

Abstract
Introduction:
The World Health Organization's 2004 Global Burden of Disease report indicated 3.6 million years of productive, healthy life is lost worldwide as a result of primary insomnia. Approximately 30–35% of people meet diagnostic criteria for primary insomnia characterized by impairment resulting from problems of falling and staying asleep.
Aims:
To evaluate the effect of Tagara (Valeriana wallichii DC.) and Jatamansi (Nardostachys jatamansi DC.) in the management of Anidra.
Materials and Methods:
A total of 34 patients were selected fulfilling the criteria for inclusion for primary insomnia were randomly selected from Out Patient Department and In Patient Department of Manasa Roga and assigned into two groups, wherein 30 patients completed the study (15 in each). Tagara Churna (powder of V. wallichii) and Jatamansi Churna (powder of N. jatamansi) in the dose of 4 gm with milk was administered three times a day for a period of 1 month.
Results:
Tagara provided significant improvement in initiation of sleep (76.00%; P < 0.001), duration of sleep (55.17%; P < 0.001), disturbed sleep (69.58%; P < 0.001), and disturbances in routine work (73.95%; P < 0.001). Jatamansi provided improvement in initiation of sleep (61.34%; P < 0.001), duration of sleep (48.25%; P < 0.001), disturbed sleep (53.08%; P < 0.001), and disturbance in routine works (43.85%; P < 0.001).
Conclusion:
Both the groups showed good results, but Tagara group showed better results in comparison to Jatamansi group.
Keywords: Anidra, Jatamansi Churna, Nardostachys jatamansi, primary insomnia, Tagara Churna, Valeriana wallichii
Introduction
Aahara (food), Nidra (sleep), and Brahmacharya (abstinence) are described to be the Trayopasthambhas (three supportive pillars) of life[1] and so, sleep is one of the essential factors to lead a healthy life. It has been rightly stated by Acharya Charaka that happiness and misery, proper and improper growth, good strength and weakness, potency and sterility, knowledge and ignorance, and life and death of an individual depend on the quality of sleep.[2]
Human being spend at least one-third of their life in asleep.[3] The importance of sleep is well accepted by modern science also because of its restorative, recuperative, and resting actions. Insomnia is a sleep disorder in which there is an inability to fall asleep or to stay asleep as long as desired. Among the chronic insomniac patients, about 25% are suffering from primary insomnia.[4]
In comparison to the therapeutic procedure of different systems of medicine, Ayurveda has a very good approach towards the treatment of Anidra (insomnia). a good number of single drugs too are described in Ayurvedic literatures which give relief from Anidra. Tagara and Jatamansi are included among the Nidrajanana (sedative and hypnotic) drugs in the classics.
By taking into consideration of the above facts, this comparative study was planned to evaluate the effect of Tagara (Valeriana wallichii DC.) and Jatamansi (Nardostachys jatamansi DC.) clinically in the management of Anidra (primary insomnia) and to compare the effect of both drugs in the management of Anidra.
Materials and Methods
A total of 34 patients fulfilling the diagnostic criteria of Anidra (primary insomnia) were randomly selected and registered from the Out Patient Department and In Patient Department of Manasa Roga. The study was carried out after obtaining the ethical clearance of Institutional Ethics Committee (SDM/IEC/35/2010- 2011 dated 14-03-2011), and prior consent was taken from the patient for undertaking the study.
For diagnosis, a detailed medical history was taken and physical examination was done in detail according to both modern and Ayurvedic clinical methods. A detailed interview was conducted to elucidate sleep problems, social problems, and other areas of functioning, etc.
To assess the psychological intactness, the mental status examination was carried out. To confirm or exclude the other medical disorders, routine hematological and urine investigations were carried out. A special proforma was prepared with a gradation of symptoms and scoring was done by adopting Athens Insomnia Scale.[5]
Inclusion criteria
Patients of insomnia suffering up to 5 years duration
Patients of either sex, between the age group 15 and 45 years
Anidra (insomnia) patients complaining of Angamarda (bodyache), Shirogaurava (heaviness in the head), Jrumbha (yawning), Jadyata (inactivity), Glani (exhaustion), Bhrama (giddiness), Apakti (indigestion).
