

Abstract
AIM: To reveal the correlation between the functional differentiation phenotypes of gastric carcinoma cells and the invasion and metastasis by a new way of cell-function classification.
METHODS: Surgically resected specimens of 361 gastric carcinomas(GC) were investigated with enzyme-, mucin-, and tumor-related marker immunohistochemistry. According to the direction of cell-function differentiation, stomach carcinomas were divided into five functionally differentiated types.
RESULTS: ① Absorptive function differentiation type (AFDT): there were 82 (22.7%) patients including 76 (92.7%) aged 45 years. Sixty-nine (84.1%) cases belonged to the intestinal type. Thirty-eight (46.3%) expressed CD44v6 and 9 (13.6%) of 66 male patients developed liver metastasis. The 5-year survival rate of patients in this group (58.5%) was higher than those with the other types (P < 0.01). ② Mucin secreting function differentiation type (MSFDT): 54 (15%) cases. Fifty-three (98.1%) tumors had penetrated the serosa, 12 (22.2%) expressed ER and 22 (40.7%) expressed CD44v6. The postoperative 5-year survival rate was 28.6%. ③ Absorptive and mucin-producing function differentiation type (AMPFDT): there were 180 (49.9%) cases, including 31 (17.2%) aged yanger than 45 years. The tumor was more common in women (62, 34.4%) and expressed more frequently estrogen receptors (ER) (129, 81.7%) than other types (P < 0.01). Ovary metastasis was found in 12 (19.4%) out of 62 female subjects. The patients with this type GC had the lowest 5-year survival rate (24.7%) among all types. ④ Specific function differentiation type (SFDT): 13 (3.6%) cases. Nine (69.2%) tumors of this type derived from APUD system, the other 4 (30.7%) were of different histologicaldifferentiation. Sixty per cent of the patients survived at least five years. ⑤ Non-function differentiation type (NFDT): 32 (8.9%) cases. Nineteen (59.%) cases had lymph node metastases but no one with liver or ovary metastasis. The 5-year survival rate was 28.1%.
CONCLUSION: This new cell-function classification of GC is helpful in indicating the characteristics of invasion and metastasis of GC with different cell-function differentiation phenotypes. Further study is needed to disclose the correlation between the cell-functional differentiation phenotypes and the relevant genotypes and the biological behavior of gastric carcinoma.
Keywords: stomach neoplasms, cell differentiation, lymphatic metastasis, prognosis, cell-function classification, immunohistochemistry, absorptive function differentiation type
INTRODUCTION
Gastric carcinoma is one of the most common malignancies and has the highest mortality in China[1,2]. The most important reason causing patients’ death is the metastasis to distant important organs. It was reported that 64.2% of gastric carcinomas developed distant organ metastases, among which the rate of liver metastasis was 31.8% of all patients, and ovary metastasis rate was 43.6% of the female patients[3]. As liver is the biggest parenchymatous organ in the body, the micrometastasis of it is very difficult to be diagnosed early. The same is true in ovary metastasis because ovaries lie in the bottom of abdominal cavity. There has been no good indicator so far to objectively predict the risk of liver and ovary metastases, making the diagnosis for micrometastases of these two organs very difficult. The present study put forward a new classification of gastric carcinoma based on the cell-function differentiation features, in an attempt to reveal the relationship between the characteristics of cell-function differentiation and the local invasion and distant organ metastases of gastric carcinomas, and to clarify the causes and molecular mechanism of metastasis to the liver or ovary.
MATERIALS AND METHODS
Subjects
Three hundred and sixty-one cases of surgically resected gastric carcinomas (from Cancer Institute, China Medical University) were involved in the study, consisting of 258 men and 103 women, including 11 without metastasis, 224 with lymph node metastases, 12 with liver metastases, and 14 with ovary metastases. At least 2 blocks were cut from each primary tumor and 1 block from each metastatic tumor of any organ involved respectively.
Principle and standards of cell-functional differentiation classification
Glandular epithelial cells of gastrointestinal tract can be divided into three main groups: ① absorptive cells of the small intestine, ② mucinous cells including goblet and columnar mucous cells; and ③ cells with specific secretary function, such as parietal, chief, paneath, and APUD system cells. According to the principle that cancer cells maintain more or less the functional differentiation potential of their ancestors, a group of comprehensive indicators that could objectively reflect absorptive, mucin-secreting, and specific function differentiation were selected: indicators of absorptive function differentiation were brush border enzymes, such as alkaline phosphatase (AKP) and L-aminopeptidase (LAP); indicators of mucin secreting function differentiation were sulfomucin (HID+), sialomucin (ABpH2.5+) and neutral mucin (PAS+), and indicators of specific function differentiation were antibodies to hormones produced by APUD cells, cellular keratin and others. According to the expressions of these indicators, the gastric carcinomas were divided into five cell-function differentiation types: ① gastric carcinomas, in which more than two thirds of cancer cells expressed AKP and LAP but did not secrete mucin or hormone, were defined as absorptive function differentiation type (AFDT); ② those in which more than two thirds of the cancer cells secreted only mucin but not AKP or LAP, were defined as mucin secreting function differentiation type (MSFDT); ③ those in which more than two thirds of the cancer cells not only expressed AKP and LAP but also produced mucin, were defined as absorptive and mucin-producing function differentiation type (AMPFDT); ④ those which neither expressed AKP and LAP nor produced mucin, were defined as non-function differentiation type (NFDT); and ⑤ specific function differentiation type (SFDT) was defined as that more than two thirds of cancer cells possessed some special functions, such as the tumors from APUD system and squamous cell cancer (Table 1 and Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6).
