

Abstract
Background:
Poisoning is one of the most common medical presentations in a hospital. Hypoglycemic patients are at increased risk of toxicity. The purpose of this study was to compare capillary blood glucose and venous blood glucose measurements using glucometer against laboratory blood glucose in case of poisoned patients being in coma.
Materials and Methods:
During the 6-month study period, a random sample of 98 patients was admitted in the Department of Poisoning Emergency and Clinical Toxicology of Noor Hospital, Isfahan University of Medical Sciences, Iran from May 2010. Data collected included age, gender, poisoning reason, vital signs, and Glasgow Coma Scale. Capillary blood samples were obtained from the fourth fingertip of the non-dominant hand. t-Test, paired t-test, Pearson's correlation analysis, and one-way analysis of variance (ANOVA) were used for analysis.
Results:
The mean of capillary blood glucose was 115.7 ± 50.2, of venous blood glucose measured by glucose meter was 117.8 ± 47.3, and of glucose measured in vitro was 115.8 ± 55.1. Mean of blood glucose showed no significant difference with the three mentioned methods. The correlation between capillary and intravenous blood glucose samples measured by glucometer was 0.93, between capillary blood glucose and in vitro measured venous blood glucose was 0.78, and between venous blood glucose measured by glucose meter and in vitro measured sample was 0.81. The mean of capillary and venous blood glucose levels measured by glucose meter, capillary and venous blood glucose levels measured in vitro, and venous blood glucose levels measured by glucose meter had no significant differences.
Conclusion:
Using venous blood sample and measuring the glucose level in it by glucometer is an acceptable and advisable method, and capillary blood glucose measurement by using glucometer is not recommended for patients in coma.
Keywords: Blood glucose monitoring, glucometry, poisoned patients
INTRODUCTION
Glucose monitoring is a vital component in the management of critically ill patients (1). Blood glucose measurement can be accomplished by sending a venous sample to the laboratory or by using a blood gas analyzer.[1] Disadvantages with this method include infection, hematoma, nerve damage, bleeding, bruising, higher cost, and increased time consumption. The capillary blood samples are obtained from the patient's fingertip with a lancet device.[2] Although in many centers bedside capillary glucose measurements have become the standard of care, previous literature has raised questions about the disparity between these measured values and those obtained from traditional blood and serum assays from central venous or arterial sources.[3] For example, in Funk et al. study, a weak correlation was obtained between the levels of venous and capillary blood glucose.[4] But in Matthews et al. study, it was observed that when the level of venous glucose was divided by 1.1, capillary blood glucose (CBG) was obtained.[5] In Boyd et al.'s study, a small but significant difference was found between the venous blood glucose checked by glucose meter and in the laboratory, and the CBG checked by glucose meter and in the laboratory.[6] Preponderance of available data suggests that blood glucose levels may have a relationship with the severity of poisoning and the clinical outcome following acute poisoning.[7] In the study of Funk et al., the volunteers were healthy; but in Funk's study, stress might have caused hypoglycemia or hyperglycemia. In Matthews et al.'s study, the patients were diabetic; in the present study, patient history did not reveal presence of diabetes in the past. The number of patients in the present study increased to 98 from 20 in Boyd et al.'s study. The purpose of this study was to compare the capillary and venous blood glucose measurements by using glucometer against the laboratory blood glucose in patients in coma due to poisoning.
MATERIALS AND METHODS
This observational study was conducted in the Department of Poisoning Emergency and Clinical Toxicology of Noor Hospital, Isfahan University of Medical Sciences, Iran from May 2010 until October 2010. A random sample consisting of 98 adult deliberate self-poisoning patients aged 13-50 years was included. They were enrolled over a 6-month period. Exclusion criteria were a history of diabetes mellitus, having received presampling intravenous dextrose solution or glucocorticoids, and poisoning with medications or toxic agents that cause hyper- or hypoglycemia as mentioned in the introduction section. Patients who themselves or their family members were not willing to cooperate were also excluded.
PROTOCOLS
Data on the following were obtained from the patients’ medical records: Age, gender, reason for poisoning or admission diagnosis, vital signs, and Glasgow Coma Scale (GCS). Immediately after ABC (Air way, Breathing, Circulation) and then every 6 h, systolic and diastolic blood pressure, heart rate, pulse rate, and GCS were recorded (GCS of patients was 3/15-14/15). Also, immediately after performing ABC, in all the included patients, one venous sample was taken for measurement of glucose, blood urea nitrogen (BUN)/creatinine (Cr), Na/K, prothrombin time (PT)/partial thromboplastin time (PTT), complete blood count (CBC)/differential analysis at fixed time intervals. Simultaneously, venous sample glucose level was determined with a glucometer; also, capillary (finger stick) glucose determination was performed. Capillary blood sample was obtained from the fourth fingertip of the non-dominant hand[8] by using a lancet device and laboratory samples were obtained from a peripheral venous in all patients. Laboratory blood glucose was analyzed in the hospital central laboratory.