Exclusion criteria
Anidra (insomnia) due to other conditions such as Madatyaya (alcoholism), Abhighata (injury), and other systemic diseases
Patients with secondary insomnia
Patients on hypnotic medicine or other drugs known to cause drowsiness.
Grouping and posology
The patients were divided into two groups
Tagara group
In this group, 16 patients were registered, and the study was completed with 15 patients. Tagara Churna (powder of V. wallichii rhizome) in the dose of 4 gm with milk was administered 3 times a day after food for a period of 1 month.
Jatamansi group
In this group, 18 patients were registered, and the study was completed with 15 patients. Jatamansi Churna (powder of N. jatamansi rhizome) in the dose of 4 gm with milk was administered 3 times a day after food for a period of 1 month.
After the completion of treatment, patients were asked to follow up study at the fortnightly interval for 1 month. Both test drugs were procured from the pharmacy attached to Sri Dharmasthala Manjunatheshwara College of Ayurveda and Hospital, Hassan.
Criteria for assessment
The cardinal signs and symptoms such as difficulty in the initiation of sleep, sleep duration, disturbed sleep, and routine disturbances before and after treatment was measured by adopting Athens Insomnia Scale.[5] Associated symptoms such as Angamarda (malaise), Shirogaurava (heaviness in head), Shirashoola (headache), Jrumbha (yawning), Glani (exhaustion), Bhrama (giddiness), Shrama (fatigue), and Klama (mental fatigue) were assessed by adopting scoring system according to severity of each symptom.
Statistical analysis
Statistical analysis was carried by using student's t- test for comparison.
Observations
A total of 34 patients of Anidra were studied in two groups; of which 30 patients completed the course of treatment (15 in each). The chronicity was reported up to 6 months to 1 year by 35.29%, 1–2 years by 29.41%, 3–6 months by 26.47%, and 2–5 years of duration was found in 8.82% of patients. Of 34 patients, specific causative factors of Anidra that is chinta (excessive thinking) which was observed in 85.29%. Other etiological factors noted in the patients of this series were Udvega (anxiety) in 64.71%, Vishada (depression) in 29.41%, and family problems in 38.23%. Cardinal symptoms such as reduction in sleep time was present in all the patients that is, 100%, difficulty in initiation of sleep in 73.52%, disturbed sleep in 52.94%, disturbed routine work in 47.05%. Associated symptoms such as Shirogaurava was present in 64.70%, Angamarda in 61.76%, Shrama in 47.05%, Klama and Shirashula in 44.11% each, Glani in 41.17%, Aruchi (distaste) in 38.23%, Apakti (indigestion) and Jrumbha in 35.29% each, Jadyata (inactivity) and Tandra (stupor) in 29.41% each, and Bhrama in 23.52% of patients.
Results
The effectiveness is considered positive on the basis of established insomnia scoring scale before treatment and after the completion of 1 month of treatment.
Tagara group provided a significant improvement in duration of sleep by 55.17%, in the initiation of sleep by 76.00%, in disturbed sleep by 69.58%, in disturbances in routine work by 73.95%. This difference was statistically highly significant (P < 0.001) [Table 1]. Jatamansi group provided 61.34% improvement in the initiation of sleep, 48.25% in the duration of sleep, 43.85% in a disturbance in routine works, and 53.08% in disturbed sleep. This improvement was statistically highly significant (P < 0.001) [Table 2].
Table 1.
Effect of Tagara on sleep pattern of 15 patients of Anidra (insomnia)

Table 2.
