

Abstract
Introduction: Irritation fibroma is the most common tumor like and sub mucosal reactive lesion in the oral cavity. Usually it is measured less than 1.5 cm in diameter; however in rare case it has more than 3 cm in diameter. Different kind of treatment for soft tissue lesions include scalpel excision, electrical surgery, and laser surgery. The diode laser can be more effective than conventional surgery, electrosurgery and cryosurgery in reduction of bleeding and pain.
Case Report: We reported a very large irritation fibroma in right lingual side of retromolar pad which was less prone to be traumatized under local irritation, in a woman wearing maxillary complete denture and use of both diode laser and scalpel for its excision.
Keywords: Diode laser, Excision, Fibroma
Introduction
Irritation fibroma is the most common tumor like and submucosal reactive lesion in the oral cavity that composed of fibrous or connective tissue causing by traumatic irritants such as calculi, foreign bodies, chronic biting, overhanging margins restoration, sharp spicules of bones and over extended borders of appliances.1-3 It was first reported in 1846 as fibrous polyp and polypus.2 Irritation fibroma has called some different terms such as traumatic fibroma, peripheral fibroma, fibrous nodule, fibroepithelial polyp, focal fibrous hyperplasia and inflammatory fibrous hyperplasia, and can grow in all organs arising from mesenchymal tissue.2,3
The term “inflammatory fibrous hyperplasia” is used to describe histologically represent fibrous inflammatory and granulation tissue.4 Also it has no malignancy and recurrency if surgical excision and removal of irritation source.5 Generally fibroma presents as a painless, round or ovoid, sessile or pedunculated (in some cases), smooth surface, pinkish in color similar to surrounding mucosa and rubbery to firm in consistency due to its collagen content.2,3 In the black race, it may demonstrate brown to gray pigmentation.3 Fibroma can be seen in any surface of the oral cavity. The most common site is the buccal mucosa along the bite line.2 Usually it is measured less than 1.5 cm in diameter; however in rare case it has more than 3 cm in diameter. Fibroma is usually seen in the forth to sixth decades of life with female predominance.2-4 When treatment is needed, surgical excision with narrow margin is the choice. Recurrence is rare, but it can happen when source of irritation does not eliminate or the excision does not completely do. The prognosis of these lesions is good overally.3,6 Surgical removal of irritation fibroma is one of the most common procedures in the oral and maxillofacial surgery field. Currently the primary area of clinical using laser in dentistry is removal soft tissue lesions.7,8 The laser surgery can be used for incisional and excisional biopsies, gingivectomy, crown lengthening and ablation of the soft tissue lesions.9 The diode laser can be more effective than conventional surgery, electrosurgery and cryosurgery in reduction of bleeding and pain.10 Histopathological features of this lesion consist of fibrous connective tissue covered by stratified squamous epithelium that connective tissue is usually collagenized and dense or even looser in some cases. The arrangement of the collagen bundles is circular, radiating or haphazard fashion.3 Different histological entities of irritation fibroma may be due to connective tissue responding to various intensities of irritation.2
Case Presentation
A 46 years old woman was referred to the Oral Medicine Department of Shahid Beheshti University of Medical Science. Her chief complaint was a large mass in her oral cavity which interfering eating from 2 years ago that became larger gradually. In the past medical history there was hypertension and taking carvedilol 25 mg 2 times daily. Intraoral examination revealed very large bulky mass measuring 3.5*2.5*1 cm, pale pinkish in color, smooth surface with no ulcer and also some telangiectatic vessels, broad base, firm in consistency located in right lingual side of retromolar pad at posterior site of mouth (Figure 1). She was wearing maxillary complete denture from 3 years ago which the posterior border of denture contact tightly with the lesion, and there was some remained roots in right molars mandibular ridge.
Figure 1 .

Intraoral Examination Revealed Very Large Bulky Mass.
Differential diagnosis was neurofibroma, irritation fibroma and soft tissue mesenchymal tumors. Because of its size, location and possible excessive bleeding, we decided to removal lesion under local anesthesia with diode laser (Dr. Smile) at the 810 nm wavelength with an average of power 3 W and a 0.4 mm diameter fiber tip in 5 minutes. The irradiation mode was continuous wave (CW). Safety measures included wearing of protective goggles, using gauze in the operative field and high vacuum suction. Inferior side of the lesion was cutting by blade no: 15, because of patients gag reflex and we had to continue procedure with scalpel. After a good coagulation surgery wound did not suture and let secondary intention. Chlorhexidine mouth wash 12% was prescribed for the patient 2 times daily. The specimen was sent to Oral and Maxillofacial Pathology department in formalin buffer solution 10% (Figure 2).
Figure 2 .
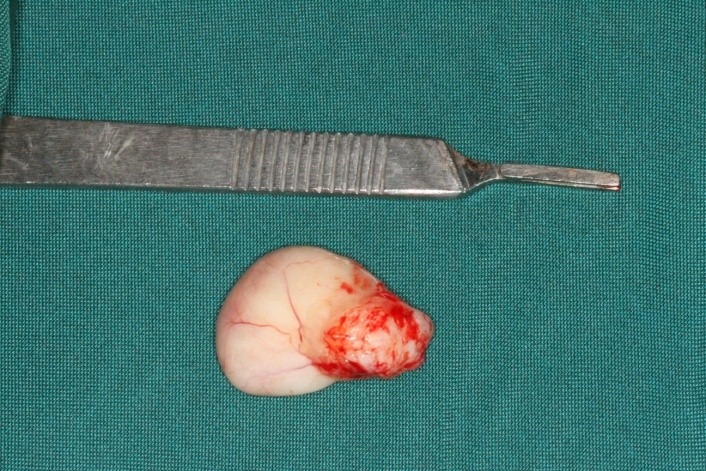
Inferior Aspect of the Specimen.
The sections showed a nodular mass composed of dense collagen bundles with wavy and spindle shaped fibroblasts, arranged in haphazard fashion. The covering stratified squamous epithelium demonstrated atrophy of rete ridge due to connective tissue proliferation. The histopathologic descriptions confirmed a focal fibrous hyperplasia (Figure 3).
Figure 3 .
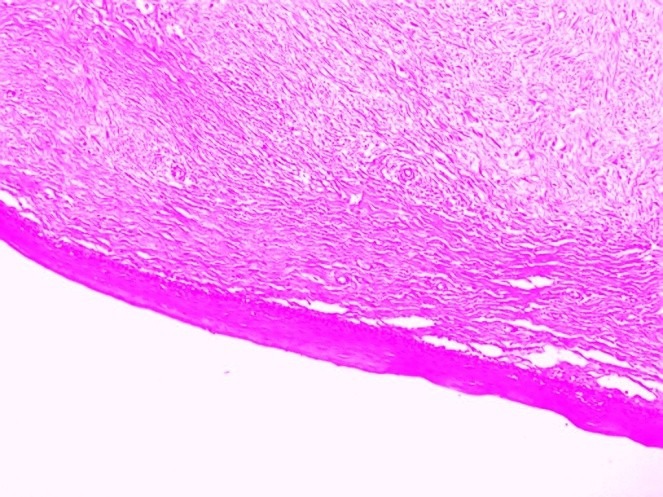
Histopathological feature of the specimen.
The patient was followed after 10 days and we observed a very good healing in that location. Also in second and sixth month there was no evidence of recurrent lesion (Figure 4).
Figure 4 .

