

Abstract
Introduction: There is a dearth of literature on tetralogy of fallot (TOF) in children in Sub-Saharan Africa. This study up aims to describe the prevalence, clinical profile and associated cardiac anomaly of children diagnosed with TOF documented over an eight year period in a tertiary hospital in South Western Nigeria.
Methods: A prospective review of all consecutive cases of TOF diagnosed with echocardiography at the Lagos State University Teaching Hospital (LASUTH) between January 2007 and December 2014. Data were analyzed using SPSS version 20. Tables and charts were used to depict those variables. Descriptive statistic are presented as percentages or means and standard deviation. Means of normally distributed variables were compared using the student t test and proportions using chi-square test. Skewed distribution were analyzed using appropriate non-parametric tests. Level of significance set at P < 0.05.
Result: The prevalence of TOF among children presenting at LASUTH at the study period was 4.9 per 10 000 while its prevalence among those with congenital heart disease was 16.9%. There was a male predominance and most children presented within 1-5 years of age. Chromosomal abnormalities such as Down syndrome, Turners syndrome and CATCH 22 syndrome were documented in some subjects. Some of the subjects had atypical presentation.
Conclusion: TOF is as common in Nigeria as other parts of the world, there is a need to established cardiac centers to salvage these children. Collaboration from developed countries will be helpful in this resource limited region.
Keywords: Tetralogy, Fallot, Profile, Nigeria, Africa
Introduction
Tetralogy of fallot (TOF) is the most common cyanotic heart lesion beyond the neonatal period1 and it accounts for a third of all congenital heart disease in patients less than 15 years of age.2 It occurs in 10% of all congenital heart disease.3 The prevalence of TOF is approximately 3.9 per 10 000 live births in the United States4 and 10%-26.2% of all congenital heart diseases in Nigeria.4-11
Diagnosis of TOF is confirmed with echocardiography.3 Definitive diagnostic features and other associated cardiac abnormalities can be identified. In advanced countries, diagnosis can be made in as early as 12 weeks of gestation with fetal echocardiopgraphy.12,13
Management is both medical and surgical and depends on the degree and type of right ventricular outflow tract obstruction and the centre’s protocol.3 There is a dearth of literature on TOF in children in Sub-Saharan Africa. This study aim to describe the prevalence, clinical profile and associated cardiac anomaly of children diagnosed with TOF documented over an eight year period in a tertiary hospital in South Western Nigeria.
Materials and Methods
Prospective and cross-sectional, involving all cases of TOF diagnosed with echocardiography at the Lagos State University Teaching Hospital,( LASUTH) between January 2007 and December 2014. The center is a tertiary hospital in South Western Nigeria. The Hospital receives referral from the South Western region and is the largest center that admits pediatric cases.
A pediatric cardiologists reviewed all the subjects referred for evaluation. A GE Vivid Q echocardiography machine with reference number 14502 WP SN 2084 with appropriate sized probes was used throughout the study period and the pediatric cardiologists performed the echocardiography on all the study subjects. Definitive diagnosis of TOF was made with echocardiography.3
The data were analyzed using SPSS version 20. The prevalence of TOF was calculated from all children who presented in the hospital as in-patient and out-patient during the study period. The prevalence of TOF was also calculated amongst those with congenital heart lesions and those with cyanotic congenital heart disease. Tables and charts were used to depict those variables. Descriptive statistic are presented as percentages or means and standard deviation. Means of normally distributed variables were compared using the student t-test and proportions using chi-square test. Skewed distribution were analyzed using appropriate non-parametric tests. Level of significance set at P < 0.05
Results
Prevalence of Tetralogy of Fallot
A total of 155 patients with echo diagnosis of TOF were documented between January 2007 and December 2014 with a total of 315 150 patients seen as out-patient and in-patient at the study centre during the study period hence the prevalence of TOF amongst the children who were seen in the hospital during the study period was 4.9 per 10 000. A total of 983 had congenital heart disease while 311 of the 983 patient with congenital heart disease had cyanotic congenital heart disease therefore, TOF accounted for 15.8% and 49.8% of congenital heart disease and cyanotic congenital heart disease respectively. Table 1 depicts the prevalence of TOF in the study subjects. Table 2 illustrates the prevalence of TOF in other countries.
Table 1 . Yearly Prevalence of TOF at the Study Center .
| Year | CHD (n) | CCHD (n) | TOF (n) | % of TOF in CHD | % of TOF in CCHD |
| 2007 | 87 | 22 | 13 | 14.9 | 59.1 |
| 2008 | 119 | 29 | 10 | 8.4 | 34.5 |
| 2009 | 90 | 23 | 18 | 20 | 86.9 |
| 2010 | 103 | 36 | 12 | 11.6 | 33.3 |
| 2011 | 153 | 48 | 27 | 17.6 | 56.3 |
| 2012 | 143 | 47 | 26 | 18.2 | 55.3 |
| 2013 | 180 | 65 | 27 | 33.7 | 41.5 |
| 2014 | 108 | 41 | 12 | 11.1 | 29.3 |
| Total | 983 | 311 | 155 | 15.8 | 49.8 |
Abbreviations: CHD, congenital heart disease; CCHD, cyanotic congenital heart disease; TOF; tetralogy of Fallot.
