011;2:132–9. doi: 10.1111/j.2040-1124.2010.00073.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanenberg RJ, Irving GA, Risser RC, et al. Duloxetine, pregabalin, and duloxetine plus gabapentin for diabetic peripheral neuropathic pain management in patients with inadequate pain response to gabapentin: an open-label, randomized, noninferiority comparison. Mayo Clin Proc. 2011;86:615–26. doi: 10.4065/mcp.2010.0681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skljarevski V, Desaiah D, Zhang Q, et al. Evaluating the maintenance of effect of duloxetine in patients with diabetic peripheral neuropathic pain. Diabetes Metab Res Rev. 2009;25:623–31. doi: 10.1002/dmrr.1000. [DOI] [PubMed] [Google Scholar]
- Wernicke JF, Raskin J, Rosen A, et al. Duloxetine in the long-term management of diabetic peripheral neuropathic pain: an open-label, 52-week extension of a randomized controlled clinical trial. Curr Ther Res Clin Exp. 2006;67:283–304. doi: 10.1016/j.curtheres.2006.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wernicke JF, Wang F, Pritchett YL, et al. An open-label 52-week clinical extension comparing duloxetine with routine care in patients with diabetic peripheral neuropathic pain. Pain Med. 2007;8:503–13. doi: 10.1111/j.1526-4637.2006.00258.x. [DOI] [PubMed] [Google Scholar]
- Raskin J, Smith TR, Wong K, et al. Duloxetine versus routine care in the long-term management of diabetic peripheral neuropathic pain. J Palliat Med. 2006;9:29–40. doi: 10.1089/jpm.2006.9.29. [DOI] [PubMed] [Google Scholar]
- Li H, Li T, Li Y, Shen Y. Pharmacokinetics and safety of duloxetine enteric-coated tablets in chinese healthy volunteers: a randomized, open-label, single- and multiple-dose study. Clin Psychopharmacol Neurosci. 2013;11:28–33. doi: 10.9758/cpn.2013.11.1.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao RK, Cheng G, Tang J, Song J, Peng WX. Pharmacokinetics of duloxetine hydrochloride enteric-coated tablets in healthy Chinese volunteers: a randomized, open-label, single- and multiple-dose study. Clin Ther. 2009;31:1022–36. doi: 10.1016/j.clinthera.2009.05.005. [DOI] [PubMed] [Google Scholar]
- Chan C, Yeo KP, Pan AX, et al. Duloxetine pharmacokinetics are similar in Japanese and Caucasian subjects. Br J Clin Pharmacol. 2007;63:310–4. doi: 10.1111/j.1365-2125.2006.02770.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994;23:129–38. [PubMed] [Google Scholar]
- Sheehan DV, Harnett-Sheehan K, Raj BA. The measurement of disability. Int Clin Psychopharmacol. 1996;11(Suppl. 3):89–95. doi: 10.1097/00004850-199606003-00015. [DOI] [PubMed] [Google Scholar]
- Rush AJ, Trivedi MH, Ibrahim HM, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry. 2003;54:573–83. doi: 10.1016/s0006-3223(02)01866-8. [DOI] [PubMed] [Google Scholar]
- Dworkin RH, Turk DC, Wyrwich KW, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. 2008;9:105–21. doi: 10.1016/j.jpain.2007.09.005. [DOI] [PubMed] [Google Scholar]
- Farrar JT, Young JP, Jr, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94:149–58. doi: 10.1016/S0304-3959(01)00349-9. [DOI] [PubMed] [Google Scholar]
- Farrar JT, Pritchett YL, Robinson M, Prakash A, Chappell A. The clinical importance of changes in the 0 to 10 numeric rating scale for worst, least, and average pain intensity: analyses of data from clinical trials of duloxetine in pain disorders. J Pain. 2010;11:109–18. doi: 10.1016/j.jpain.2009.06.007. [DOI] [PubMed] [Google Scholar]
- Gao Y, Ning G, Jia WP, et al. Duloxetine versus placebo in the treatment of patients with diabetic neuropathic pain in China. Chin Med J (Engl) 2010;123:3184–92. [PubMed] [Google Scholar]
- Khan A, Khan SR, Walens G, Kolts R, Giller EL. Frequency of positive studies among fixed and flexible dose antidepressant clinical trials: an analysis of the food and drug administration summary basis of approval reports. Neuropsychopharmacology. 2003;28:552–7. doi: 10.1038/sj.npp.1300059. [DOI] [PubMed] [Google Scholar]