

Abstract
Workers’ working conditions, work-related health problems and sickness absence are interdependent factors. Both workers’ health problems and their absence are adverse events which generate significant costs for both Poland's Social Insurance Institution (ZUS) and employers. Despite the related burdens, it is difficult to assess the number of workers who experience work-related health problems, to indicate the share of those workers who have been unfit for work owing to such disorders and to indicate the types of workers’ disorders which are caused by factors the workers are exposed to in the working environment. This article presents the findings of surveys carried out in selected production and service-providing companies, assessing the scale and nature of work-related health problems and their links with workers’ sickness absence.
Keywords: work-related health problems, absence from work, presenteeism at work, enterprises
1. Introduction
In 2011, the total number of sick leave absences owing to sickness of the insured at Poland's Social Insurance Institution (ZUS) was nearly 17 million. With the average length of the sick leave being 12 days, this total number corresponded to over 200 million days of sickness absence, which generated significant costs for both ZUS and enterprises.[1] In 2011, the costs of sickness benefits financed from the Social Insurance Fund amounted to more than PLN 7000 million (approximately 0.5% of gross domestic product [GDP]), whereas those financed by employers and from the Fund for Guaranteed Employee Benefits amounted to nearly PLN 4500 million, and a growing tendency can be seen in relation to those costs.[2] It is worth noting that in addition to sickness benefits the costs of absence are also generated by other concurrent factors and relate to, among others, costs of compensation for substitution and overtime, costs of recruitment and training of new workers, costs of loss of and delays in production, as well as other costs associated with reduced work efficiency and quality.[3]
Many survey reports indicate that the scale of workers’ sickness absence is largely related to the working conditions affecting workers’ health. The results of the Fifth European Working Conditions Survey conducted by the European Foundation for the Improvement of Living and Working Conditions (Eurofound) show that nearly 40% of Polish employees believe that work affects their health negatively.[4] Eurostat estimates, however, show that approximately 17% of the general absence of workers is caused by accidents at work and 26% by work-related health problems.[5]
Despite such estimates, it is still very difficult to assess the number of workers who experience work-related health problems and to indicate the share of those workers who have been unable to work owing to such disorders. It is equally hard to indicate which type of workers’ disorders is caused by factors workers are exposed to in the working environment, and this represents an obstacle in designing preventive measures.
The literature on this subject is dominated by surveys which focus exclusively on the analysis of links between several selected factors of the working environment and sickness absence. But there is no information on comprehensive surveys in this regard, which is also confirmed by other researchers.[6]
Many authors see a link between hard manual work and repetitive tasks as well as static strength and musculoskeletal disorders as a cause of sickness absence.[7–9] This is reflected, for example, in pan-European surveys conducted by the European Foundation for the Improvement of Living and Working Conditions,[5] according to which sickness absence in European Union countries is mainly due to musculoskeletal disorders (39% of all sick leave absences lasting 2 weeks or more). Another 19% of all sick leave cases are owing to stress, depression and anxiety, which accounts for 10% of all cases of permanent incapacity to work.[10]
More and more surveys are showing the importance of the influence of psychosocial factors of the working environment on absence from work, e.g., low satisfaction with work, lack of control, high requirements and other stressors.[11–13]
According to Böckerman and Ilmakunnas,[14] the occurrence of at least one harmful and/or dangerous factor causes a significant (7%) increase in the risk of occurrence of sickness absence. The surveys by Melchior et al. [15] show that the links between the working environment-related factors and sickness absence are weaker in the group of healthy workers, and the indicators of absence frequency are twice as high among manual and office workers than among executives and management. It should be added that the influence of working environment-related factors varies by survey and by profession. For example, a survey conducted among nurses from the Norwegian healthcare sector [16] shows that among the factors under assessment (e.g., the level of workload, physical burdens at work, behavioural control, style of leadership, support from the superior, awards for employees, atmosphere at work, conflict of roles and violence at work) only atmosphere at work significantly increases the risk of sickness absence. The researchers were surprised by the lack of relationship between the sickness absence and the significant physical burden or the burden resulting from professional duties and responsibilities.