Table 2 . Country Prevalence of TOF in CHD .
| City/Country | Author | Year a | Percent b |
| Malawi | Kennedy and Miller14 | 2013 | 17.9 |
| Zimbabwe | Bannerman et al15 | 1998 | 19.6 |
| Iran | Rahim et al16 | 2008 | 16.9 |
| Iraq | Khadim and Issa17 | 2009 | 12.6 |
| India | Kapoor and Gupta18 | 2008 | 4.6 |
| Sudan | El Hag21 | 1994 | 4.2 |
| Saudi Arabia | Alabdulgader22 | 2006 | 3.5 |
| Qatar | Robida et al23 | 1997 | 5.1 |
| Denmark | Laursen24 | 1980 | 5.8 |
| Oman | Subramanyan et al25 | 1998 | 9.6 |
| Taiwan | Shann26 | 1969 | 18.1 |
| Canada | Rose et al27 | 1964 | 8.1 |
Abbreviations: CHD, congenital heart disease; TOF; tetralogy of Fallot.
aYear of publication. bPercentage of TOF in all CHD.
Clinical Presentation
The male to female ratio was 1.7:1. The mean age of the children was 51.6 ± 52.5 (months). Table 3 describes the age groups of the patients. The most common indication for cardiac evaluation in the study subjects was cyanosis with a suspicion of a cyanotic congenital heart disease. 110 (71%) children were clinically cyanosed on presentation. Record of oxygen saturation was documented with pulse oximeter in 89 subjects. 69 of the 89 (77.5%) of the pulse oximeter records had evidence of cyanosis and 63/69 (91%) of the pulse oximeter recordings of cyanosis were truly cyanosed.
Table 3 . Age Groups of the Subjectsa .
| Age Groups | Male | Female | Total | Percent |
| ≤ 6 monthsb | 12 | 8 | 20 | 13.8 |
| > 6 months -12 months | 11 | 9 | 20 | 13.8 |
| >12 month-5 years | 36 | 25 | 61 | 42.1 |
| > 5-10 years | 13 | 1 | 14 | 9.6 |
| Above 10 years | 18 | 12 | 30 | 20.7 |
| Total | 90 | 55 | 145 | 100 |
a The age of four males and five females were missing. The sex and age of one subject was not documented.
b P value = 0.17, x2= 6.4.
Association Syndromes
However, Down syndrome was documented on 7 subjects, 3 had Turners syndrome and one had CATCH 22. This is shown in Figure 1.
Figure 1 .
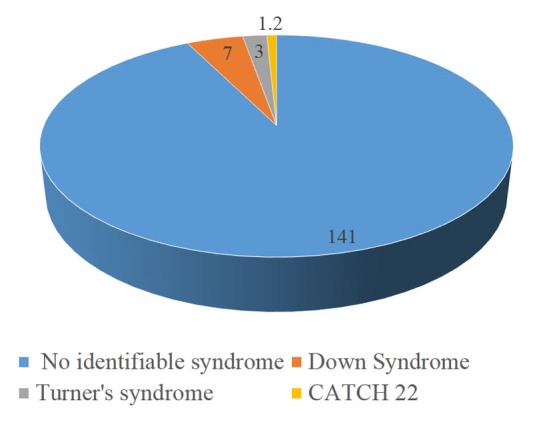
Associated Chromosomal Anomalies/Syndromes.
Discussion
The prevalence of TOF in children in the present study is 4.9 per 10 000 children. This prevalence rate is a hospital based result and thus may not represent the prevalence in the general population. Prevalence rate of TOF have been documented in relation to live birth. A prevalence of 3-6 infants per 10 000 live birth have been reported by Bhmji.2 Population prevalence rate is not known in Sub-Saharan Africa.
