

Abstract
Background:
Carotid intima-media thickness (IMT) is increasingly identified as a marker of atherosclerosis and increased risk of cerebrovascular disease.
Aim:
We aimed to investigate the prevalence of carotid IMT in asymptomatic Indian individuals, more than 40 years of age, and correlate it with other risk factors for cerebrovascular ischemia.
Materials and Methods:
Individuals attending outpatient services of Nizam's Institute of Medical Sciences, who were asymptomatic for cerebrovascular ischemia underwent detailed history and carotid Doppler examination. IMT on mid common carotid artery (CCA) was measured. All subjects’ blood was taken for biochemical estimation of fasting blood sugar and total cholesterol levels.
Results:
Out of 1,392 subjects, 571 (41%) had abnormal IMT and 821 (59%) had normal IMT. On comparison of the two groups, the factors significantly associated with abnormal IMT were mean older age (59 vs 50.7 years; P < 0.0001) and higher prevalence of hypertension (257 (45%) vs 236 (28.7%); P < 0.0001), diabetes (159 (27.8%) vs 139 (16.9%); P < 0.0001), and hypercholesterolemia (124 (21.7%) vs113 (13.7%); P = 0.0001). After adjustment with multiple logistic regression, significant predictors were age (odds 3.2; 95% confidence interval (CI) 2.5-4.1), male gender (odds 1.5; 95% CI 1.1-1.9), hypercholesterolemia (odds 1.5; 95% CI 1.1-2.0), hypertension (odds 1.4; 95% CI 1.1-1.8), and diabetes (odds 1.3; 95% CI 1.0-1.7).
Conclusion:
We found age, sex, hypertension, diabetes, and hypercholesterolemia to be independent risk factor for abnormal IMT in asymptomatic subjects over 40 years of age.
Keywords: Asymptomatic Indian subjects, IMT, risk factors
Introduction
Atherosclerosis is one of the most common causes of mortality throughout the world and continues to be the leading cause of morbidity in industrialized countries in population more than 45 years of age. But there are major variations in the disease occurrence and incidence in different countries of the world and areas within each country.[1] Extracranial carotid atherosclerosis is the most common cause of stroke in western part of the world. Several studies have identified common carotid artery (CCA) intima-media thickness (IMT) to be independently associated with cerebrovascular and cardiovascular diseases.[2] Few studies have also established carotid IMT as a risk factor for coronary artery disease, stroke, death from myocardial infarction, or a combination of these events.[3,4] The influence of both nonmodifiable and modifiable risk factors on carotid atherosclerosis have been looked at, in the western middle-aged populations.[5,6,7] There is a lack of data from India about carotid atherosclerosis and the factors involved. The aim of this study was to investigate the association between asymptomatic carotid artery IMT and cerebrovascular risk factors in subjects older than 40 years from a tertiary care center in India.
Materials and Methods
This study was carried out in the Neurology department of Nizam's Institute of Medical Sciences (NIMS), Hyderabad, India. NIMS is one of the referral university teaching hospitals in India. One thousand three hundred and ninety-two consecutive, asymptomatic individuals with age ≥40 years and no present or past history of stroke or transient ischemic attack were enrolled into this study. This research study was approved by the Institutional Ethical Committee and the study period was 36 months from September 2003 to August 2006. Data were collected through face-to-face interviews of subjects by a project research fellow, clinical examination by the principal investigator, and a detailed medical record review. Standard techniques were used to measure height, weight, fasting blood sugar, blood pressure, specimen lipids (including total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), very LDL (VLDL), and triglycerides), and glucose.[8]
Hypertension was defined as per the guidelines of Joint National Committee VI-VII.[9] Diabetes was diagnosed according to World Health Organization (WHO) criteria.[10] Smokers were defined as those reporting daily smoking. Ex-smokers and occasional smokers were classified as non-smokers.[11] Alcoholics were defined as those in whom the alcohol consumption was >50 g/day.[12] Hypercholesterolemia was defined as per the guidelines of the National Institutes of Health (NIH), USA, (2001).[13]
When possible, data were obtained directly from subjects, by use of the standardized data collection instruments. When the subjects were unable to provide answers, proxy, or his/her close blood relations, knowledgeable about the subject's history were interviewed.
