

Abstract
Objective
The purpose of this case report is to describe the diagnostic value of ultrasonography (US) in a patient with injury to the lateral ligaments of the ankle with concomitant ankle joint osteoarthritis and anterior impingement.
Clinical Features
A 28-year-old male had a history of an inversion injury of the left ankle. Diagnostic US of the left ankle using an 8- to 15-MHz linear array transducer demonstrated a full thickness tear of the anterior talofibular ligament, partial thickness tearing of the calcaneofibular ligament, and laxity of the ankle with varus stress testing. In addition, US was able to demonstrate degeneration of the ankle and talonavicular joints and anterior impingement with dorsiflexion. Osteoarthritic changes were confirmed with radiography. Other US findings included remote deltoid ligamentous complex injury, multiple sites of tenosynovitis, and a large ankle joint effusion with synovial hypertrophy and synovitis.
Intervention and Outcome
Using US, an accurate diagnosis was established with respect to the pathology and functional impairments of the patient’s ankle.
Conclusion
This case report exemplifies the value and utility of US in diagnosing derangement in ligamentous, tendinous, articular, and osseous injuries of the ankle.
Key indexing terms: Ultrasonography, Ankle joint, Diagnosis, Chiropractic
Introduction
Ankle joint injuries are common especially in sports and may result in ligamentous trauma, functional instability, and early degenerative changes.1, 2 Acute ankle injuries typically compromise the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL).3 Recurrent inversion injuries may result in ankle instability subsequent to failure of the lateral stabilizing ligamentous structures. This in turn results in a range of functional deficits and internal derangement. This may include increased likelihood of synovial inflammation, synovitis, cartilage degradation, hyperalgesia and post-traumatic osteoarthritis, varus malalignment and persistent instability.2, 4 In fact, lateral ankle sprains in sporting injuries are the main cause of post-traumatic ankle osteoarthritis.4 Furthermore, a combination of tibiotalar osteophytes and surrounding synovitis may produce anterior ankle impingement, a condition characterized by limitations with dorsiflexion and concurrent pain.5 Inversion ankle injuries should be thoroughly examined so that appropriate diagnosis and treatment can be provided to avoid recurrent injury and obviate ankle joint osteoarthritis. Ultrasonography (US) is useful in evaluating the lateral ankle ligaments as it provides high resolution of ligament anatomy and pathology.6 In addition, as US imaging can be performed dynamically, the integrity of the lateral ankle ligaments can be assessed in real-time under joint stress maneuvers. In cases where joint degeneration has occurred or impingement is suspected clinically, the dynamic nature of US again allows real-time visualization of bony impingement while also permitting correlation to the patient’s symptomatology. Recently, bedside US in an emergency department performed by the emergency physician was demonstrated to have comparable sensitivity (93.8%) and specificity (100%) in detection of ATFL injuries when compared to a magnetic resonance image (MRI) interpreted by a radiologist.7 In patients with suspected chronic lateral ligamentous injury, US again demonstrated high sensitivity, specificity, and accuracy when compared to arthroscopy for detection of ATFL and CFL injury.8 The purpose of this case report is to describe a patient with a chronic injury to the lateral ligaments of the ankle with presumed secondary osteoarthritis and subsequent anterior ankle impingement and the use of US in diagnosing derangement in ligamentous, tendinous, articular, and osseous injuries of the ankle.
