

Abstract
Background:
Aphasia, an acquired inability to understand and/or speak language, is a common repercussion of stroke that denigrates the quality of life (QOL) in the affected persons. Several languages in India experience the dearth of instruments to measure the QOL of persons with aphasia. Malayalam, the language spoken by more than 33 million people in Kerala, the southern state of India, is not an exception to this.
Objective:
This study aimed to adapt and validate the widely-used stroke-aphasia quality of life (SAQOL-39) scale to Malayalam.
Materials and Methods:
We required seven Malayalam-speaking Speech Language Pathologists (SLPs), hailing from different regions of Kerala, to examine the socio-cultural suitability of the original items in SAQOL-39 and indicate modifications, wherever necessary. Subsequently, the linguistic adaptation was performed through a forward-backward translation scheme. The socio-culturally and linguistically adapted Malayalam version was then administered on a group of 48 Malayalam-speaking persons with aphasia to examine the test-retest reliability, acceptability, as well as the internal consistency of the instrument.
Results:
The Malayalam SAQOL-39 scale showed high test-retest reliability (intraclass correlation coefficient, ICC = 0.91) as well as acceptability with minimal missing data (0.52%). Further, it yielded high internal consistency (Chronbach's ∝ = 0.98) as well as item-to-total and inter-domain correlations.
Conclusions:
The Malayalam version of SAQOL-39 is the first socio-culturally and linguistically adapted tool to measure the QOL of persons with stroke-aphasia speaking this language. It may serve as a potential tool to measure the QOL of this population in both clinical practice and future research endeavors.
Keywords: Aphasia, India, Malayalam, quality of life, stroke
Introduction
The quality of life (QOL) is an evolving construct in the domain of healthcare services. In this domain, QOL is more aptly termed as health-related QOL (HRQOL). The HRQOL is an index of persons’ subjective perceptions on various domains of day-to-day functioning. Specifically, it refers to an individual's ability to lead the productive life.[1] Broadly, it has widespread implications in the planning, implementation, and evaluation of healthcare policies as well as in the resource allocation.[2]
Among the various medical conditions, stroke (cerebrovascular accident) is one of the potential detriments to the QOL in the affected persons. The impact of stroke on their life is determined by the functional limitations imposed by this condition. One of the common repercussions of stroke is aphasia, an inability to speak and/or understand language. One in every three persons with stroke experiences aphasia in the acute stage. Further, majority of the aphasic population continue to exhibit linguistic deficits even after 2 years post-onset.[3] In the realm of rehabilitation, the ultimate aim of any medical, surgical, or therapeutic intervention program is to improve the QOL of the affected persons. Aphasia following stroke is not an exception to this philosophy.[2] However, unlike many other post-stroke conditions, aphasia necessitates the use of language-specific tools to measure the QOL in the affected persons.
In the past, questionnaires have been the mainstay of the assessment of health- and non-health-related QOL. Within the healthcare domain, the abundant use of generic QOL instruments in the past have recently given way to disease-specific tools as the latter tools are specifically tailored to measure the impact of specific diseases on persons’ life. Further, several refinements have been incorporated to the existing generic QOL instruments to make them sensitive to specific diseases/conditions. For instance, Hilari and co-workers[1] refined the stroke-specific quality of life (SS-QOL) to measure the QOL of people with aphasia following the stroke (Stroke-Aphasia Quality of Life – SAQOL scale). These authors evaluated the psychometric properties of the initial SAQOL version (containing 53 items) and refined it to a shorter version consisting of 39 items (SAQOL-39). Since then, the SAQOL-39 has been adapted to several languages both in India (Kannada[4] & Hindi[5]) as well as around the world (e. g., Spanish[6], Italian[7]). Such adaptations not only provide sensitive tools to various languages, but also foster cross-linguistic and cross-cultural comparison of QOL data across the centers and nations.[5]
The QOL of persons with aphasia in India
To draw inferences on the QOL of persons with aphasia in India is rather difficult as the prevalence of this condition in Indian population is not readily available. However, some estimation could be made from the prevalence of stroke in India. For example, about 203 persons in 100,000 experience stroke in India.[8] Combining the argument that aphasia is common in a third of the total stroke population[3] with the colossal population of the country, it may be inferred that several thousands of people experience aphasia in India. The intricacy is further raised by the multi-lingual status of the country, which, in turn necessitates the development of QOL instruments in each language. In this context, there has been a recent surge of interest in devising language-specific tools to measure the QOL of persons with aphasia in the Indian context. These tools[4,5] have taken utmost care to circumvent the latent problems associated with the mere translation of tools developed for western culture to the Indian context. Yet, many languages in India continue to experience the dearth of socio-culturally and linguistically validated tools to assess the QOL of persons with aphasia. Malayalam, the language spoken by more than 33 million people[9] in Kerala (the south-western state in India) is not an exception to this. In this context, we aimed to linguistically and socio-culturally adapt the globally-used SAQOL-39 in English to Malayalam in this study.