The general prevalence of TOF amongst all congenital heart disease is 10%.2,3 Different researchers have reported varying rates depending on the region of study. In the present study, TOF was recorded in 15.8% of all congenital heart diseases. Previous studies in Nigeria have documented rates between 10% and 26.2% in all congenital heart diseases.4-11 Prevalence rate of TOF in all congenital heart diseases in other countries within Africa is between 10 and 19.6%.14-16 Similarly the authors in Africa had different methods, study subjects, and duration. The prevalence rate in other centers in Iran17 and Iraq18 is 16.9% and 12.6%, respectively which is similar with reports in Africa. In India, different authors have recorded rates between 4.6% and 5.5%.19,26
There was a male predominance of TOF in the present study with a male to female ratio of 1.7:1. This finding is similar with other earlier reports.18,19,26 TOF being a cyanotic congenital heart disease, 71% of our subjects presented with cyanosis. Pulse-oximeter is a vital tool in evaluation of patients with congenital heart disease, we were able to document cyanosis using pulse oximeter in up to 91% of the subjects who were cyanosed. Few patients, 5 (3.2%) presented with atypical presentation like gangrene of the right hand and forearm, stroke, cerebral abscess and congestive cardiac failure. Onset of clinical manifestation in patients with TOF depends on the severity of right ventricular outflow tract obstruction.3 Patients may present in neonatal period when there is severe obstruction to right ventricular outflow. The youngest patient was a 2 days old female who was part of a conjoint twin with TOF and pulmonary atresia. Two-thirds of the patients were under 5 years at diagnosis and 60.4% of those were between 1 and 5 years. One-third of the subjects were more than 5 years at presentation. The mean age of the subjects at presentation was 51.6 ± 52.5 in months (4.3 ± 4.4 in years). This mean age is almost similar to that reported by Kennedy and Miller14 in Malawi. Other authors have presented earlier age at diagnosis of TOF.26 However diagnosis of TOF and other congenital heart diseases are usually made between 1-5 years of age, especially in resource poor countries.13,18,27 Possible reasons for the trend of late presentation and diagnosis includes difficulty in assessing specialized care, poverty and poor health seeking behaviour.12,13,17
Chromosomal anomalies have been documented in up to 25% of patients with TOF, the commonest being trisomies and 22q11.2 micro deletion syndromes.3-5 We documented in this study 11 (7.1%) patients with TOF and chromosomal anomalies. There were 7 (4.5%) patient with Down syndrome, 3 (1.9%) of Turners syndrome and 1 (0.65%) case of CATCH 22 syndrome. Risk of recurrence rate for TOF is 3%,3 in this study we had two cases of TOF from the same family, a younger and other sibling.
Patients with TOF may have other associated cardiac defects. In this study, we documented the other associated cardiac lesions in our subjects with TOF. The most common was pulmonary atresia followed by atrial septal defect (ASD). All the patients with ASD had secundum ASD.
Conclusion
We report a prevalence of 4.9 per 10 000 children in this hospital base study. The prevalence of TOF in congenital heart disease is 15.8% and this was similar to other studies within Nigeria and the sub-region. There was a male predominance and most children presented within 1-5 years of age. Chromosomal abnormalities such as Down syndrome, Turners syndrome and CATCH 22 syndrome were documented in some subjects. Some of the subjects had atypical presentation. TOF is as common in Nigeria as other parts of the world, there is a need to established cardiac centers to salvage these children. Collaboration from developed countries will be helpful in this resource limited region.
Acknowledgements
We gratefully acknowledge the children who participated in this study and their parents.
Ethical Issues
Ethical clearance was obtained from the ethical committee of the hospital.
Competing Interests
None to be declared.
Please cite this article as: Animasahun BA, Madise-Wobo AD, Omokhodion SI, Njokanma OF. Children with tetralogy of fallot in an urban centre in Africa. J Cardiovasc Thorac Res 2015;7(4):168-171. doi:10.15171/jcvtr.2015.36.
References
- 1. Perry LW, Neil CA, Ferencz C. EUROCAT working party on congenital heart disease: perspective in pediatric cardiology. Epidemiology of congenital heart disease, the Baltimore – Washington infant study 1981-89 Amok. New York: Futura; 1993:33-62.
- 2. Bhmji S. Tetralogy of fallot. http://emedicine.medscape.com/article/2035949-clinical. Accessed April 25, 2015.