Effect of Jatamansi on sleep pattern of 15 patients of Anidra (insomnia)

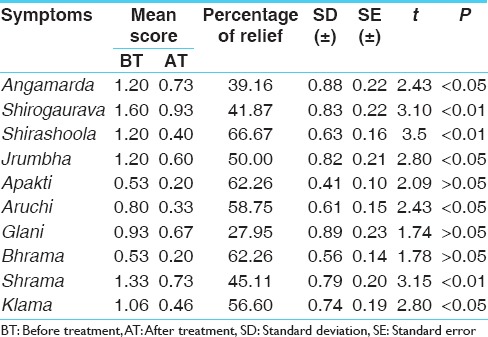
Tagara provided significant relief in Angamarda (78.33%), Shirogaurava (72.60%), Shirashoola (55.83%), Jrumbha (26.41%), Glani (36.79%), Bhrama (86.02%), Shrama (80.45%), and Klama (83.33%) [Table 3]. Jatamansi also gave significant relief in Angamarda (39.16%), Shirogaurava (41.87%), Shirashoola (66.67%), Jrumbha (50.00%), Aruchi (58.75%), Shrama (45.11%), Klama (56.00%), etc. [Table 4].
Table 3.
Effect of Tagara on associated symptoms of 15 patients of Anidra (insomnia)
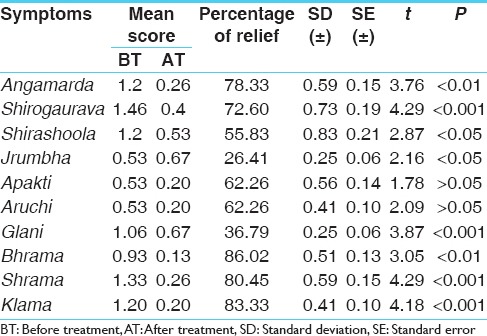
Table 4.
Effect of Jatamansi on associated symptoms of 15 patients of Anidra (insomnia)
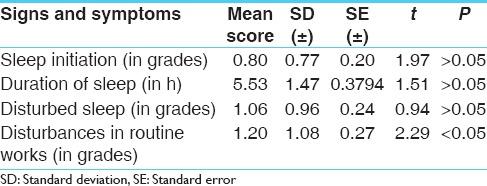
While comparing the effect in between two groups of Tagara and Jatamansi, a statistical significance was present only in the symptom of disturbances in routine works whereas in the symptoms such as sleep initiation, duration of sleep, and disturbed sleep was insignificant [Table 5].
Table 5.
Comparative effect of Tagara and Jatamansi in Anidra
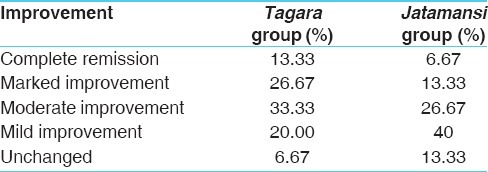
The consideration of the overall effect of Tagara showed that, in this group, 13.3% had complete remission, 26.67% patient had marked improvement, 33.33% patients had moderate improvement, and 20.00% had mild improvement. Remaining 6.67% of patients remained unchanged. While in Jatamansi group, complete remission was found in 6.67% of patients, marked improvement in 13.33%, moderate improvement in 26.67%, and mild improvement in 40.00%; remaining 13.33% of patients remain unchanged [Table 6].
Table 6.
Overall effect of therapy
Discussion
Tamas (psychic principle) and Kapha Dosha (bodily humor) are responsible for sleep, whereas Rajas (psychic principle) and Vata Dosha (bodily humor) are responsible for loss of sleep or insomnia. Tagara and Jatamansi have similar Rasa (taste), Guna (property), and Vipaka (end product of digestion) while they differ only in Virya (potency). It is mentioned that there cannot be any Karma (action) without the help of Virya (potency).[6] The Rasa (taste) of Tagara is being Katu (pungent), Tikta (bitter), Kashaya (astringent), they should probably aggravate Vata (bodily humor). However because of its Ushna Virya (hot potency), it alleviates rather than aggravate Vata. This might be the probable reason that Tagara showed a better action when compared to Jatamansi. These pharmacodynamic actions are helpful in breaking the pathogenesis of Anidra.