Case Report
A 28-year-old man presented to a chiropractic teaching clinic with a chief complaint of left ankle pain 5 days after an inversion injury while playing basketball. Clinical findings included inability to fully bear weight on the left, pain provoked while walking, moderate localized swelling over the left lateral ankle joint and point tenderness over the left lateral malleolus. No ecchymosis was noted. Positive orthopedic tests included anterior drawer and varus stress testing. He was diagnosed clinically with a grade II ATFL sprain and underwent conservative treatment directed at ankle stabilization and proprioceptive rehabilitation. Twelve weeks after initiating treatment he sustained an insidious exacerbation of left ankle pain. Ultrasonography of the left ankle was performed using a GE LOGIQ E9 US system (GE Healthcare, Milwaukee, WI) operating with an 8- to 15-MHz linear array transducer to evaluate for internal derangement and to assess the dynamic stability of the lateral ankle ligaments. During the US examination, a full thickness ATFL tear was visualized without power Doppler activity indicating the likelihood of chronic ligament injury (Fig 1). Laxity and partial thickness tear of the CFL was visualized during varus stress testing. Ankle joint and talonavicular osseous hypertrophic changes consistent with osteoarthritis were noted. Additionally, forceful dorsiflexion provoked anterior ankle pain due to bony impingement subsequent to these osteoarthritic changes (Fig 2). Other US findings also included remote deltoid ligamentous complex injury, fibularis (peroneus) and posterior tibialis tenosynovitis, and a large ankle joint effusion with synovial hypertrophy and synovitis. In order to further evaluate the osteoarthritic changes, radiography of the ankle was performed. Radiographic examination demonstrated joint space narrowing within the ankle joint, talar ridging, juxta-articular osteophytes at the talonavicular joint, and multiple corticated ossicles within the ankle joint supporting a diagnosis of osteoarthritis complicated by secondary synovial chondrometaplasia (Fig 3). The patient provided consent for publication of their de-identified healthcare information.
Fig 1.

Ultrasound image of a normal ATFL (A) for comparison with the same region of the anterolateral ankle in our patient (B). The normal ATFL (arrows in image A) demonstrates a hyperechoic compact fibrillar pattern between its attachment to both the fibula (fib) and talus (tal). In our patient (image B), the ATFL is notably absent due to chronic tearing and has been replaced by disorganized, hypoechoic (dark) synovial tissue (asterisks).
Fig 2.
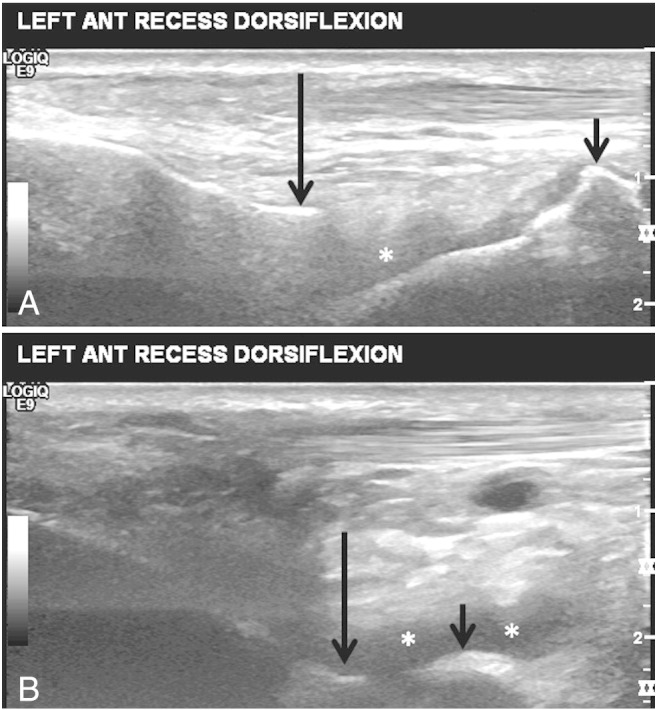
Images taken from a cine of ankle dorsiflexion with the US transducer in long axis to the tibia. Image A is the beginning of dorsiflexion. Note the hyperechoic tibial cortex (long arrow) and hyperechoic degenerative talar ridging (short arrow). A small amount of hypoechoic joint fluid is also seen (asterisk). At end-range dorsiflexion (image B), appreciate the near abutment of the tibia (long arrow) and talar ridges (short arrow). Also, there has been a modest increase in the amount of joint fluid (asterisks). Visualization of abutment of these bony structures correlated with the patient’s symptom of anterior ankle pain, a finding consistent with an impingement syndrome.