The clinical severity of poisoning was graded according to the method described by Person and coworkers, and developed by the International Program on Chemical Safety, the European Community, and the European Association of Poisons Centers and Clinical Toxicologists (IPCS/EC/EAPCCT).[7] The poisoning severity score (PSS) is a four-point scale graded as (0) none, (1) minor, (2) moderate, (3) severe, and (4) fatal.[9,10] All patients received medical treatment under the direction of the hospital's consultant physicians. Five patients themselves or their family members were not willing to cooperate and, therefore, were excluded. Also, three of the other patients died during research, so their data were eliminated from the study. Therefore, the final study sample consisted of 90 patients. In addition, the date and time of all capillary and laboratory blood glucose (CBG and LBG, respectively) values obtained during the stay in the department were recorded and compared with the date strips because the strips may be out of date, which could decrease the accuracy.
Glucose measurements
Blood samples were obtained immediately after ABC. In cases of hypoglycemia, the glucose level was checked every hour using a glucose meter until the normal blood glucose levels were obtained. Blood glucose levels on admission were divided into hypoglycemic (<70 mg/dl), normoglycemic (70-126 mg/dl), and hyperglycemic (>126 mg/dl) values.[11]
Statistical methods
The mean difference between CBG and LBG was calculated for each measurement. Agreement was considered if the difference between them did not exceed 15%. Agreement between CBG and LBG was compared during shock and non-shock states and within hypoglycemic and hyperglycemic subgroups. Bias between measurements was defined as the mean of the difference between measurements, precision as the standard deviation of the differences between measurements, and the 95% upper and lower limits of agreement as ±2 standard deviation (SD) from the mean bias.[1]
Statistical analyses were performed by SPSS. Data are presented as mean ± SD. The t-test and paired t-test, Pearson's correlation analysis, and one-way analysis of variance (ANOVA) method were used. A two-sided P value of less than 0.05 was considered significant. Correlation and linear regression analyses were performed.
RESULTS
Ninety poisoned patients with the mean age of 24.8 ± 8.1 years were studied and investigated in the present study. Among them, 39 were females and 51 were males (43.3% and 56.7%, respectively). The mean age of the studied females and males were 24.1 ± 8.1 and 25.3 ± 8.2 years, respectively; according to the t-test, there was no significant difference between both sexes (P = 0.47). The frequency percentage of intoxication factors in the study sample is shown in Figure 1. It is observed that the most common intoxication factor is drug consumption. In Table 1, the mean and standard deviation of blood pressure, pulse, and respiration of all patients and for each sex are shown. The t-test performed on the above-mentioned data revealed that the hemodynamic variables showed no significant differences in terms of sex.
Figure 1.
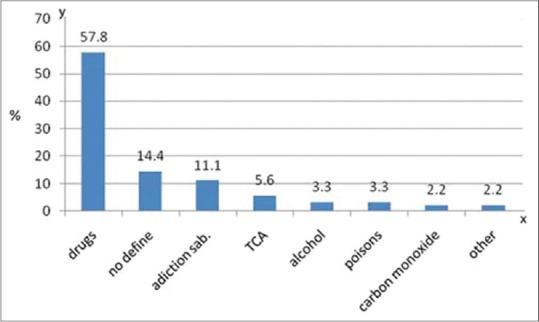
Frequency distribution of poisoning causes
Table 1.
Mean and standard deviation of hemodynamic variables P > 0.05

In the studied patients, the mean of GCS index was 10.6 ± 3.4. 10.6 ± 3.3 in females and 10.5 ± 3.5 in males; t-test showed no significant difference between both sexes (P = 0.89).