In their surveys, Bokenblom and Ekblad [17] prove that, particularly among men, a low level of control over work contributes to increased occurrence of short-term absence (of up to 8 days), and the factor negatively related to short-term absence among men was the level of workload, which means that the higher the workload, the lower the frequency of the occurrence of short-term sickness absence. Yet the same workload contributes to an increase in frequency of long-term absence (8 days or more). Increased long-term sickness absence is also driven by the low level of control over work and the lack of support from other co-workers. Similar surveys on reasons for short-term and long-term absence were also conducted in Denmark. The reason for both short-term and long-term absence (10 days or more) among men was low support from executives and poor transparency of tasks. Among women, the reasons for absence were excessive diversity of tasks, excessive requirements and insufficient scope of competence.[18] Lidwall et al. [19] confirm that, since the 1990s, working conditions, in particular the psychosocial working environment, have become more and more relevant in terms of long-term absence caused by illness. Social support at work turned out to be of the highest relevance for absence caused by illness. Also, a significant level of risk associated with ergonomics of the working environment was found to concur with long-term sickness absence for workers of both genders. However, the relationship between significant exposure to harmful factors of the working environment and the sickness absence proved to be relevant for men only.
Other authors of surveys point out that psychosocial working conditions only account for 12–14% of cases of absence caused by illness, which suggests that there are other, more relevant factors which might affect both the number of days of absence and its frequency.[20]
This article presents the findings of surveys carried out in selected production companies, assessing the scale and nature of work-related problems.
2. Methods
The survey focused on work-related health problems defined as disorders whose occurrence or exacerbation had been caused by factors occurring in the working environment. The survey was carried out on a sample of 350 workers employed in 11 production companies, of which 100 were white-collar workers and 250 were blue-collar workers. Pregnant women and workers reporting chronic diseases were excluded. The general description of respondents is presented in Table 1. The average age of the respondents was 40.4 years, and more than one-half of them were younger than 38 years old. The majority of white-collar workers were represented by individuals who have completed university education (women 74%, men 80%) and the majority of blue-collar workers were represented by those who have completed secondary professional education (women 75%, men 57%).
Table 1. Population studied (N = 350).
| N | % | |
|---|---|---|
| Type of work | ||
| Production | 250 | 72.6 |
| Office | 100 | 27.4 |
| Gender | ||
| Women | 175 | 50 |
| Men | 175 | 50 |
| Age (years) | ||
| 18–29 | 67 | 19.4 |
| 30–49 | 202 | 58.4 |
| 50–65 | 77 | 22.2 |
| Education | ||
| Primary and lower secondary | 15 | 4.3 |
| Vocational | 174 | 49.7 |
| Upper secondary | 70 | 20.0 |
| Tertiary | 91 | 26.0 |
| Work experience (years) | ||
| 0–10 | 228 | 67.5 |
| 11–20 | 61 | 18.0 |
| ≥21 | 49 | 14.5 |
An anonymous questionnaire was used for the survey, and was distributed among workers using the envelope method. The questionnaire consisted of questions about the following:
Workers’ perceptions of exposure to harmful and strenuous risk at work, especially chemical substances, dusts, infected materials, noise, vibration, cold and hot microclimate, radiation, electromagnetic fields, hot and cold surfaces, body position, manual handling, repetitive movements, working at height, physical extortion and lighting. Each item presented the workers with a choice of responding either yes or no. The number of positive responses per worker was used as the variable ‘number of physical risks that the employee is exposed to’.
Workers’ perceptions of psychosocial risks concerning four work aspects: increased psychical stress resulting from the nature of work, work organization, work climate and motivation, and job satisfaction (3-point scale with a choice of responding yes, partly or no).
Workers’ perceptions of occurrence of work-related health disorders and other diseases during the last 12 months (including disorders and diseases classified according to the template of medical certificate on temporary incapacity to work issued on the Social Insurance Fund form). In particular, the questionnaire contained questions on the following health disorders and diseases: disorders/diseases relating to respiratory, circulatory, digestive, nervous, genitourinary and musculoskeletal systems; hearing or vision problems; skin problems; mental problems; internal secretion, eating or metabolism disorders; contagious and parasitic diseases; tumours; diseases of blood and blood-forming organs; and chronic fatigue. Again each item presented the workers with a choice of responding either yes or no.