Materials and Methods
This study followed the methods used in an earlier study that adapted the original English version of SAQOL-39 to Kannada.[4] The corresponding author of the original study granted permission to adapt the original instrument to Indian languages. The socio-cultural adequacy of items in the original version to the Malayalam-speaking community was examined by seven speech-language pathologists (SLPs) hailing from this state. These SLPs were required to examine all 39 items for their social and cultural adequacy and suggest modifications, wherever needed. All SLPs agreed upon the entire items except one (i. e., Upper Extremities Function [UE2: Putting on socks]). After holding discussion with these SLPs, an alternate item was identified (i. e., brushing teeth) to replace the original item. Subsequently, for the purpose of linguistic adaptation, we selected 9 bilingual (Malayalam-English) SLPs from various parts of Kerala to derive a Malayalam version that is compatible with the dialectical variations of this language. Five SLPs were required to translate the original English version to Malayalam (i. e., forward translation) and remaining 4 were required to translate the forward-translated Malayalam version to English (i. e., backward translation). On instances of linguistic/dialectic differences, consensus was obtained among the SLPs in each phase of the translation by way of mutual discussion with them. This led to the backward translated English version that was essentially similar to the original version. Thus, the linguistic adaptation of SAQOL-39 from English to Malayalam was accomplished.
We administered the socio-culturally and linguistically adapted Malayalam version of SAQOL-39 to 48 Malayalam-speaking persons with aphasia residing in Kerala. They were identified from the medical records of our hospital. We collected data from all those persons with chronic aphasia (months post-onset ≥ 6 months)[10] following stroke and excluded those who were suffering from non-stroke-related conditions such as dementia, heart disease, acquired immuno deficiency syndrome (AIDS), metastatic carcinoma, and/or uncorrected peripheral visual impairments.
Psychometric evaluation
Test-retest reliability
We re-administered the Malayalam SAQOL-39 on 10 participants with aphasia within 30 days from the date of initial administration to assess the test-retest reliability. The intraclass correlation coefficient (ICC) was computed from the scores of both administrations using Statistical Package for the Social Sciences (SPSS) (Version 16). The ICC showed excellent test-retest reliability (ICC = 0.91) of the newly adapted version of SAQOL-39 in Malayalam.
Acceptability
Based on the scores from 48 participants in this study, the Malayalam SAQOL-39 showed high acceptability as evidenced by the nominal missing data (0.52%; arising from two items [M4 and M6: 0.26% each]) and non-skewed distribution of scores on all but one item (FR7: -1.2: cut-off: + 1 to -1).
Internal consistency
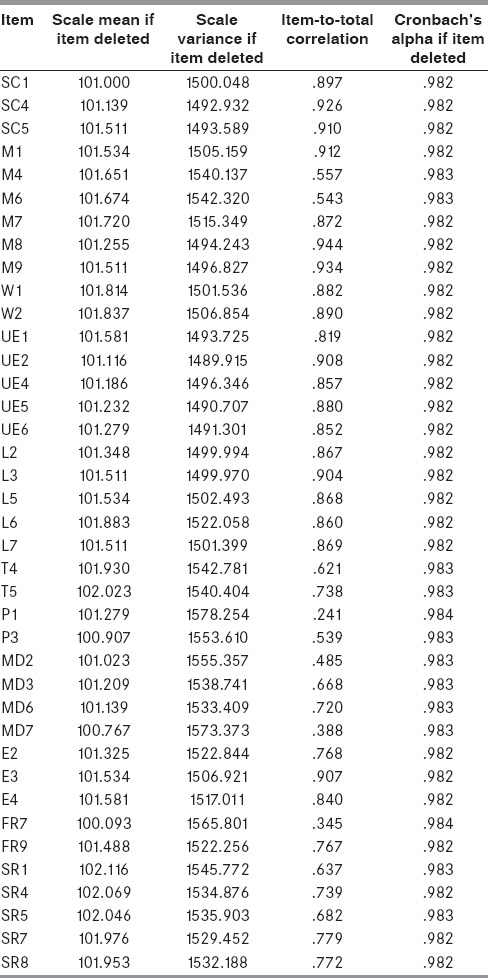
We calculated the Chronbach's alpha (∝) to assess the internal consistency of the Malayalam SAQOL-39. Chronbach's ∝ reflects the correlation between each item and the remaining (total) items in the instrument. Values of ∝ closer to 1 are, therefore, indicative of high item-to-total correlation. This, in turn, signals the high internal consistency of the instrument. The Malayalam SAQOL-39 scale showed an extremely high value of ∝ (0.98), thus ensuring high internal consistency of the scale. Table 1 provides the item-to-total correlations of all 39 items in the new version of the instrument. Additionally, we assessed the internal consistency of items within each domain of Malayalam SAQOL-39 scale. These analyses also revealed high levels of ∝ in each domain (Physical: 0.982; Communication: 0.956; Psychosocial: 0.879; Energy: 0.902) of the newly adapted instrument.