Fig 3.
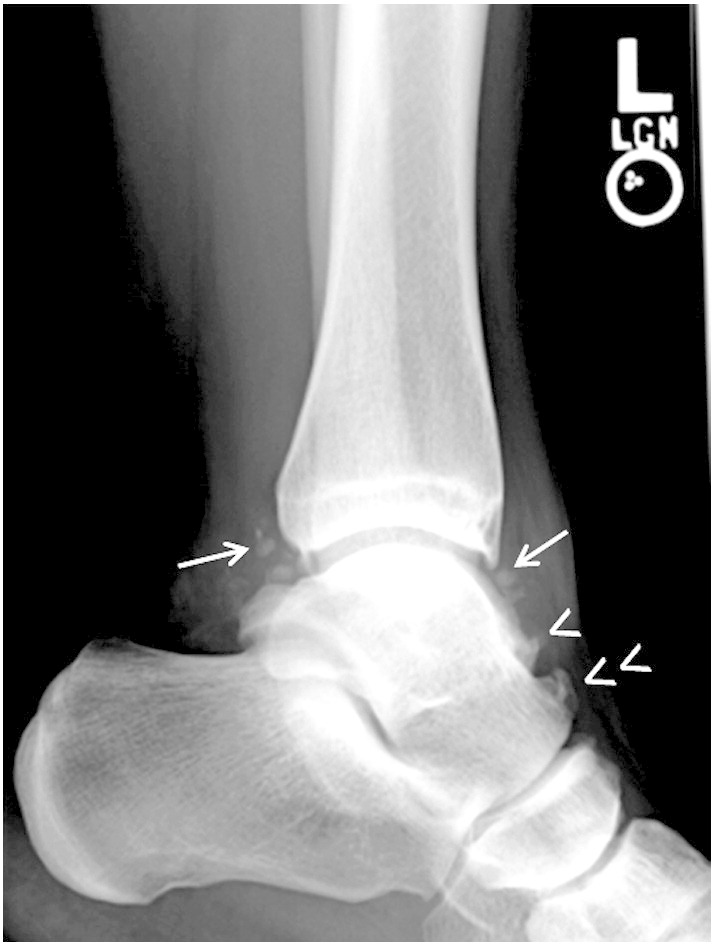
Lateral radiograph of the left ankle demonstrates degenerative changes consisting of multiple osteochondral loose bodies (secondary synovial chondromatosis; arrows), ridging of the talus at the presumed joint capsule attachment (arrowhead) and an additional osteophyte at the talonavicular articulation (double arrowheads).
Discussion
Ultrasonography and radiography were utilized to diagnose the multiple ankle ligamentous injuries sustained by this patient and the presumed osteoarticular sequelae. Importantly, US provided a real-time dynamic examination of the impaired ligamentous structures likely contributing to chronic joint instability and recurrent exacerbation of symptoms. In addition, US enabled visualization of ankle joint and talonavicular osteoarthritis. These findings were confirmed with radiography. Furthermore, due to the capacity to correlate the visualized bony impaction with symptoms of anterior ankle joint pain, a diagnosis of anterior impingement was established during real time US examination. Therefore, in this case, US provided pertinent and timely clinical information regarding the functional impairments of the patient’s ankle.
