

Abstract
Thoracic aortic mycotic aneurysms caused by Aspergillus fumigatus postoperatively are rare and devastating complications. These cases are usually attributed to intraoperative contamination of surgical equipment. We present a patient who had an ascending aortic mycotic aneurysm 20 weeks post aortic valve replacement. A high index of suspicion allowed for diagnosis and prompt treatment, although the patient presented in an unusual manner. Treatment included both medical and surgical therapy to minimize morbidity and mortality. Despite treatment our patient suffered long-lasting consequences due to the aggressive nature of the disease. Cases presented in the literature and this experience show that a high index of suspicion must be maintained in such patients regardless of immune status and postoperative interval, in order to avoid long-lasting sequelae.
Keywords: Thoracic aortic aneurysm, Pseudoaneurysm, Aortic valve replacement, Aortic aneurysm, False lumen
Introduction
Although rare, mycotic aneurysms have high rates of morbidity and mortality. The true incidence is not known, but it has been estimated to be between 0.65% and 1.3% of all aortic aneurysms [1]. Furthermore, the incidence of thoracic aortic aneurysm is estimated to be 5.9 cases per 100,000 people/year [2], making thoracic aortic mycotic aneurysms (TAMAs) even rarer. Mycotic aneurysms were first described by Osler secondary to endocarditis, and the term “mycotic” referred to any type of infection and not just fungal etiology [1,2]. Fungal organisms like Aspergillus species responsible for formation of mycotic aneurysms are rare; more common organisms implicated are Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus, and Salmonella. The incidence of mycotic aneurysms caused by fungi is difficult to ascertain, since there are few reports. The Centers for Disease Control and Prevention estimates the incidence of aspergillosis to be 1 to 2 cases per 100,000 people/year [3].
Mycotic aneurysms may present with a constellation of nonspecific symptoms and signs, most commonly fever, night sweats, leukocytosis, elevated inflammatory markers, sepsis, anterior chest discomfort, dysphagia, cough, wheezing, stridor, and pneumonitis [3–7]. A high index of suspicion is required to ascertain the diagnosis and implement treatment promptly. Mycotic aneurysms have high rates of rupture and are generally associated with poor outcomes despite medical and surgical intervention [1,2,4–7]. However, better antimicrobial therapies and imaging modalities are helping to ascertain the diagnosis earlier. Past studies have shown that 80% of mycotic aneurysms are the result of microbial aortitis and 3% are estimated to involve infection of a preexisting aneurysm [4].
Case Presentation
A 79-year-old woman underwent aortic valve replacement (AVR) with a bovine bioprosthesis in April 2012. Past medical history included hypertension, paroxysmal atrial fibrillation, and no immunocompromised status. In August 2012 she presented with sudden bilateral loss of vision without fever, chills, or any signs of infection. The most recent echocardiogram showed no issues with the prosthetic aortic valve. However, echocardiogram on admission showed a large vegetation occupying 80% of the ascending aortic lumen together with a large pseudoaneurysm and disruption of the suture line of the aorta (Fig. 1). The Mitroflow® bioprosthetic valve (Sorin Group, Arvada, CO) was working appropriately. Chest computed tomography (CT) scan showed a large pseudoaneurysm, possibly mycotic (Fig. 2). Considering the friable appearance of this mass in the aorta, performing an angiogram was not found to be safe.
Figure 1.