Color doppler
The ultrasonographic examination was performed by two qualified radiologists and a stroke specialist experienced in neurosonology. The sonographic evaluation was done using a high resolution duplex ultrasound system, Advance Technical Laboratories (ATL) HDI 3000 duplex with a probe at scanner frequency of 7-10 MHz by two radiologists. The examination included2 cm of CCA and the carotid artery bulb as has been done in previous similar studies. IMT on mid CCA was measured in all subjects. Thickness of IMT greater than 0.08 cm was considered abnormal.[14] In case of discordant report on whether there was abnormal IMT or normal IMT, the case was reviewed and result was decided by the stroke specialist. Figure 1 B mode image of CCA showing normal IMT (0.05 cm). Figure 2 B mode image of CCA showing abnormal IMT (0.10 cm).
Figure 1.
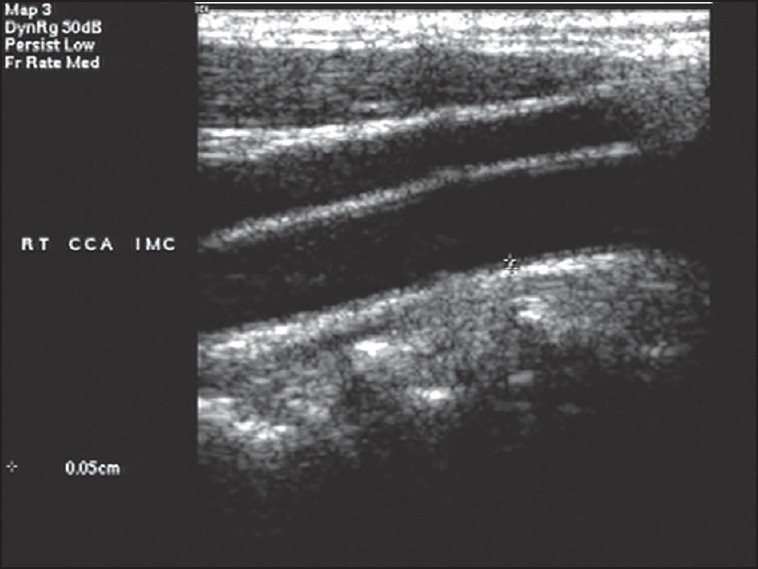
B mode image of common carotid artery showing normal IMT (0.05 cm). IMT = Intima-media thickness
Figure 2.
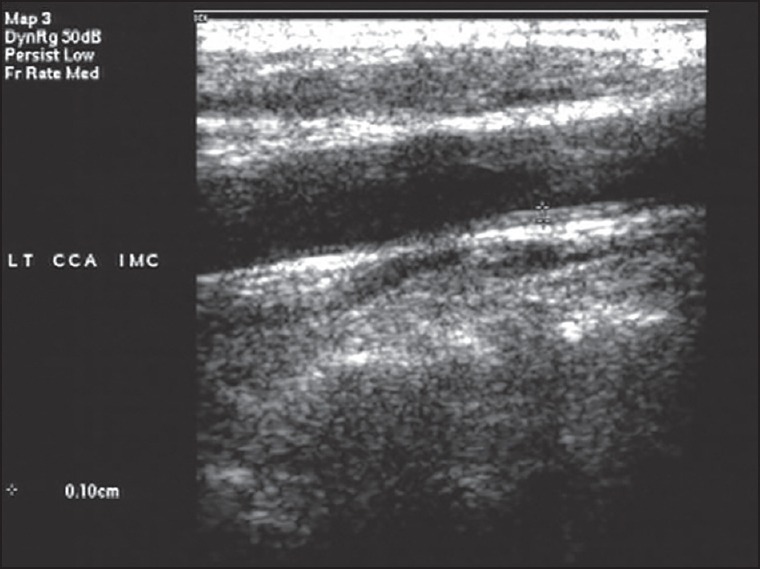
B mode image of common carotid artery showing abnormal IMT (0.10 cm)
Statistical analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) 15.0 window software (SPSS Inc). Continuous variables were presented in titer of mean and ± standard deviation (SD). Interrater correlation amongst the two radiologists was assessed using kappa coefficient. The Student's t-test was used to test the differences in continuous variables, and χ2 test was used to study the association in proportions. We estimated odds ratio (OR) and the resulting 95% confidence interval (CI) for the matched normal IMT and abnormal IMT. Multiple logistic regression was assessed before and after adjustment for potential confounders. All tests were two-sided and P-value <0.05 was considered statistically significant.