Table 1.
Item-to-total correlation of 39 items in Malayalam version of stroke-aphasia quality of life (SAQOL)-39
Within-scale analysis
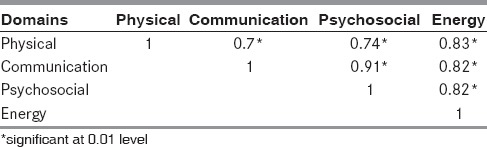
We examined the correlation between various domains of Malayalam SAQOL-39 scale. The results showed significant correlation (P < 0.01) among all four domains [see Table 2].
Table 2.
Inter-domain correlation coefficients
The QOL of people with aphasia
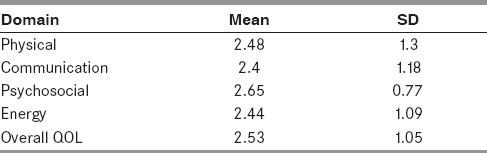
Finally, the data obtained from 48 participants enrolled in this study were used to assess their QOL. For this purpose, we calculated the mean scores of each domain as well as the overall mean QOL scores. The mean overall QOL of our participants with aphasia was 2.53 (standard deviation, SD = 1.05) and the domain-specific mean scores are provided in Table 3.
Table 3.
The group mean (standard deviation, SD) scores of the overall items as well as the four sub-domains of Malayalam stroke-aphasia quality of life (SAQOL)-39 (n = 48)
Discussion
Considering the lack of validated and published instruments to measure the QOL of Malayalam-speaking persons with aphasia, this study aimed to adapt a widely-used instrument (SAQOL-39) from English to Malayalam and examine some of the essential psychometric properties of the same. We exercised utmost care to avoid the inaptness of mere translation of instruments designed for western population to Indian scenario by socio-culturally adapting the original English version to Indian population under consideration. For this purpose, we required seven SLPs hailing from different regions of Kerala examine the socio-cultural adequacy of all 39 items and suggest modifications wherever necessary. The single item of disagreement was UE7 (putting on socks). After holding simultaneous discussion with all seven SLPs, this item was replaced by another consensual item that tapped the function of upper extremities (brushing teeth). This procedure yielded the socio-culturally adapted version of SAQOL-39 in English for the purpose of next (i. e., linguistic) adaptation.
The translation of original English version to Malayalam was accomplished through a forward-backward translation scheme. This has been an established practice to retain the originality of the contents that may be lost during the translation process.[4,5] While the SLPs (n = 5) in the forward translation scheme translated the original English version to Malayalam, those (n = 4) in the backward scheme translated the Malayalam (i. e., translated version) to English. This backward translated English version was compared with the original version to ensure that there were no notable differences between the two versions. Instances of disparities in the usage of words, primarily arising from the regional and dialectical differences in Malayalam, were resolved through a simultaneous consensual discussion with the translators. This ensured the linguistic suitability of the newly adapted version of SAQOL-39 scale to subtle regional/dialectical variations in Malayalam.
The socio-culturally and linguistically adapted Malayalam version of SAQOL-39 was subsequently administered on a group of 48 persons with aphasia following stroke. Their scores were used to establish certain psychometric properties of this instrument. The Malayalam SAQOL-39 scale exhibited high test-retest reliability (ICC = 0.91) and internal consistency (∝ = 0.98), which in turn, were comparable to that of the original (English) version (ICC = 0.98; ∝ = 0.93)[11] as well as the recently adapted versions to Kannada (ICC = 0.8; ∝ = 0.9)[4] and Hindi (ICC = 0.9; ∝ = 0.98).[5] Further, the items within each domain also exhibited high internal consistency (Physical: ∝ = 0.982; Communication: ∝ = 0.956; Psychosocial: ∝ = 0.879; Energy: ∝ =0.902), thus ensuring high within-domain consistency. Finally, all four domains showed significantly high correlation among each other [see Table 2]. Essentially, previous adaptations to Indian languages[4,5] also showed similar findings on such psychometric properties.