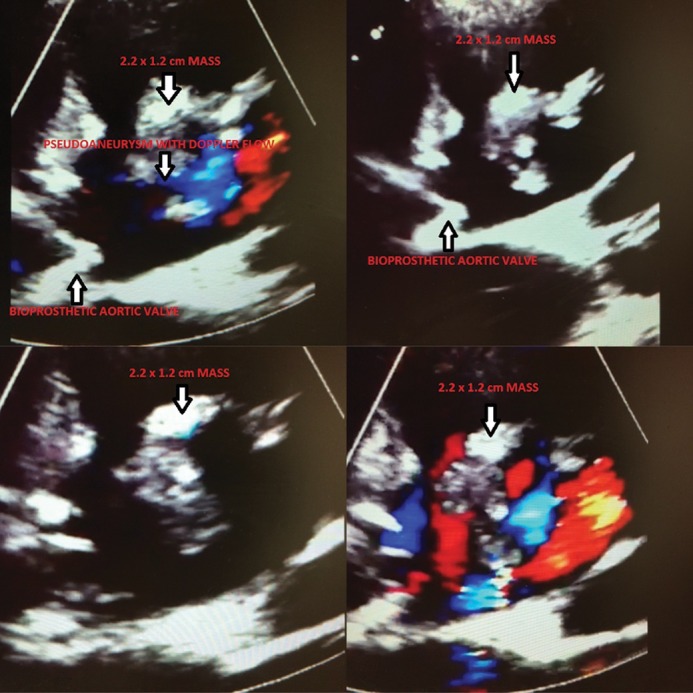
2D Echo. Ascending aortic wall has frank perforation, with evidence of flow into a possible pseudoaneurysm and a large (2.2 × 1.2 cm) mobile echodensity attached to the anterior aspect of the opening into the aneurysm.
Figure 2.
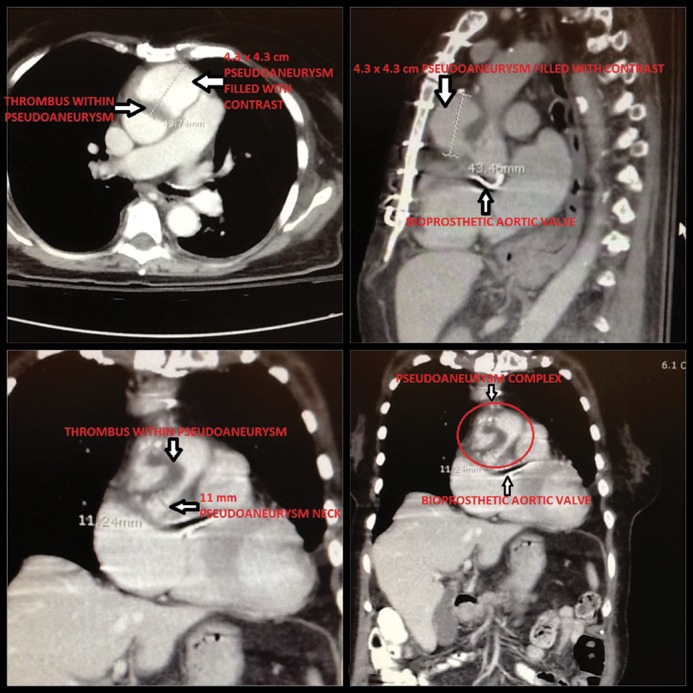
Chest computed tomogram. Ascending aorta with low-attenuation linear thrombus extending into and within a large surrounding complex pseudoaneurysm, part of which remains patent and contrast filled and part of which is thrombosed, measuring approximately 4.3 × 4.3 cm. The neck measures approximately 11 mm.
In the operating room, the patient was heparinized and cannulated through the left femoral artery and left femoral vein, and placed on cardiopulmonary bypass before opening the chest. Distal control was achieved above the aneurysm (where the aorta was normal) after an uneventful redo sternotomy. The pseudoaneurysm was left intact within its pericardial covering. The patient's temperature was decreased to 28°C. The large mycotic aneurysm was opened, revealing a large fungal ball sitting in the lumen of the aorta. Amphotericin wash was given several times. The Mitroflow® bioprosthetic valve appeared normal. The entire area of the pseudoaneurysm and fungus ball was excised and sent for bacteriology analysis. At this time, a 24 mm homograft was used to replace the ascending aorta. The patient recovered appropriately. Postoperative chest CT was obtained (Fig. 3). The patient exhibited mental status changes on postoperative day 5, which prompted brain MRI. Two cerebellar abscesses and a hemorrhagic stroke were noted (Fig. 4), for which the patient declined treatment. Currently, the patient is doing well, living with her husband, although she did not recover her vision. The patient completed a yearlong antifungal therapy of intravenous amphotericin and oral fluconazole. The last brain MRI showed much improvement (Fig. 5).
Figure 3.