The third follow up after 6 months.
Discussion
Most of exophytic lesions in oral cavity are considered to be more reactive than neoplasia.6 Different kind of treatment for soft tissue lesions include: scalpel excision, electrical surgery and laser surgery.7 There are some complications in conventional surgery such as intra and postoperative bleeding, difficulties in wound healing, deep anesthesia, swelling, scarring and postsurgical pain.7,9 Diode lasers have many advantages like; less bleeding, scarring, pain, infection, swelling, reduction in surgical time and a good coagulation.7-9 Diode laser are absorbed by pigmented tissue and hemoglobin.8 And it transmits energy (with wavelengths ranging from 810 to 980 nm in a continuous or pulsed mode) to the cells by warming, coagulating, welding, drying, carbonization, vaporization and protein denaturation.9,11 In numerous studies revealed that laser make sterile conditions because of reduction of bacteremia at the site of operation.7
Laser can be considered as a good modality even for very large lesions which are difficult to access by conventional surgery.
Conflict of Interest
The authors have no conflict of interest to declare.
Please cite this article as follows: Bakhtiari S, Taheri JB, Sehhatpour M, Asnaashari M, Attarbashi Moghadam S. Removal of an extra-large irritation fibroma with a combination of diode laser and scalpel. J Lasers Med Sci. 2015;6(4):182-184. doi:10.15171/jlms.2015.16.
References
- 1. Neville B, Damm DD, Allen CM, Bouqout J. Oral and Maxillofacial Pathology. 3rd ed. United Kingdom: Saunders Elsevier; 2009.
- 2.Singh A, Vengal M, Patil N, Sachdeva SK. Traumatic fibroma- A saga of reaction against irritation. Dental Impact. 2012;4(1):49–52. [Google Scholar]
- 3.Halim DS, Pohchi A, EE Yi P. The prevalence of fibroma in oral mucosa among patient attending USM dental clinic Year 2006- 2010. The Indonesian J Dent Res. 2010;1(1):61–66. [Google Scholar]
- 4.Bagde H, Waghmare A, Savitha B, Vhanmane P. Irritation fibroma - a case report. Int J Dent Clinics. 2013;5(1):39–40. [Google Scholar]
- 5.Hashemi Pour MS, Rad M, Mojtahedi A. A survey of soft tissue tumor- like lesions of the oral cavity: a clinicipathological study. Iran J Pathol. 2008;3(20):81–87. [Google Scholar]
- 6.Harshavardhana B, Rath SK, Mukherjee M. A rare case of irritation fibroma associated with aleukoplakia of oral mucosa. AOSR. 2012;2(1):34–36. [Google Scholar]
- 7.Asnaashari M, Azari Mehrabi S, Alirezaei S, Asnaashari N. Clinical application of 810 nm diode laser to remove gingival hyperplastic lesion. J Lasers Med Sci. 2013;4(2):96–98. [PMC free article] [PubMed] [Google Scholar]
- 8.Ayoub AH, Negm SA. Removal of fibroma using 980 nm diode laser: a case report. Int J Dent Clinics. 2014;6(1):26–27. [Google Scholar]
- 9.Eliades A, Stavrianos C, Kokkas A, Kafas P, Nazaroglou I. 808 diode laser in oral surgey: a case report of laser removal of fibroma. Journal of Medical Science. 2010;4(3):175–178. doi: 10.3923/rjmsci.2010.175.178. [DOI] [Google Scholar]
- 10.Singh G, Yulia Yulia, Chhibber A. laser assisted biopsy of intra- oral irritation fibroma: a cse report. SOLAZE. 2009;3(2):28–30. [Google Scholar]
- 11.Azma E, Safavi N. Diode laser application in soft tissue oral surgery. J Lasers Med Sci. 2013;4(4):206–211. [PMC free article] [PubMed] [Google Scholar]