Results
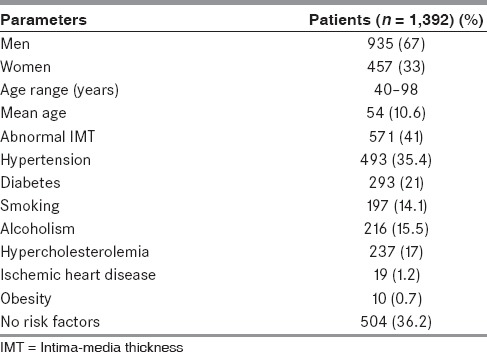
Out of 1,392 subjects, 935 (67%) were men. Mean age was 54 (± 10.6) years ranging from 40 to 98 years and 571 (41%) had abnormal IMT. There was a good interrater correlation between the two radiologists with a kappa coefficient of 0.9. On evaluation of risk factors, 493 subjects (35.4%) had hypertension, 293 (21%) had diabetes mellitus, and 237 (17%) had hypercholesterolemia. Smokers constituted 14.1%, while 15.5% of subjects were alcoholics. Prior history of ischemic heart disease was noted in 19 subjects (1.2%), 10 (0.7%) had obesity, and the remaining 504 (36.2%) asymptomatic individuals had no risk factors [Table 1].
Table 1.
Baseline characteristics
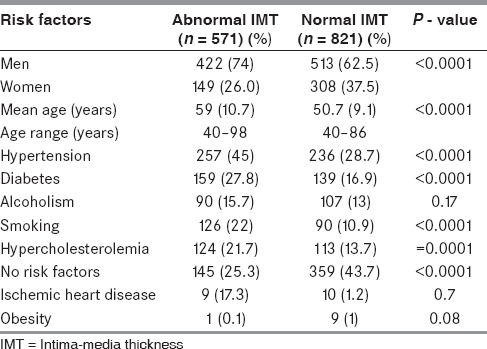
We compared the two groups, 571 subjects with abnormal IMT and 821 with normal IMT. Men were more in abnormal IMT group, that is, 422 (74%) vs 513 (62.5%) in normal IMT group (P < 0.0001). Mean age was 59 (± 10.7) years in abnormal IMT group vs 50.7 (± 9.1) years in normal IMT group (P < 0.00001). On comparison of various risk factors, hypertension was more prevalent (257,45%) in abnormal IMT group compared to 236 (28.7%) subjects in normal IMT group (P < 0.0001). Higher prevalence of diabetes (159,27.8%) in abnormal IMT group versus 139 (16.9%) in normal IMT group (P < 0.0001), hypercholesterolemia (124,21.7%) in abnormal IMT group vs 113 (13.7%) in normal IMT group (P = 0.0001), smoking (126,22%) in abnormal IMT group versus 90 (10.9%) in normal IMT group (P < 0.0001) was seen in abnormal IMT group. Previous history of ischemic heart disease was significantly more (9,17.3%) in abnormal IMT group compared to 10 (1.2%) subjects in normal IMT group (P < 0.0001). There was no difference in alcohol consumption and obesity between the two groups. Subjects with no risk factors were significantly higher in normal IMT group [Table 2].
Table 2.
Differences between abnormal IMT and normal IMT
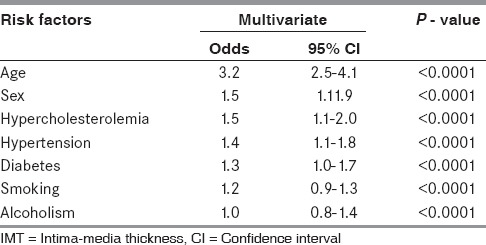
On multiple logistic regression (step wise method) of abnormal IMT with various risk factors, age (OR 3.2, 95% CI 2.5-4.1), sex (men; OR 1.5, 95%CI 1.1-1.9), hypertension (OR 1.4, 95%CI 1.1-1.8), diabetes (OR 1.3, 95%CI 1.1-1.7), and hypercholesterolemia (OR 1.3; 95%CI 1.0-1.6) were independent risk factors of abnormal IMT [Table 3].
Table 3.
Predictors of abnormal IMT
Discussion
Atherosclerosis of the cranial vessels can be easily assessed using carotid IMT. The measurement is simple, based on ultrasound and can be easily performed. The identification of abnormal IMT can help in prevention of cardiovascular and cerebrovascular diseases.[6]
In our study we found abnormal IMT in 41% of asymptomatic subjects. This shows that a large proportion of our population is already at an increased risk of cerebrovascular events and need to be identified.