- 3.Balliard F, Anderson R. Tetralogy of Fallot. Orphanet J Rare Dis. 2009;4:2. doi: 10.1186/1750-1172-4-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Antia AU. Congenital heart disease in Nigeria-clinical and necropsy study of 260 cases. Arch Dis Child. 1974;49(1):36–39. doi: 10.1136/adc.49.1.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jaiyesimi F, Antia AU. Congenital heart disease in Nigeria: a ten year experience at UCH, Ibadan. Am Trop Paediatr. 1981;1(2):77–85. doi: 10.1080/02724936.1981.11748065. [DOI] [PubMed] [Google Scholar]
- 6.Ibadin MO, Sadoh WE, Osarogiagbon W. Congenital heart disease at the University of Benin Teaching Hospital. Niger J Paediatr. 2005;32(2):29–32. [Google Scholar]
- 7.Mahmoud U, Mariya M. Spectrum of congenital heart disease in tropical environment: an echocardiography study. J National Med Association. 2007;99(6):665–669. [PMC free article] [PubMed] [Google Scholar]
- 8.Okperi BO. Pattern of congenital heart disease in Delta State University Teaching Hospital, Oghara, Nigeria. Continental J Tropical Medicine. 2012;6(1):48–50. doi: 10.5707/cjtm.2012.6.1.48.50. [DOI] [Google Scholar]
- 9.Adeoye KP, Omotoso PO, Afolabi JK. Pattern of congenital heart disease in Ilorin, Nigeria. Niger Postgrad Med J. 2012;19(4):230–234. [PubMed] [Google Scholar]
- 10.Chinawa JM, Eze JC, Obi I, Arodiwe I, Ujunwa F, Daberechi A. et al. Synopsis of congenital cardiac disease among children attending University of Nigeria Teaching Hospital Ituku Ozalla, Enugu. BMC Res Notes. 2013;6:475. doi: 10.1186/1756-0500-6-475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Asani M, Aliyu I, Kabir H. Profile of congenital heart defects among children at Aminu Kano Teaching Hospital Kano, Nigeria. J Med Trop. 2013;15(2):131–134. [Google Scholar]
- 12.Poon LC, Huggon IC, Zidere V, Allan LD. Tetralogy of Fallot in the fetus in the current era. Ultrasound Obstet Gynecol. 2007;29(6):625–627. doi: 10.1002/uog.3971. [DOI] [PubMed] [Google Scholar]
- 13.Chew C, Halliday JL, Riley MM. Population based study of antenatal detection of congenital heart disease by ultrasound examination. Ultrasound Obstet Gynecol. 2007;29(6):619–624. doi: 10.1002/uog.4023. [DOI] [PubMed] [Google Scholar]
- 14.Kennedy N, Miller P. Spectrum of paediatric cardiac disease presenting to an outpatient clinic in Malawi. BMC Res Notes. 2013;(6):53. doi: 10.1186/1756-0500-6-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bannerman CH, Mahalu W. Congenital heart disease in Zimbabwean children. Ann Trop Paediatr. 1998;18(1):5–12. doi: 10.1080/02724936.1998.11747918. [DOI] [PubMed] [Google Scholar]
- 16.Rahim F, Ebadi A, Saki G, Remazani A. Prevalence of congenital heart disease in Iran: a clinical study. J Med Sci. 2008;6:547–552. [Google Scholar]
- 17.Khadim J, Issa S. Spectrum of congenital heart disease in Basra: an echocardiography study. The Medical Journal of Basra University. 2009;27(1):15–18. [Google Scholar]
- 18.Kapoor R, Gupta S. Prevalence of congenital heart disease, Kanpur India. Indian Pediatr. 2008;45(4):309–311. [PubMed] [Google Scholar]
- 19.Wanni KA, Shahzad N, Ashraf M, Ahmed K, Jan M, Rasool S. Prevalence and spectru of congenital heart disease in children. Indian Heart J. 2014;2:76–79. doi: 10.4103/2321-449x.140230. [DOI] [Google Scholar]
- 20.Chinawa JM, Obu HA, Eke CB, Eze JC. Pattern and clinical profile of children with complex cardiac anomaly at University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu State, Nigeria. Niger J Clin Pract. 2013;16:462–467. doi: 10.4103/1119-3077.116890. [DOI] [PubMed] [Google Scholar]
- 21.El Hag AI. Pattern of congenital heart disease in Sudanese Children. East Afr Med J. 1994;71:580–586. [PubMed] [Google Scholar]
- 22.Alabdulgader AA. Congenital heart disease in Saudi Arabia :current epidemiology and future projections. East Med health J. 2006;12(supp2):157–67. [PubMed] [Google Scholar]
- 23.Robida A, Folger GM, Hajar HA. Incidence of congenital heart disease. Int J Epidemiol. 1988;17:589–594. [Google Scholar]
- 24.Laursen HB. Some epidemiological aspects of congenital heart disease in Denmark. Acta Paediatrica Scandinavica. 1980;69(5):519–524. doi: 10.1111/j.1651-2227.1980.tb07332.x. [DOI] [PubMed] [Google Scholar]
- 25.Subramanyan R, Joy J, Venugopalan P, Sapru A, Al-Khusaiby SM. Incidence and spectrum of congenital heart disease in Oman. Ann Trop Paedaitr. 2000;20:337–41. doi: 10.1080/02724936.2000.11748155. [DOI] [PubMed] [Google Scholar]
- 26.Shann MK. Congenital heart disease in Taiwan, Republic of China. Circulation. 1969;39:251–258. doi: 10.1161/01.cir.39.2.251. [DOI] [PubMed] [Google Scholar]
- 27.Rose V, Body AR, Ashton T. Incidence of congenital heart disease in children in the city of Toronto. CMAJ. 1964;91:95–100. [PMC free article] [PubMed] [Google Scholar]