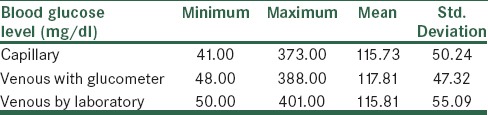
Based on the obtained results, the mean of CBG was 115.7 ± 50.2, venous blood glucose measured by glucometer was 117.8 ± 47.3, and venous blood glucose measured in vitro was 115.8 ± 55.1; one-way ANOVA test showed no significant difference in the mean of blood glucose level measured by the three methods (P = 0.95). Also, in Figure 2, the obtained results show that there was a correlation between CBG and venous blood glucose measured by glucometer to a level of 0.93, which was significant according to the Pearson correlation test (P < 0.001). In Figure 3, the correlation between CBG and venous blood glucose measured in vitro was 0.78; this correlation was also statistically significant. Finally, in Figure 4, the correlation rate between venous blood glucose measured by glucometer and in vitro was 0.81, which was statistically significant (P < 0.001). The correlation between the levels of venous blood glucose and CBG (by glucometer) measured with the methods mentioned is shown in Figure 2. On the other hand, performing paired t-test on the obtained data showed that the mean of capillary and intravenous blood glucose levels measured by glucometer had no significant differences (P = 0.28). The mean of measured capillary and venous blood glucose levels had also no significant difference in vitro (P = 0.98). Also, the mean of venous blood glucose levels measured by glucometer and in vitro had no significant difference (P = 0.56). The mean and standard deviation of blood glucose level with the three mentioned methods are shown in Table 2.
Figure 2.
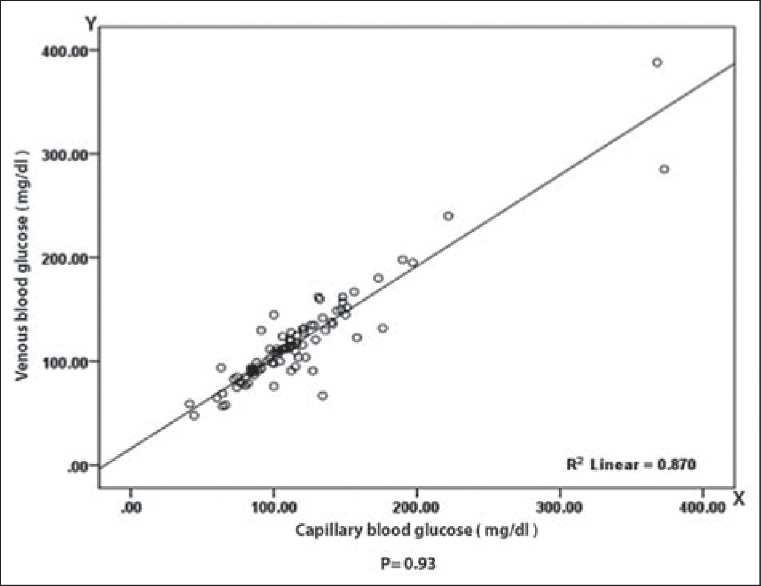
Correlation between capillary blood glucose and venous blood glucose (mg/dl) (P = 0.93)
Figure 3.
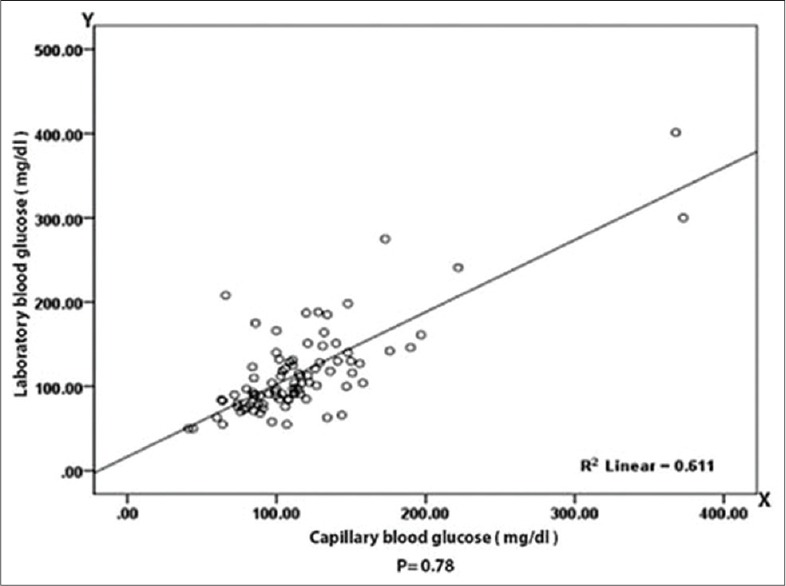
Correlation between capillary blood glucose and laboratory blood glucose (mg/dl) (P = 0.78)
Figure 4.