Abnormal carotid IMT in this study was significantly associated with aging, hypertension, diabetes, and hypercholesterolemia. These results are consistent with the previous studies.[15]
In our study, while one-fifth of subjects less than 50 years had abnormal IMT, more than 80% over 80 years of age had abnormal IMT; thereby, showing a significant and independent correlation between increasing age and abnormal IMT. This is in agreement with several epidemiological studies.[16,17] In the absence of atheroma, the intimal and medial wall of the arteries becomes thicker and more inflexible. Howard et al., observed that there is an yearly increase in IMT of CCAs, by approximately 0.011 mm in men and 0.009 mm in women.[17] Thus, the high frequency of abnormal IMT in the older individuals may not directly translate into a higher risk of cardiovascular events. In fact, studies have noted that an accelerated increase in the IMT of CCAs may be a precursor for cardiovascular events.[18]
We noted that hypertension was seen more frequently in abnormal IMT (45%) compared to normal IMT (28%) group, and this association persisted after multiple logistic regression analysis confirming its independent association. This correlates with the fact that hypertension causes atherosclerosis by causing stress on the vessel wall.[19] A recent meta-analysis has shown that there may be ongoing subclinical atherosclerosis and increased IMT even in subjects with masked hypertension, that is, hypertensive patients with normotension in clinic suggesting a strong association.[19]
Diabetes has been identified as an independent risk factor for abnormal IMT in previous studies.[20] The current study also confirmed that diabetes was significantly associated with abnormal IMT. The relationship of diabetes with atherosclerosis, can however be explained by an alternate hypothesis that inflammation predisposes to both conditions.[21]
Several studies have observed hypercholesterolemia as a known risk factor for increased IMT in adults[7,22] and children.[23] There is also a linear correlation between plasma cholesterol values and IMT.[22,23] We too observed that hypercholesterolemia was significantly associated with abnormal IMT in asymptomatic subjects and was an independent risk factor.
Although on univariate association, smoking was associated with abnormal IMT (P < 0.0001), on multivariate logistic regression analysis, it was not found to be an independent risk factor in our study. This is contrary to previous studies which have noted a strong correlation.[7,22,24] Clinical and experimental studies indicate that either active or passive exposure to smoking promotes vasomotor dysfunction, atherogenesis, and thrombosis in multiple vascular beds.[23,25,26] In our study, the number of subjects who were smokers were lesser, and hence the lack of effect may have been contributed by the small sample size.
Although various studies have shown a correlation between individual risk factors and abnormal IMT, the association of risk factors and their role has not been clearly determined in an Indian population. In our study we did not find a statistically significant increase in the abnormal IMT with increasing risk factors. This may be due to small sample size as most of our subjects had one or two risk factors.
The only number of risk factors may not be important, some risk factors in combination can worsen atherogenecity more than others. Among subjects with combination of two risk factors, diabetes in combination with hypercholesterolemia (OR 3.5, 95% CI:1.2-9.9), hypertension (OR 2.1, 95% CI 1. 36-3.2), or smoking (OR 2.0, 95%CI:0.4-9.1) was associated with an increased risk of developing abnormal IMT. This result was similar to previous studies.[27] Similarly, combination of three risk factors defining metabolic syndrome — diabetes, smoking, and hypertension — had an OR of 7.2, establishing that these combinations are more lethal. Thus, the prevention of modifiable risk factors may prevent atherosclerotic cerebrovascular disease to a large extent.
There are some limitations in the study. It is a simple study which dichotomized the population into normal and abnormal IMT groups. We did not further analyze the actual carotid intima medial thickness which could have further stratified the cerebrovascular risk. Similarly in the risk factors, we only assessed the presence or absence of the various risk factors. Future studies with further stratification based on their treatment and control may help in assessing the effect of the control of modifiable risk factors on the carotid IMT.
Conclusion
This prospective study is the first to look at the effects of various risk factors on carotid IMT in an Indian subcontinent and a large number of asymptomatic subjects were included. This study establishes that abnormal IMT is seen in a significant proportion of asymptomatic Indian subjects, identifying a large proportion of population at risk of cerebrovascular disease. Our study established that age, hypertension, diabetes, and hypercholesterolemia were independently associated with abnormal IMT.
Acknowledgement
This study was supported by a grant from Indian Council of Medical Research, New Delhi, Lr no. SWG/Neuro/8/2001-NCD-1 dated 08-09-2003.
Footnotes
Source of Support: This study was supported by a grant from Indian Council of Medical Research, New Delhi, Lr no SWG/Neuro/8/2001-NCD-1 dated 08-09-2003
Conflict of Interest: None declared.