Impingement syndromes of the ankle can be an important cause of chronic pain and often arise post-injury.5 Recurrent injury, long-term ligament laxity and subsequent joint instability lead to the development of abnormal osseous and soft tissue thickening causing impingement syndromes of the ankle.5 Mechanical instability, often seen after inversion ankle injuries, is connected to the anatomic abnormalities of the ankle and related to ligament laxity.9 Functional instability relates to posture, muscle, and proprioceptive deficits, and is also commonly associated with inversion injuries.9 These mechanical and functional deficits contribute to the aberrant healing process and patients become high-risk for developing impingement syndromes as seen in our case. Considering the extensive degenerative changes present, it is likely the patient in this current case has suffered multiple remote ankle injuries. Osteophytosis and synovitis are known sequelae of chronic ankle injury and, if present anteriorly, may provoke impingement, characterized by limitation in dorsiflexion with concurrent pain at end range.5 In this case, US successfully demonstrated multiple ligament injuries with joint laxity and ankle degeneration with subsequent bony impingement providing important information with regard to ankle function and circumventing more expensive imaging such as MRI. Although conflicting reports exist describing the diagnostic accuracy of US in diagnosing anterolateral ankle impingement,10, 11 there is understandably high interest to continue to explore the utility of US in diagnosing impingement syndromes around the ankle.12 The findings of our case suggest that US is valuable in establishing the diagnosis of anterior ankle impingement.
The diagnostic performance of US in evaluating the ATFL has been described. In one study using arthroscopy as the reference standard, US demonstrated 91% accuracy in diagnosing ATFL injury compared to 67% for stress radiography and 97% MRI.13 Although MRI is a valuable tool for diagnosis of lateral ligament ankle injuries, US appears comparable in performance, is readily available and lower in cost, portable and less time consuming.13 Additionally, dynamic maneuvers can be performed by the US examiner when an abnormality is detected. For example, Croy et al studied the difference (mm) of the talofibular interval using stress US in the neutral, anterior drawer, and inversion stress positions in participants with acute inversion sprains.1 Despite self-reported functional improvement, US provided the talofibular interval distance at rest and with stress showing only marginal improvement 6 weeks post-injury.1 This is clinically important because chronic instability increases the risk of repeated episodes of future sprains.2 Therefore, US appears to be beneficial in reproducibly quantifying lateral ligamentous damage and instability and may therefore guide treatment.1 For example, a treatment outcome may be stability of the tibiotalar interval with stress under US visualization. Presumably, this treatment goal would take longer to achieve after the patient is pain free, and may impact the return to play time, subsequent re-injury and co-morbidities such as osteoarthritis and functional impingement. This is an area requiring further research. Furthermore, US is safe, utilizes no ionizing radiation, is portable, widely available, and cost-effective. US can be performed at less cost and with greater availability than MRI. These features support US imaging as an attractive clinical and research tool.
Although US has been shown to be clinically beneficial in evaluation of the ATFL, false positives have been documented.13 In such cases, a hypoechoic zone was seen in the ligament mimicking a tear, although arthroscopic visualization of the ligament was normal.13 It was thought that intraligamentous partial tearing or degeneration was responsible for producing the hypoechoic region on US.13 Additionally, the oblique orientation of the fibers of the ATFL makes it susceptible to anisotropy artifact, which is a hypoechoic finding arising from loss of beam perpendicularity.14 It is crucial during the US examination to apply an inversion stress and to angle the US transducer back and forth to limit the artifact of anisotropy. Also, a significant drawback for US diagnosis is its operator dependence and steep learning curve.
Limitations
As this is a case report there are inherent limitations and the findings of this case cannot necessarily be generalized to other patients or the general public.
Conclusion
This case report exemplifies the value and utility of US in diagnosing derangement in ligamentous, tendinous, articular, and osseous injuries of the ankle.
Funding Sources and Conflicts of Interest
No funding sources or conflicts of interest were reported for this study.