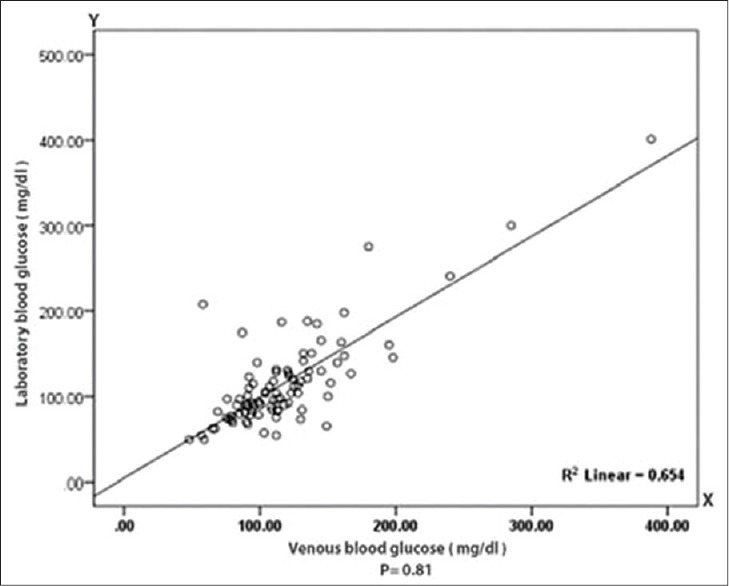
Correlation between venous blood glucose and laboratory blood glucose (mg/dl) (P = 0.81)
Table 2.
Mean and standard deviation and range of blood glucose with the three methods
DISCUSSION AND CONCLUSION
The overall objective of conducting the present study was to compare CBG level with intravenous blood glucose level measured by glucometer and in the laboratory. According to the results obtained from the study, the mean of CBG level and venous blood glucose level measured by glucometer had no significant difference in both methods. The correlation rate between the blood glucose levels was 93%, whereas between the levels of CBG and LBG, the observed correlation rate was less and was equivalent to 78%. Also, the correlation between the levels of venous blood glucose measured by glucometer and in the laboratory was 0.81. Thus, if laboratory measured venous blood glucose was considered as the basis, the level of venous blood glucose measured by glucometer would be closer to the level of measured blood glucose in the laboratory. On the other hand, in case of poisoned patients being in coma, one of the crucial steps is measurement of blood glucose level. Glucometer is considered as the most accessible tool for measuring blood glucose. So, considering the lack of a significant difference between the blood glucose measured by glucometer and in the laboratory, this tool can be used to determine the blood glucose level of poisoned patients being in coma.
In a study on 97 healthy volunteers, Funk et al. simultaneously took capillary and venous blood samples from individuals and the blood glucose level of the two samples was measured by a glucometer. A weak correlation was obtained between the levels of venous and capillary blood glucose.[4] But in Matthews et al.'s study, in which capillary and venous blood glucose of 182 diabetic patients was measured by a glucometer, it was observed that when the level of venous blood glucose was divided by 1.1, CBG was obtained.[5] In Boyd et al.'s study, samples of venous and capillary blood were taken from 20 patients bedridden in the emergency room and the glucose levels in both samples were checked by a glucometer and in the laboratory. Small but significant difference was obtained on comparing the venous blood glucose checked by glucometer and in the laboratory with the CBG checked by glucometer.[6] In a study conducted by Kuwa et al., samples of capillary, venous, and plasma blood were compared; the blood glucose levels in the three mentioned methods showed no significant difference.[12] In a study conducted by Kruijshoop et al., using capillary glucose level has been recommended as the screening test to diagnose diabetes II.[8] In another study conducted by Dubose, the correlation between the levels of capillary and venous blood glucose was found in patients with and without shock, in which a slight difference was observed between both groups.[13] While in the study of Fekih Hassen, samples because of the difference of capillary and venous blood glucose levels in patients with serious conditions, using capillary samples has not been recommended to determine the level of blood glucose level.[2] The difference between our study and other studies is that in the present study, the blood glucose level of poisoned patients was determined by the three above-mentioned methods, while the other studies were conducted with different goals. For example, in the study of Funk et al., only healthy patients were studied. Stress due to poisoning and taking overdose might have caused hyperglycemia or hypoglycemia in the present study. Accuracy in the determination of blood glucose level is very important. In Matthews et al.'s study, only the diabetics were examined, and in Boyd et al.'s study, emergency patients including internal neurology and poisoned persons were studied. Also, in the study of Kuwa et al., the aim of research was doing a epidemiological study. Therefore, the source of difference between the results of the mentioned studies may be the sample population. Thus, given the results obtained in this study, whereas the level of blood glucose determined by glucometer is close to the level of laboratory blood glucose, on the other hand, it involves risks such as infection, hematoma, nerve damage, bleeding, and bruising induced by capillary sampling. Also, there are relative and absolute contraindications to take capillary blood samples from patients of poisoning who are in coma, such as environmental vasoconstriction, cold extremities, hypotension, infection, inflammation, and local edema of tissues.[4] In conclusion using venous blood sample and measuring it by glucometer strip is an acceptable and advisable method and CBG measurement by using glucose meter is not recommended for patients in coma.