References
- 1.Prevention of coronary heart disease in clinical practice. Recommendations of the Second Joint Task Force of European and other societies on coronary prevention. Eur Heart J. 1998;19:1434–503. doi: 10.1053/euhj.1998.1243. [DOI] [PubMed] [Google Scholar]
- 2.Burke GL, Evans GW, Riley WA, Sharrett AR, Howard G, Barnes RW, et al. Arterial wall thickness is associated with prevalent cardiovascular disease in middle-aged adults. The Atherosclerosis Risk in Communities (ARIC) Study. Stroke. 1995;26:386–91. doi: 10.1161/01.str.26.3.386. [DOI] [PubMed] [Google Scholar]
- 3.Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, et al. American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima Media-Thickness Task Force. Endorsed by the Society of Vascular Medicine. J Am Soc Echocardiogr. 2008;21:93–111. doi: 10.1016/j.echo.2007.11.011. [DOI] [PubMed] [Google Scholar]
- 4.Fine-Edelstein JS, Wolf PA, O’Leary DH, Poehlman H, Belanger AJ, Kase CS, et al. Precursors of extracranial carotid atherosclerosis in the framingham study. Neurology. 1994;44:1046–50. doi: 10.1212/wnl.44.6.1046. [DOI] [PubMed] [Google Scholar]
- 5.Kiechl S, Willeit J, Egger G, Poewe W, Oberhollenzer F. Body iron stores and the risk of carotid atherosclerosis: Prospective results from the Bruneck study. Circulation. 1997;96:3300–7. doi: 10.1161/01.cir.96.10.3300. [DOI] [PubMed] [Google Scholar]
- 6.Bonithon-Kopp C, Touboul PJ, Berr C, Leroux C, Mainard F, Courbon D, et al. Relation of intima-media thickness to atherosclerotic plaques in carotid arteries. The Vascular Aging (EVA) Study. Arterioscler Thromb Vasc Biol. 1996;16:310–6. doi: 10.1161/01.atv.16.2.310. [DOI] [PubMed] [Google Scholar]
- 7.Howard G, Burke GL, Szklo M, Tell GS, Eckfeldt J, Evans G, et al. Active and passive smoking are associated with increased carotid wall thickness. The Atherosclerosis Risk in Communities Study. Arch Intern Med. 1994;154:1277–82. [PubMed] [Google Scholar]
- 8.Sacco RL, Roberts JK, Boden-Albala B, Gu Q, Lin IF, Kargaman DE, et al. Race-ethnicity and determinants of carotid atherosclerosis in a multiethnic population. The Northern Manhattan Stroke Study. Stroke. 1997;28:929–35. doi: 10.1161/01.str.28.5.929. [DOI] [PubMed] [Google Scholar]
- 9.Britov AN, Bystrova MM. New guidelines of Joint National Committee (USA) on Prevention, Diagnosis and Management of Hypertension. From JNC VI to JNC VII. Kardiologiia. 2003;43:93–7. [PubMed] [Google Scholar]
- 10.Radhakrishnamurthy B. Diabetes mellitus: In heart disease. 2nd editon. Columbus: Quill Publication; 2003. pp. 31–7. [Google Scholar]
- 11.Glader CA, Boman J, Saikku P, Stenlund H, Weinehall L, Hallmanns G, et al. The proatherogenic properties of lipoprotein (a) may be enhanced through the formation of circulating immune complexes containing Chlamydia pneumoniae specific IgG antibodies. Eur Hear J. 2000;21:639–46. doi: 10.1053/euhj.1999.1755. [DOI] [PubMed] [Google Scholar]
- 12.Saposnik G, Caplan LR, Gonzalez LA, Baird A, Dashe J, Luraschi A, et al. Differences in stroke subtypes among natives and caucasians in Boston and Buenos Aires. Stroke. 2000;31:2385–9. doi: 10.1161/01.str.31.10.2385. [DOI] [PubMed] [Google Scholar]
- 13.Radhakrishnamurthy B. Blood lipid: In heart disease. 2nd editon. Columbus: Quill Publication; 2003. pp. 18–27. [Google Scholar]
- 14.Polak JF, O’Leary DH, Kronaml RA, Wolfson SK, Bond MG, Tracy RP, et al. Sonographic evaluation of carotid artery atherosclerosis in the elderly: Relationship of disease severity to stroke and transient ischemic attack. Radiology. 1993;188:363–70. doi: 10.1148/radiology.188.2.8327679. [DOI] [PubMed] [Google Scholar]