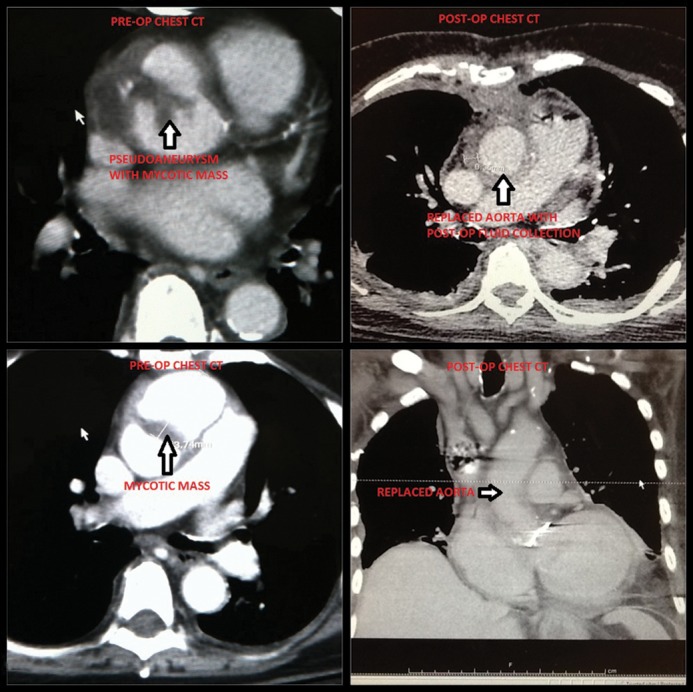
Chest computed tomogram. Interval resection of pseudoaneurysm with replacement of the ascending aorta. Thoracic aorta is normal in caliber without evidence of dissection or aneurysm.
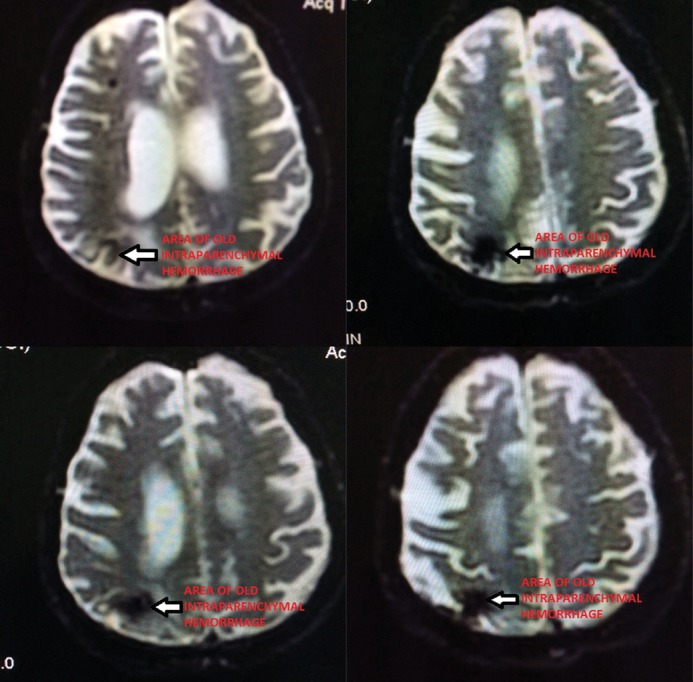
Figure 4.
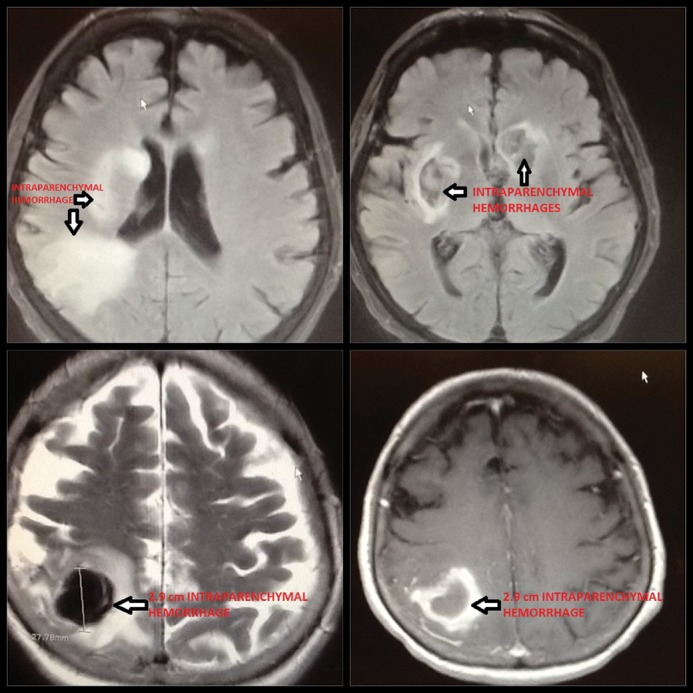
Brain MRI. Intraparenchymal areas of hemorrhage noted with the largest along the right parietal lobe measuring approximately 2.9 cm in anteroposterior dimension. Intraparenchymal areas of hemorrhage along right insular cortex, right basal ganglia, and left head of the caudate.