Total absence, determined as a self-reported absence during the last 12 months including: a number of days of formal sick absence (owing to health problems, an accident at work and other reasons) and a number of days during which the worker used their annual leave instead of sick leave.
Workers were also asked to:
estimate the number of sick absences during the last 12 months caused by working conditions, and
report cases of presenteeism of ill employees at work during the last 12 months and their reasons, as well as cases of catching flu or other illnesses from ill workmates present at work during the last 12 months.
Moreover, the respondents were asked to assess the financial situation of their employer, feeling whether their job is safe and the occupational safety and health are properly protected, and assessment of one's health in comparison with the health of other people of the same age (5-point Likert scale).
3. Results
3.1. Work-related health problems
Out of all respondents, 240 (68%) reported work-related health problems, and 69 (19%) of them indicated that this type of problem had caused absence. Within a group of individuals who reported work-related health problems, one-quarter of respondents reported one disorder, 22.5% of respondents two disorders, and the majority (44.5%) reported three to five disorders. In total, all respondents reported 742 work-related health problems.
Most workers reported work-related health problems in the form of musculoskeletal disorders (42%), chronic fatigue (39%), eye disorders (27%), skin diseases (18%) and disorders of the respiratory system (17%) (Table 2).
Table 2. Type of work-related health problems in the population studied according to subjective assessment done by workers (N = 350).
| Type of work-related health problem | N | Workers suffering from health problems (%) |
|---|---|---|
| Musculoskeletal disorders | 148 | 42.29 |
| Chronic fatigue | 139 | 39.71 |
| Vision problems | 97 | 27.71 |
| Respiratory diseases | 61 | 17.43 |
| Skin problems | 64 | 18.29 |
| Circulatory system problems | 43 | 12.29 |
| Mental problem | 43 | 12.29 |
| Hearing problems | 24 | 6.86 |
| Digestive problems | 23 | 6.57 |
| Nervous system problems | 18 | 5.14 |
| Tumours | 11 | 3.14 |
| Internal secretion, eating or metabolism disorders | 13 | 3.71 |
| Contagious and parasitic diseases | 11 | 3.14 |
| Genitourinary system problems | 7 | 2.00 |
| Diseases of blood and blood-forming organs | 9 | 2.57 |
3.2. Presenteeism
Among workers who came to work during the last 12 months even though their health condition indicated the need to take sick leave, there were more office workers (50% of all office workers and 40% production workers). The results of statistical analyses showed that there was a statistically relevant relationship between the type of work (office versus production related) and the presence of sick workers at work and their reasons (3, N = 149, χ 2 = 20.8; p < 0.001). Among office/administration workers, a relatively more frequent motivation was ‘tasks/assignments to be delivered within a deadline’. Production workers came to work more frequently despite sickness because of ‘inner’ motivation (Cramer's V = 0.37; p < 0.001) (Figure 1).
Figure 1.
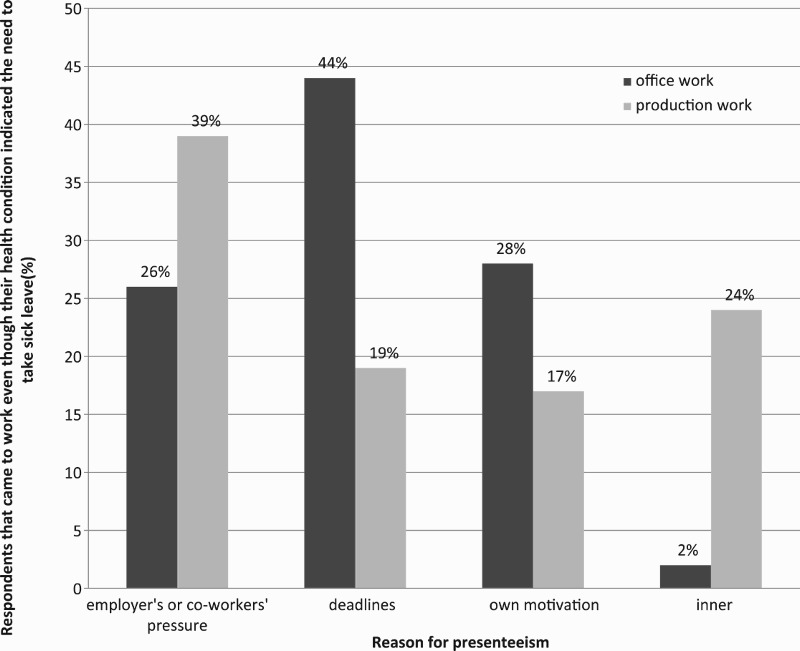
Percentage of respondents that came to work even though their health condition indicated the need to take sick leave by reasons and types of work, N = 350.
