

Sir,
A 29-year-old woman presented with a gradually growing, painless, infraumbilical mass in the anterior abdominal wall. Abdominal ultrasonography showed a subcutaneous swelling with heterogeneous echotexture located above the rectus sheath. The swelling was 5 cm × 4 cm × 4 cm at presentation. There was no associated lymphadenopathy or fever. Fine-needle aspiration cytology (FNAC) of the mass showed numerous large histiocytes with voluminous eosinophilic cytoplasm containing intact lymphocytes, plasma cells, and neutrophils (emperipolesis) [Figure 1]. Some of these histiocytes were binucleate or multinucleated. The nuclei were bland with fine, evenly distributed chromatin. We made a diagnosis of extranodal Rosai-Dorfman disease. An excision biopsy was subsequently performed. Grossly, the mass was solid gray-white and measured 5 cm × 4 cm × 2.5 cm. Microscopic examination showed numerous histiocytes exhibiting emperipolesis along with dense inflammation and stromal fibrosis [Figure 2], confirming our cytology diagnosis. The histiocytes expressed S100 protein [Figure 3].
Figure 1.
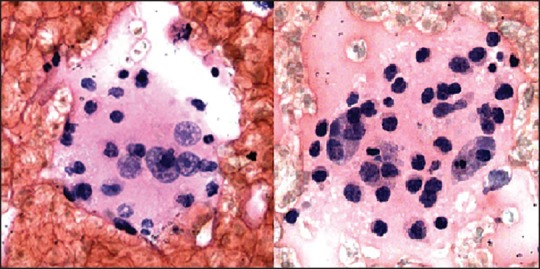
FNAC, histiocyte exhibiting emperipolesis (H and E, ×400)
Figure 2.
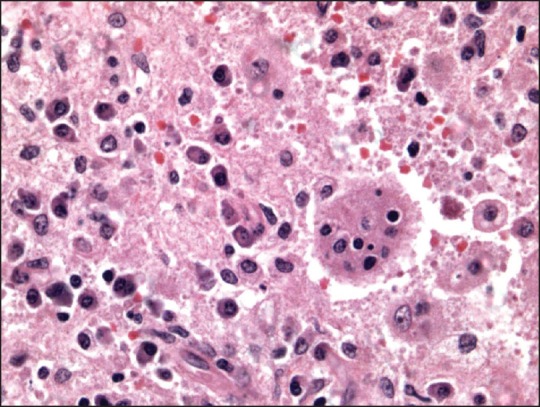
Histology, emperipolesis (H and E, ×200)
Figure 3.
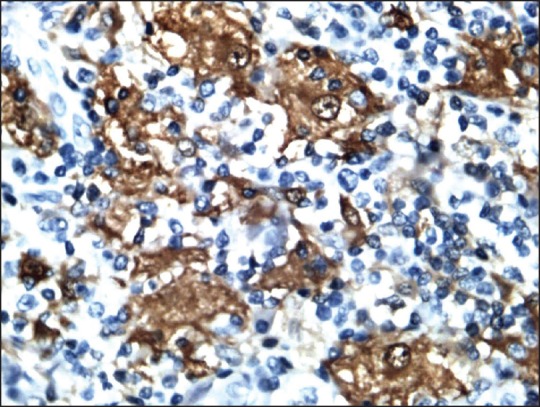
Immunohistochemistry, S100 positivity of histiocytes (Diaminobenzidine [DAB], ×200)
Rosai-Dorfman disease (sinus histiocytosis with massive lymphadenopathy) was described by Rosai and Dorfman in 1969.[1] However, earlier in 1947, Robb-Smith had documented it as giant cell reticulosis in children. It is an idiopathic, nonneoplastic proliferative disorder of histiocytes with concomitant extranodal involvement in approximately one-third of cases. Nodal Rosai-Dorfman disease commonly presents as painless massive bilateral cervical lymphadenopathy, frequently associated with fever, leukocytosis, elevated erythrocyte sedimentation rate (ESR), and hypergammaglobulinemia. Isolated extranodal manifestation is relatively rare, often lacks constitutional symptoms, and has been reported in the orbit, paranasal sinuses, skin, meninges, thyroid, bone, and salivary glands.[2] The disease has not been documented in the abdominal wall so far.
The disease is commonly observed in the first and second decades of life, with a slight male predilection. Isolated extranodal forms tend to occur at an older age.
The etiology of the disease remains unknown. It is attributed to either immunological dysfunction or infectious agents that result in macrophage proliferation stimulated by growth factors. The disease may be self-limiting or may require surgical intervention based on size and symptoms.
Both nodal and extranodal Rosai-Dorfman disease exhibit similar morphology on FNAC.[3,4]
The microscopic hallmark of the disease on FNAC as well as on histology is the presence of the following: Numerous large histiocytes having one or more nuclei; fine, evenly spread chromatin; and abundant eosinophilic cytoplasm that exhibits emperipolesis, that is, there are engulfed intact lymphocytes, neutrophils, and/or plasma cells within their cytoplasm. Immunohistochemistry with S100 shows cytoplasmic positivity in the histiocytes. The histiocytes also show positivity with CD11c, CD14, CD68, and CD33.[5]
The conditions that may be considered with such morphology on FNAC are reactive sinus histiocytosis, Langerhans cell histiocytosis, hemophagocytic syndrome, and lymphomas. However, emperipolesis is not seen in any of the conditions mentioned above. Further, there are nuclei with grooves in Langerhans cell histiocytosis, a feature not seen in Rosai-Dorfman disease. Lymphomas show a diffuse, monotonous lymphoid population, often with increased mitoses — another feature not seen in Rosai-Dorfman disease.
Though extranodal Rosai-Dorfman disease is an uncommon entity, cytopathologists must keep this entity in mind as a possible diagnosis in abdominal wall soft-tissue masses.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy: A newly recognised benign clinicopathological entity. Arch Pathol. 1969;87:63–70. [PubMed] [Google Scholar]
- 2.Deshpande AH, Nayak S, Munshi MM. Cytology of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease) Diagn Cytopathol. 2000;22:181–5. doi: 10.1002/(sici)1097-0339(20000301)22:3<181::aid-dc10>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]
- 3.Foucar E, Rosai J, Dorfman R. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): Review of the entity. Sem Diag Pathol. 1990;7:19–73. [PubMed] [Google Scholar]
- 4.Kumar B, Karki S, Paudyal P. Diagnosis of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease) by fine needle aspiration cytology. Diagn Cytopathol. 2008;36:691–5. doi: 10.1002/dc.20904. [DOI] [PubMed] [Google Scholar]
- 5.Kushwaha R, Ahluwalia C, Sipayya V. Diagnosis of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease) by fine needle aspiration cytology. J Cytol. 2009;26:83–5. doi: 10.4103/0970-9371.55229. [DOI] [PMC free article] [PubMed] [Google Scholar]