Valerian and Nardostachys belong to the Valerianaceae family and share a group of active constituents, and the herbs are each characterized by an unusual fragrance, derived from the essential oil components. While looking into the mechanism of action of the drugs, both Tagara and Jatamansi have similar actions.[7,8] Valeranone and Valepotriates are present in both the drugs, where in the percentage of the active chemical constituents are more in the case of V. wallichii. Valeranone present in Tagara is 2%[7] whereas in Jatamansi it is only 0.02–0.1%.[9] Furthermore, Valepotriates are present in 3–6% in Tagara[10] whereas in Jatamansi it is less than 0.07%.[11] Valepotriates are responsible for the chief effect of Valerian as a potent Sedative.[12] It inhibits enzyme-induced breakdown of GABA in the brain resulting in sedation.[7,8] This might be the probable reason that there was a significant improvement in the signs and symptoms of the patients.
Conclusion
It is obvious from the foregoing study that Tagara and Jatamansi provided significant relief in signs and symptoms of the patients of Anidra. While comparing the results of both drugs it can be stated that Tagara provided better relief in the patients of Anidra in comparison to Jatamansi. Thus, it can be concluded that Tagara which is having the property of Nidrajanana (sedative and hypnotic) was found to be more effective in Anidra when compared to Jatamansi.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Trikamji J, editor. 2nd ed. Varanasi: Chaukhamba Sanskrit Sansthan; 1990. Agnivesha, Charaka, Dridhabala, Charaka samhita, Sutra Sthana, Ch.11, Ver. 35; p. 74. [Google Scholar]
- 2.Trikamji J, editor. Agnivesha, Charaka, Dridhabala, Charaka Samhita, Sutra Sthana, Ch.21, Ver. 36. 2nd ed. Varanasi: Chaukhamba Sanskrit Sansthan; 1990. p. 118. [Google Scholar]
- 3.Namboodiri VM. Sleep and Sleep Disorders. Concise Textbook of Psychiatry. 2nd ed. New Delhi: Elsevier; 2005. p. 271. [Google Scholar]
- 4.Roth T. Insomnia: Epidemiology, characteristics, and consequences Clin Cornerstone. 2003;5:5–15. doi: 10.1016/s1098-3597(03)90031-7. [DOI] [PubMed] [Google Scholar]
- 5.Soldatos CR, Dikeos DG, Paparrigopoulos TJ. The diagnostic validity of the Athens Insomnia Scale. J Psychosom Res. 2003;55:263–7. doi: 10.1016/s0022-3999(02)00604-9. [DOI] [PubMed] [Google Scholar]
- 6.Trikamji J, editor. 2nd ed. Varanasi: Chaukhamba Sanskrit Sansthan; 1990. Agnivesha, Charaka, Dridhabala, Charaka Samhita. Sutra Sthana, Ch. 26, Ver. 65; p. 147. [Google Scholar]
- 7.Houghton PJ. The scientific basis for the reputed activity of Valerian. J Pharm Pharmacol. 1999;51:505–12. doi: 10.1211/0022357991772772. [DOI] [PubMed] [Google Scholar]
- 8.Prabhu V, Karanth KS, Rao A. Effects of Nardostachys jatamansi on biogenic amines and inhibitory amino acids in the rat brain. Planta Med. 1994;60:114–7. doi: 10.1055/s-2006-959429. [DOI] [PubMed] [Google Scholar]
- 9.Gupta RK, Disket J, Mann S. A review on spikenard (Nardostachys jatamansi DC.) – An endangered essential herb of India. Int J Pharm Chem. 2012;2:52–60. [Google Scholar]
- 10.Bos R, Woerdenbag HJ, De Smet PAGM, Keller K, Haensel R, Chandler RD, et al. Adverse Effects of Herbal Drugs. Vol. 3. Berlin: Springer-Verlag; 1998. Valeriana species; pp. 165–80. [Google Scholar]
- 11.Dugaheh MA, Meisami F, Torabian Z, Sharififar F. Antioxidant effect and study of bioactive components of Valeriana sisymbriifolia and Nardostachys jatamansi in comparison to Valeriana officinalis. Pak J Pharm Sci. 2013;26(1):53–8. [PubMed] [Google Scholar]
- 12.Lindahl O, Lindwall L. Double blind study of a valerian preparation. Pharmacol Biochem Behav. 1989;32:1065–6. doi: 10.1016/0091-3057(89)90082-8. [DOI] [PubMed] [Google Scholar]