Women more often came to work while being sick (44%) than men (41.7%). There is a statistically relevant relationship between gender (men versus women) and the presence of sick workers at work and their reasons (1, N = 150, χ 2 = 18.12; p < 0.001). Among the men a relatively more frequent motivation was ‘tasks/assignments to be delivered within a deadline’. The women came to work more frequently despite sickness because of ‘inner’ motivation (Cramer's V = 0.34; p < 0.001) (Figure 2).
Figure 2.

Percentage of respondents that came to work even though their health condition indicated the need to take sick leave by reasons and gender, N = 350.
More office workers (31%) and women (36%) than production workers (25.6%) and men (18.3%) admitted that during the last 12 months they have contracted a disease from their co-workers, e.g., flu. Statistical analyses have proved that there is a statistically relevant relationship between gender and the chance of contracting flu or other infection from a co-worker (1, N = 350, χ 2 = 18.88; p < 0.001). Being a woman considerably increases the chance of contracting a disease from a co-worker (ϕ = 0.2; p < 0.001) (Figure 3).
Figure 3.

Percentage of respondents that have contracted a disease from their co-workers, e.g., flu, by types of work and gender, N = 350.
3.3. Absence
Total length of absence arising from a worker's own sickness during the last 12 months amounted to 822 days. In total, 14.3% of women and 16.7% of men admitted that during the last 12 months they had used their annual leave instead of sick leave, which produced an additional 250 days (Figure 4). In total, 1072 days were lost owing to sickness (including both sick leave and annual leave) among 35% of the respondents. The average length of total sick absence amounted to 8.6 days.
Figure 4.
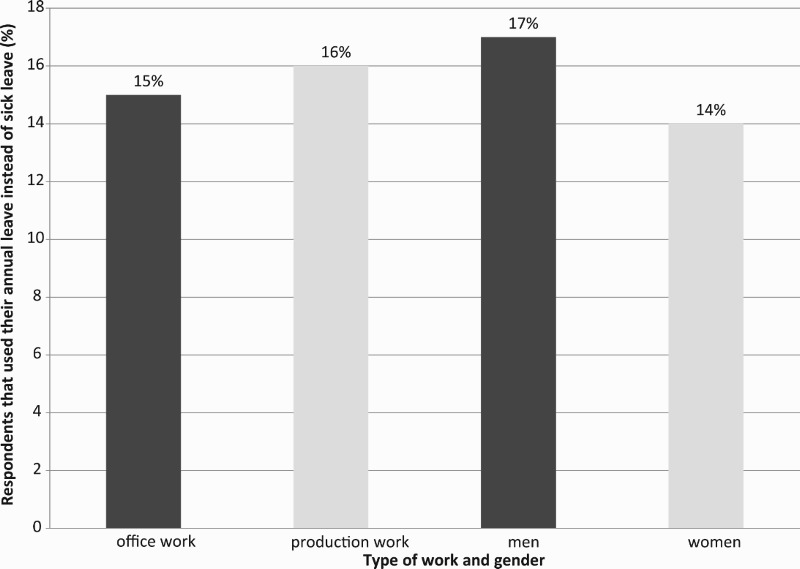
Percentage of respondents that used their annual leave instead of sick leave by types of work and reasons and gender, N = 350.