Figure 5.
Brain MRI. Resolving brain lesion on right parietal lobe.
Discussion
We present a rare case of TAMA with an unusual presentation. In the literature, most cases of TAMA caused by fungus have presented with some type of systemic symptom (i.e., fever, tachycardia, hypotension, leukocytosis, etc.) [1,4–7]. Our patient presented with only a complaint of progressive bilateral vision loss. At the time of surgery, the aortic valve prosthesis was intact and free of infection. In our case, the suspected site of infection was the suture line above the valve, possibly a pledgeted suture contaminated in the operating room at the time of aortic valve replacement 20 weeks prior. As alluded to in other case reports, the possible origin of the infective agent in our patient is suspected to be airborne spores arising from the operating room ventilation system. The literature reports an average of 10 months between surgery and diagnosis [5–7]. A high index of suspicion and prompt surgical and medical therapy must be implemented immediately to avoid long-term morbidity and mortality. Traditionally, treatment has included surgical debridement, including graft excision, and aggressive antifungal therapy; however, mortality remains high, attributed to both the highly aggressive nature of the infection and delay in diagnosis. It is important to note that despite intervention, the patient sustained embolic and hemorrhagic strokes preoperatively, and she did not recover her sight; however, she continues to be well otherwise.
In summary, thoracic aortic mycotic aneurysms caused by Aspergillus are a rare but serious entity with high rates of morbidity and mortality, which requires prompt recognition and implementation of medical and surgical therapy.
Conflict of Interest
The authors have no conflict of interest relevant to this publication.
References
- 1. Chan YC, Morales JP, Taylor PR. The management of mycotic aortic aneurysms: is there a role for endoluminal treatment? Acta Chir Belg. 2005;105:580–587. [DOI] [PubMed] [Google Scholar]
- 2. Brunicardi F, Anderson D. Thoracic aneurysms and aortic dissection. In: Schwartz's Principles of Surgery, 9th Edition, Print New York: McGraw-Hill, Health Professions Division; 2010, p. 668–669. [Google Scholar]
- 3. Cdc.gov. 2013. CDC - Aspergillosis Statistics - Aspergillosis. [online] Available at: http://www.cdc.gov/fungal/aspergillosis/statistics.html and http://www.cdc.gov/fungal/aspergillosis/symptoms/clinical-features.html [Accessed: 24 Oct 2013].
- 4. Laohapensang K, Rutherford RB, Arworn S. Infected aneurysm. Ann Vasc Dis. 2010;3:16–23. 10.3400/avd.ctiia09002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Afsari K, Stallone R, Wong GD. Mycotic (infected) aneurysm caused by Streptococcus pneumoniae. Infect Med. 2001;18(6). [Google Scholar]
- 6. Collazos J, Mayo J, Martínez E, Ibarra S. Prosthetic vascular graft infection due to Aspergillus species: case report and literature review. Eur J Clin Microbiol Infect Dis. 2001;20:414–417. 10.1007/s100960100521 [DOI] [PubMed] [Google Scholar]
- 7. Oyama J, Zhou L, Mehta S, Laury A, Tsakonas J, Laks H, et al. Aspergillus fumigatus vegetation of a prosthetic aortic root graft with mycotic aneurysm and subarachnoid hemorrhage. Int J Infect Dis. 2013: 17:e773–e776. 10.1016/j.ijid.2012.11.028 [DOI] [PubMed] [Google Scholar]