References
- 1.Croy T., Saliba S., Saliba E., Anderson M.W., Hertel J. Talofibular interval changes after acute ankle sprain: a stress ultrasonography study of ankle laxity. J Sport Rehabil. 2013;22(4):257–263. doi: 10.1123/jsr.22.4.257. [DOI] [PubMed] [Google Scholar]
- 2.Golditz T., Steib S., Pfeifer K. Functional ankle instability as a risk factor for osteoarthritis: using T2-mapping to analyze early cartilage degeneration in the ankle joint of young athletes. Osteoarthritis Cartilage. 2014;22:1377–1385. doi: 10.1016/j.joca.2014.04.029. [DOI] [PubMed] [Google Scholar]
- 3.Fong D.T., Chan Y.Y., Mok K.M., Yung P., Chan K.M. Understanding acute ankle ligamentous sprain injury in sports. Sports Med Arthrosc Rehabil Ther Technol. 2009;1:14. doi: 10.1186/1758-2555-1-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Valderrabano V., Hintermann B., Horisberger M., Fung T.S. Ligamentous posttraumatic ankle osteoarthritis. Am J Sports Med. 2006;34(4):612–620. doi: 10.1177/0363546505281813. [DOI] [PubMed] [Google Scholar]
- 5.Robinson P., White L.M. Soft-tissue and osseous impingement syndromes of the ankle: role of imaging in diagnosis and management. Radiographics. 2002;22(6):1457–1469. doi: 10.1148/rg.226025034. [discussion 70–1] [DOI] [PubMed] [Google Scholar]
- 6.De Maeseneer M., Marcelis S., Jager T. Sonography of the normal ankle: a target approach using skeletal reference points. AJR Am J Roentgenol. 2009;192(2):487–495. doi: 10.2214/AJR.08.1316. [DOI] [PubMed] [Google Scholar]
- 7.Gun C., Unluer E.E., Vandenberk N., Karagoz A., Senturk G.O., Oyar O. Bedside ultrasonography by emergency physicians for anterior talofibular ligament injury. J Emerg Trauma Shock. 2013;6(3):195–198. doi: 10.4103/0974-2700.115340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cheng Y., Cai Y., Wang Y. Value of ultrasonography for detecting chronic injury of the lateral ligaments of the ankle joint compared with ultrasonography findings. Br J Radiol. 2014;87 doi: 10.1259/bjr.20130406. 20130406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bonnel F., Toullec E., Mabit C., Tourne Y., Sofcot Chronic ankle instability: biomechanics and pathomechanics of ligaments injury and associated lesions. Orthop Traumatol Surg Res. 2010;96(4):424–432. doi: 10.1016/j.otsr.2010.04.003. [DOI] [PubMed] [Google Scholar]
- 10.McCarthy C.L., Wilson D.J., Coltman T.P. Anterolateral ankle impingement: findings and diagnostic accuracy with ultrasound imaging. Skeletal Radiol. 2008;37(3):209–216. doi: 10.1007/s00256-007-0411-6. [DOI] [PubMed] [Google Scholar]
- 11.Cochet H., Pele E., Amoretti N., Brunot S., Lafenetre O., Hauger O. Anterolateral ankle impingement: diagnostic performance of MDCT arthrography and sonography. AJR Am J Roentgenol. 2010;194(6):1575–1580. doi: 10.2214/AJR.09.3650. [DOI] [PubMed] [Google Scholar]
- 12.Pesquer L., Guillo S., Meyer P., Hauger O. US in ankle impingement syndrome. J Ultrasound. 2014;17(2):89–97. doi: 10.1007/s40477-013-0054-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Oae K., Takao M., Uchio Y., Ochi M. Evaluation of anterior talofibular ligament injury with stress radiography, ultrasonography and MR imaging. Skeletal Radiol. 2010;39(1):41–47. doi: 10.1007/s00256-009-0767-x. [DOI] [PubMed] [Google Scholar]
- 14.Milz P., Milz S., Putz R., Reiser M. 13 MHz high-frequency sonography of the lateral ankle joint ligaments and the tibiofibular syndesmosis in anatomic specimens. J Ultrasound Med. 1996;15(4):277–284. doi: 10.7863/jum.1996.15.4.277. [DOI] [PubMed] [Google Scholar]