3.4. Logistic regression
A binary logistic regression analysis was performed to determine the influence of specific variables on the probability of absence, based on their coincidence.
The dependent variable, ‘Total absence’, was constructed as a dichotomous indicator based on the ‘absence/no absence’ opposition, where all the results of the survey different from ‘0’ (coded as ‘no absence’) were coded as ‘absence’. The reason for recoding the variable into a dichotomous one was strong asymmetry in the distribution of the ‘Total absence’ variable with significant over-representation of ‘0’, even after deduction of outliers (skewness = 2.35). The skewness of ‘Absence’ results from the natural reasons, because absence at work is far less frequent than presence at work.
Following the existing theory and research hypotheses, numerous variables were selected as predictor variables in the initial model, including quantitative variables, i.e., number of physical risks that the employee is exposed to, four indicators of psychosocial risk (including indicators of increased psychical stress resulting from nature of work, work organization, work climate and motivation, job satisfaction), a number of health problems, and length of service at current position, and qualitative variables including financial situation of an employer, feeling whether the job is safe and the occupational safety and health are properly protected, and assessment of one's health in comparison with the health of the other people of the same age. The qualitative variables were recorded as dummy variables.
The type of job performed was proven at the earlier stages of the project to be interaction variable, which changes the relationship between specific variables and absence at work. Therefore, analyses were conducted for white-collar workers and blue-collar workers separately.
For white-collar workers, all of the models were statistically insignificant [χ 2(18) = 95.581, p > 0.05], partially because of high over-representation of non-absent workers (74%). For blue-collar workers, the model was well fit to data and statistically significant [χ 2(18) = 95.813, p < 0.001], increasing the prediction level of absence from 60% in the initial model to 77%. Goodness of fit for the model was confirmed by the Hosmer–Lemeshow test, which was not statistically significant [H = 5.533(8), p = 0.7], and by pseudo-R 2 (Nagelkerke R 2 = 0.44). However, because numerous predictors of the model were not statistically significant, they were later excluded from the model. As a result, the enhanced model included the number of physical risks that the employee is exposed to, job satisfaction indicator, number of health problems, length of service at current position (quantitative variables) and financial situation of an employer (qualitative variable). The goodness of fit for the enhanced model was slightly lower [Nagelkerke R 2 = 0.4; H = 9.649(8), p = 0.29] and the enhanced model itself was statistically significant [χ 2(8) = 82.097, p < 0.001]. The majority of variables in the enhanced model were statistically significant except for dummy variables for the financial situation of an employer, which, as a result, was excluded from the model.
The variables included in the final model included the quantitative variables only: A, the number of physical risks that the employee is exposed to; B, a job satisfaction indicator; C, a number of health problems; and D, length of service at current position. The final model was well fitted to the data. It was statistically significant [χ 2(4) = 71.2, p < 0.001], and the prediction level for absence exceeded 75% in comparison with 60% in the initial model. Goodness of fit for the model was confirmed by the Hosmer–Lemeshow test, which was not statistically significant [H = 6.9(8), p = 0.55], and fit for pseudo-R 2 to the final model was satisfactory (Nagelkerke R 2 = 0.35).
The final regression model was as follows:
Seven unusual observations altering the regression parameters were identified, of which five were excluded from the analysis. As the result, the goodness of fit for the model to the data was increased [χ 2(4) = 85.4, p < 0.001; H = 14.7(8), p = 0.07]. The pseudo-R 2 shows better fit as well (Nagelkerke R 2 = 0.42). The prediction level for absence increased from 61% to 78%. The prediction level for lack of absence is still much higher and reaches 92%.
The improved final model is as follows:
According to the model, an increment of the job satisfaction indicator B by 1 (indicator value range is 0–2) lowers the probability of the absence by 58%, an increment of the number of health problems C by 1 increases the probability of absence by 34%, an increment of the number of physical risks that the employee is exposed to A by 1 increases the probability of absence by 15%, and increment of the length of service at current position D by 1 increases the probability of absence by 6%.