Limitations of this study were death of patients or lack of patients’ cooperation that decreased the number of samples. The other limitations are applying insufficient blood to the strip and using strips that are exposed to excess moisture or humidity that could decrease the accuracy.
ACKNOWLEDGMENT
This work was supported by Isfahan University of Medical Sciences, Isfahan, Iran.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Juneja D, Pandey R, Singh O. Comparison between arterial and capillary blood glucose monitoring in patients with shock. Eur J Intern Med. 2011;22:241–4. doi: 10.1016/j.ejim.2011.01.004. [DOI] [PubMed] [Google Scholar]
- 2.Fekih Hassen M, Ayed S, Gharbi R, Ben Sik Ali H, S. Marghli S, Elatrous S. Bedside capillary blood glucose measurements in critically ill patients: Influence of catecholamine therapy. Diabetes Res Cline Pract. 2010;87:87–91. doi: 10.1016/j.diabres.2009.09.018. [DOI] [PubMed] [Google Scholar]
- 3.Desachy A, Vuagnat AC, Ghazali AD, Baudin OT, Longuet OH, Calvat SN, et al. Accuracy of bedside glucometry in critically ill patients: Influence of clinical characteristics and perfusion index. Mayo Clin Proc. 2008;83:400–5. doi: 10.4065/83.4.400. [DOI] [PubMed] [Google Scholar]
- 4.Funk DL, Chan L, Lutz N, Verdile VP. Comparison of capillary and venous Glucose measurements in healthy volunteers. Prehosp Emerg Care. 2001;5:275–7. doi: 10.1080/10903120190939788. [DOI] [PubMed] [Google Scholar]
- 5.Matthews DR, Burton SF, Bown E, Chusney G, Dornan T, Gale A, et al. Capillary and Venous blood Glucose measurements using a direct glucose sensing meter. Diabet Med. 1991;8:875–80. doi: 10.1111/j.1464-5491.1991.tb02128.x. [DOI] [PubMed] [Google Scholar]
- 6.Boyd R, Leigh B, Stuart P. Capillary versus venous bedside blood glucose estimation. Emerg Med. 2005;22:177–9. doi: 10.1136/emj.2003.011619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sabzghabaee AM, Eizadi-Mood N, Gheshlaghi F, Adib N, Safaeian L. Is there a relationship between admission blood glucose level following acute poisoning and clinical outcome.? Arch Med Sci. 2011;7:81–6. doi: 10.5114/aoms.2011.20608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kruijshoop M, Feskens EJ, Blaak EE, de Bruin TW. Validation of capillary glucose measurements to detect glucose intolerance or type 2 diabetes mellitus in the general population. Clin Chim Acta. 2004;341:33–40. doi: 10.1016/j.cccn.2003.10.033. [DOI] [PubMed] [Google Scholar]
- 9.Persson HE, Sjoberg GK, Haines JA, Pronczuk de Garbino J. Poisoning severity score. Grading of acute poisoning. J Toxicol Clin Toxicol. 1998;36:205–13. doi: 10.3109/15563659809028940. [DOI] [PubMed] [Google Scholar]
- 10.Casey PB, Dexter EM, Michell J, Vale JA. The prospective value of the IPCS/EC/EAPCCT poisoning severity score in cases of poisoning. J Toxicol Clin Toxicol. 1998;36:215–7. doi: 10.3109/15563659809028941. [DOI] [PubMed] [Google Scholar]
- 11.Ousman Y. Hyperglycemia in the hospitalized patient. Clin Diabetes. 2002;20:147–8. [Google Scholar]
- 12.Kuwa K, Nakayama T, Hoshino T, Tominaga M. Relationships of glucose concentrations in capillary whole blood, venous whole blood and venous plasma. Clin Chim Acta. 2001;307:187–92. doi: 10.1016/s0009-8981(01)00426-0. [DOI] [PubMed] [Google Scholar]
- 13.Du Bose JJ, Inaba K, Branco BC, Barmparas G, Lam L, Teixeira PG, et al. Discrepancies between capillary glucose measurements and traditional laboratory assessments in both shock and non-shock states after trauma. J Surg Res. 2012;178:820–6. doi: 10.1016/j.jss.2012.04.003. [DOI] [PubMed] [Google Scholar]