- 15.Corrado E, Rizzo M, Tantillo R, Muratori I, Bonura F, Vitale G, et al. Markers of inflammation and infection influence the outcome of patients with baseline asymptomatic carotid lesions: A 5-year follow-up study. Stroke. 2006;37:482–6. doi: 10.1161/01.STR.0000198813.56398.14. [DOI] [PubMed] [Google Scholar]
- 16.Novo S. Influence of risk factors and aging on asymptomatic carotid lesion. Adv Vasc Pathol. Amsterdam: Excerpta Medica; 1997. pp. 36–46. [Google Scholar]
- 17.Howard G, Sharrett AR, Heiss G, Evans GW, Chambless LE, Riley WA, et al. Carotid artery intimal-medial thickness distribution in general populations as evaluated by B-mode ultrasound. ARIC Investigators. Stroke. 1993;24:1297–304. doi: 10.1161/01.str.24.9.1297. [DOI] [PubMed] [Google Scholar]
- 18.Kasliwal RR, Bansal M, Desai D, Sharma M. Carotid intima-media thickness: Current evidence, practices, and Indian experience. Indian J Endocrinol Metab. 2014;18:13–22. doi: 10.4103/2230-8210.126522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cuspidi C, Sala C, Tadic M, Rescaldani M, De Giorgi GA, Grassi G, et al. Untreated masked hypertension and carotid atherosclerosis: A meta-analysis. Blood Press. 2015:1–7. doi: 10.3109/00365521.2014.992185. [DOI] [PubMed] [Google Scholar]
- 20.Paivansalo M, Rantala A, Kauma H, Lilja M, Reunanen A, Savolainen M, et al. Prevalence of carotid atherosclerosis in middle-aged hypertensive and control subjects. A cross-sectional systematic study with duplex ultrasound. J Hypertens. 1996;14:1433–9. doi: 10.1097/00004872-199612000-00008. [DOI] [PubMed] [Google Scholar]
- 21.Wagenknecht LE, D’Agostino RB, Jr, Haffner SM, Savage PJ, Rewers M. Impaired glucose tolerance, type 2 diabetes, and carotid wall thickness: The Insulin Resistance Atherosclerosis Study. Diabetes Care. 1998;21:1812–8. doi: 10.2337/diacare.21.11.1812. [DOI] [PubMed] [Google Scholar]
- 22.Schmidt MI, Duncan BB, Sharrett AR, Lindberg G, Savage PJ, Offenbacher S, et al. Markers of inflammation and prediction of diabetes mellitus in adults (Atherosclerosis Risk in Communities study): A cohort study. Lancet. 1999;353:1649–52. doi: 10.1016/s0140-6736(99)01046-6. [DOI] [PubMed] [Google Scholar]
- 23.Howard G, Wagenknecht LE, Burke GL, Diez-Roux A, Evans GW, McGovern P, et al. Cigarette smoking and progression of atherosclerosis: The Atherosclerosis Risk in Communities (ARIC) Study. JAMA. 1998;279:119–24. doi: 10.1001/jama.279.2.119. [DOI] [PubMed] [Google Scholar]
- 24.Pauciullo P, Iannuzzi A, Sartorio R, Irace C, Covetti G, Di Costanzo A, et al. Increased intima-media thickness of the common carotid artery in hypercholersterolemic children. Arterioscler Thromb. 1994;14:1075–9. doi: 10.1161/01.atv.14.7.1075. [DOI] [PubMed] [Google Scholar]
- 25.Mannami T, Konish M, Baba S, Nishi N, Terao A. Prevalence of asymptomatic carotid atherosclerotic lesions detected by high-resolution ultrasonography and its relation to cardiovascular risk factors in the general population of a Japanese city: The Suita Study. Stroke. 1997;28:518–25. doi: 10.1161/01.str.28.3.518. [DOI] [PubMed] [Google Scholar]
- 26.Deckert T, Feldt-Rasmussen B, Borch-Johnsen K, Jensen T, Kofoed-Enevoldsen A. Albuminuria reflects widespread vascular damage: The Steno hypothesis. Diabetologia. 1989;32:219–26. doi: 10.1007/BF00285287. [DOI] [PubMed] [Google Scholar]
- 27.Salonen R, Salonen JT. Determinants of carotid intima-media thickness: A population based ultrasonography study in eastern Finnish men. J Intern Med. 1991;229:225–31. doi: 10.1111/j.1365-2796.1991.tb00336.x. [DOI] [PubMed] [Google Scholar]