4. Discussion and conclusions
The survey results show that the occurrence of work-related health problems is quite frequent in the working population. According to the results of a modular survey entitled ‘Accidents at work and work-related health problems’ conducted in 2007 by Poland's Central Statistical Office (GUS), 41% of workers reported work-related health problems,[21] and on the basis of those results it can be assumed that at some workplaces (particularly production plants) this percentage may be much higher and in one-third of cases it may result in absence.
The survey results are similarly negative in terms of the number of work-related health issues. They show that more than two-thirds of workers report more than one work-related health issue and almost 20% of them stayed on sick leave, whereas in the modular survey by GUS this percentage was slightly more than 50%. Most workers report work-related health problems in the form of musculoskeletal disorders, chronic fatigue, eye disorders and disorders of the respiratory system. Slightly less frequently, workers complain about health problems relating to skin diseases, diseases of the circulatory system or mental problems. As for the type of work-related health problems, it noteworthy that their nature is specific, and their distribution by disease group differs from the diseases being the grounds for the issuance of a medical certificate.[21]
The statistical analyses confirm among production workers a greater number of work-related health problems and higher sick absence. There is also a positive relationship between the number of physical risks that the employee is exposed to and the absence rate, and between the length of service at current position and the absence rate. A negative relationship is observed between job satisfaction and the absence rate. The number of physical risks can be treated as predictors of absence because their influence on people's health is well known in medical research, whereas it is difficult to say the same in relation to job satisfaction that can be both or a predictor or a consequence of absence.[22]
As the days of absence do not reflect the whole issues of health problems, firstly the incidents of presenteesim and its reason were researched. According to the data collected, 40% of respondents admitted they come to work when sick and about one-quarter admitted they contracted a disease from their co-workers, e.g., flu. Findings from another study conducted in Polish enterprises show that costs of presenteeism related only to lower productivity and shortened work time owing to bad health conditions of workers can exceed two to five times the total indirect costs of absence.[23]
Another problem that was touched on in this research is that many workers in Polish enterprises take annual leave while being ill instead of sick leave (according to the research, 15% of respondents). Days of annual leave used by respondents instead of sick leave were included in the total absence that was used in the dependent variable in the logistic regression.
Acknowledgements
The author would like to thank Szymon Ordysiński for participating in statistical analyses and helpful discussion. This article has been based on the results of a research task carried out within the scope of the second stage of the National Programme ‘Improvement of Safety and Working Conditions’ partly supported in 2011–2013 - within the scope of research and development - by the Ministry of Science and Higher Education/National Centre for Research and Development. The Central Institute for Labour Protection – National Research Institute (CIOP-PIB) was the Programme's main coordinator.
Disclosure statement
No potential conflict of interest was reported by the author.
References
- Absencja chorobowa w 2011 roku. Warsaw: ZUS; 2012. [Sick absence in 2011] [Google Scholar]
- Ważniejsze informacje z zakresu ubezpieczeń społecznych 2011 r. Warsaw: ZUS; 2012. [Chief information on social insurance in 2011] [Google Scholar]
- Pęciłło-Pacek M. Koszty absencji chorobowej i działania je ograniczające [Cost of work-related sick absence and activities aimed at reducing it] Bezpieczeństwo Pracy – Nauka i Praktyka. 2012;9:12–15. [Google Scholar]
- Eurofound . Fifth European working conditions survey. Luxembourg: Publication Office of the European Union; 2012. [Google Scholar]