The mean (overall) QOL of the participants in this study was 2.53 (SD = 1.05) on a scale of 1 to 5. Comparable, yet minimally higher QOL scores were obtained in Kannada- (Mean = 2.69; SD = 1.05)[4] and Hindi-speaking (Mean = 2.71; SD = 0.95)[5] persons with aphasia in the Indian context. The mean (overall) QOL data from the present study also substantiated the earlier observation[5] that the QOL of persons with aphasia in India is markedly lower compared to their counterparts in Europe (Spanish: Mean = 3.75; SD = 0.86; English: Mean = 3.26; SD = 0.7).[1,6] These observations substantiate the usefulness of the current instrument in cross-centric comparison of QOL data in persons with aphasia.
Conclusion
The Malayalam SAQOL-39 scale is a valid, reliable, and robust instrument like its original version in English and adaptations to various other languages. It may serve as a potential tool to measure the QOL of this population in both clinical practice and future research endeavors. Further, it facilitates comparison of cross-cultural and cross-linguistic QOL data from people with aphasia following the stroke across centers.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Hilari K, Byng S, Lamping DL, Smith SC. Stroke and Aphasia Quality of Life Scale-39 (SAQOL-39): Evaluation of acceptability, reliability, and validity. Stroke. 2003;34:1944–50. doi: 10.1161/01.STR.0000081987.46660.ED. [DOI] [PubMed] [Google Scholar]
- 2.Worrall LE, Holland AL. Quality of life in aphasia. Aphasiology. 2003;17:4. [Google Scholar]
- 3.Palmer R, Cooper C, Enderby P, Brady M, Julious S, Bowen A, et al. Clinical and cost effectiveness of computer treatment for aphasia post stroke (Big CACTUS): Study protocol for a randomised controlled trial. Trials. 2015;16:1–12. doi: 10.1186/s13063-014-0527-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kiran S, Krishnan G. Stroke and aphasia quality of life scale in Kannada-evaluation of reliability, validity and internal consistency. Ann Indian Acad Neurol. 2013;16:361–4. doi: 10.4103/0972-2327.116932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mitra H, Krishnan G. Adaptation and validation of Stroke-Aphasia Quality of Life (SAQOL-39) scale to Hindi. Ann Indian Acad Neurol. 2014 doi: 10.4103/0972-2327.144276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lata-Caneda MC, Pineiro-Temprano M, Garcia-Fraga I, Garcia-Armesto I, Barrueco-Egido JR, Meijide-Failde R. Spanish adaptation of the Stroke and Aphasia Quality of Life Scale-39 (SAQOL-39) Eur J Phys Rehabil Med. 2009;45:379–84. [PubMed] [Google Scholar]
- 7.Posteraro L, Formis A, Bidini C, Grassi E, Curti M, Bighi M, et al. Aphasia quality of life: Reliability of the Italian version of SAQOL-39. Eura Medicophys. 2004;40:257–62. [PubMed] [Google Scholar]
- 8.Anand K, Chowdury D, Sing KB, Panday CS, Kapoor SK. Estimation of mortality and morbidity due to strokes in India. Neuroepidemiology. 2001;20:208–11. doi: 10.1159/000054789. [DOI] [PubMed] [Google Scholar]
- 9.New Delhi: Office of the registrar general and census commissioner, India; [Last accessed on 2014 Mar 11]. censusindia.gov.in [Internet] Available from: http://www.censusindia.gov.in/2011-prov-results/prov_data_products_kerala_.html . [Google Scholar]
- 10.Eldar R. Integrated stimulation — community rehabilitation in developed countries: A proposal. Disabil Rehabil. 2000;22:266–74. doi: 10.1080/096382800296728. [DOI] [PubMed] [Google Scholar]
- 11.Hilari K, Lamping DL, Smith SC, Northcott S, Lamb A, Marshall J. Psychometric properties of the Stroke and Aphasia Quality of Life Scale (SAQOL-39) in a generic stroke population. Clin Rehabil. 2009;23:544–57. doi: 10.1177/0269215508101729. [DOI] [PubMed] [Google Scholar]