- Eurostat . Work and health in the EU. A statistical portrait (1994–2002) Luxembourg: Office for Official Publications of the European Communities; 2004. [Google Scholar]
- Allebeck P, Mastekaasa A. Swedish council on technology assessment in health care (SBU). Chapter 5. Risk factors for sick leave – general studies. Scand J Public Health Suppl. 2004;32:49–108. doi: 10.1080/14034950410021853. [DOI] [PubMed] [Google Scholar]
- Hartvigsen J, Bakketeig L, Leboeuf-Yde C, et al. The association between physical workload and low back pain clouded by the “healthy worker” effect. Spine. 2001;26(16):1788–1792. doi: 10.1097/00007632-200108150-00011. [DOI] [PubMed] [Google Scholar]
- Niedhammer I, Bugel I, Goldberg M, et al. Psychosocial factors at work and sickness absence in the Gazel cohort: a prospective study. Occup Environ Med. 1998;55(11):735–741. doi: 10.1136/oem.55.11.735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kivimäki M, Vahtera J, Thomson L, et al. Psychosocial factors predicting employee sickness absence during economic decline. J Appl Psychol. 1997;82(6):858–872. doi: 10.1037/0021-9010.82.6.858. [DOI] [PubMed] [Google Scholar]
- Milczarek M, Schneider E, Gonzalez ER. OSH in figures: stress at work — facts and figures. Luxembourg: Office for Official Publications of the European Communities; 2009. [Google Scholar]
- Hoogendoorn W, Bongers P, de Vet H, et al. High physical work load and low job satisfaction increase the risk of sickness absence due to low back pain: results of a prospective cohort study. Occup. Environ Med. 2002;59(5):323–328. doi: 10.1136/oem.59.5.323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grossi G, Soares J, Angesleva J, et al. Psychosocial correlates of long-term sick-leave among patients with musculoskeletal pain. Pain. 1989;80(3):607–620. doi: 10.1016/S0304-3959(98)00253-X. [DOI] [PubMed] [Google Scholar]
- North F, Syme S, Feeney A, et al. Psychosocial work environment and sickness absence among British civil servants: the Whitehall II Study. Am J Public Health. 1996;86(3):332–340. doi: 10.2105/ajph.86.3.332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Böckerman P, Ilmakunnas P. Interaction of working conditions, job satisfaction, and sickness absences: evidence from a representative sample of employees. Soc Sci Med. 2008;67(4):520–528. doi: 10.1016/j.socscimed.2008.04.008. [DOI] [PubMed] [Google Scholar]
- Melchior M, Krieger N, Kawachi I, et al. Work factors and occupational class disparities in sickness absence: findings from the GAZEL cohort study. Am J Public Health. 2005;95(7):1206–1212. doi: 10.2105/AJPH.2004.048835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eriksen W, Bruusgaard D, Knardahl S. Work factors as predictors of sickness absence: a three month prospective study of nurses’ aides. J Occup Environ Med. 2003;60(4):271–278. doi: 10.1136/oem.60.4.271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bokenblom M, Ekblad K. Working conditions, absence and gender – a multilevel study. Working Paper 10. Örebro, Sweden: Örebro University; 2010.
- Nielsen M, Rugulies R, Christensen K, et al. Psychosocial work environment predictors of short and long spells of registered sickness absence during a 2-year follow up. J Occup Environ Med. 2006;48(6):591–598. doi: 10.1097/01.jom.0000201567.70084.3a. [DOI] [PubMed] [Google Scholar]
- Lidwall U, Bergendorff S, Voss M, et al. Long-term sickness absence: changes in risk factors and the population at risk. Int J Occup Med Environ Health. 2009;22(2):157–168. doi: 10.2478/v10001-009-0018-3. [DOI] [PubMed] [Google Scholar]
- Roelen CAM, Koopmans PC, Bultmann U, et al. Psychosocial work conditions and registered sickness absence: a 3-year prospective cohort study among office employees. Int Arch Occup Environ Health. 2009;82(9):1107–1113. doi: 10.1007/s00420-009-0425-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wypadki przy pracy i problemy zdrowotne związane z pracą. Warsaw: GUS; 2008. [Accidents at work and work-related health problems] [Google Scholar]
- Bugajska J, Żołnierczyk-Zreda D, Hildt Ciupińska K. Profilaktyka dolegliwości mięśniowo-szkieletowych w kontekście psychospołecznych aspektów pracy. Bezpieczeństwo Pracy – Nauka i Praktyka. 2011;(4):12–15. [Musculoskeletal ailments prophylaxis In the light of psychosocial work conditions] [Google Scholar]
- Pęciłło M. Szacowanie ukrytych kosztów absencji chorob owej [Estimation indirect costs of sick absence] Bezpieczeństwo Pracy – Nauka i Praktyka. 2013;10(505):13–15. [Google Scholar]