Table 1.
Standards of cell-function classification of gastric carcinoma
| Type |
Brush border enzyme |
Mucin |
Immunohistochemistry |
||||
| AKP | LAP | HID | ABpH2.5 | PAS | Ch-A | Keratin | |
| AFDT | + | + | - | - | - | - | - |
| MSFDT | - | - | + | + | + | - | - |
| ANOFDT | + | + | + | + | + | - | - |
| SFDT | - | - | - | - | - | + | +* |
| NFDT | - | - | - | - | - | - | - |
*Chosen according to practice.
Figure 1.
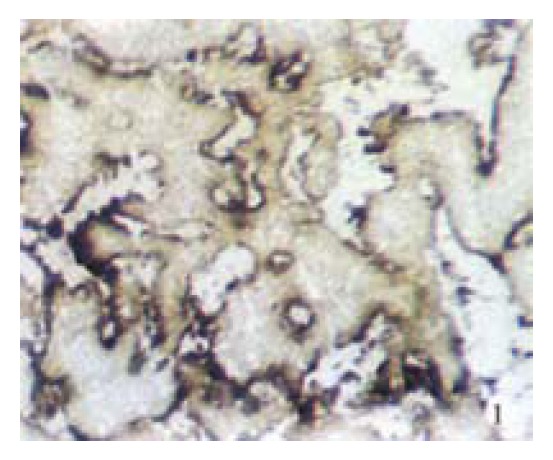
Primary stomach cancer of AFDT with liver metastasis. AKP was moderately positive and distributed along the free edge of cancerous papillary structure. Frozen section. × 20
Figure 2.
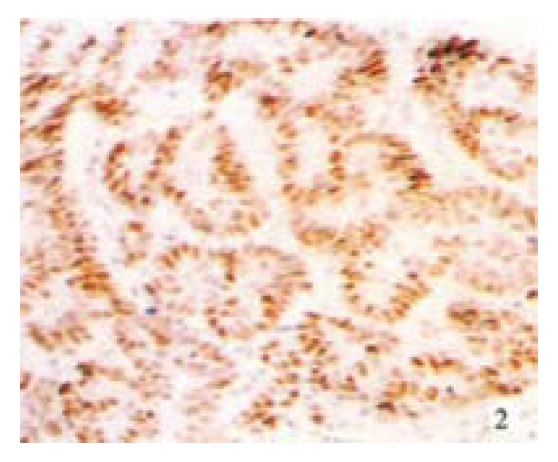
The same case in Figure 1, Tp53 protein was expressed in most of primary cancer cells. Immunostain, × 16
Figure 3.
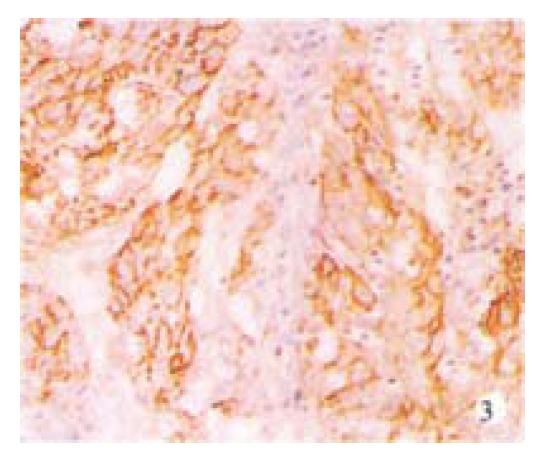
The same case of Figure 1. CD44v6 was expressed in most of primary cancer cells. Immunostain, × 20
Figure 4.
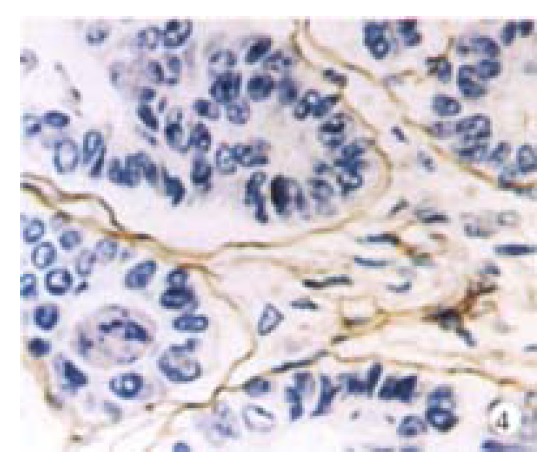
The same case of Figure 1. There was obvious basement membrane like structure with Laminin positive in the primary tumor. Immunostain, × 40
Figure 5.
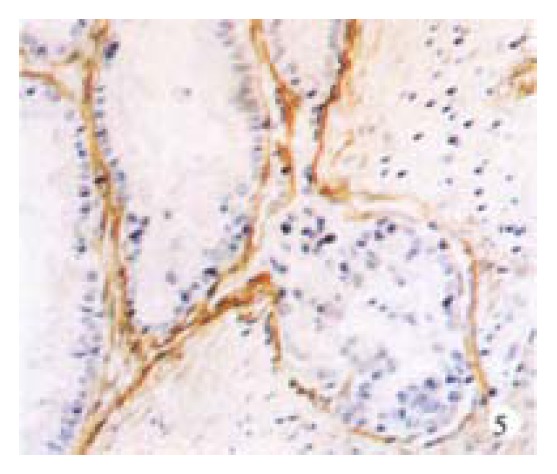
The same case of Figure 1. There was also obvious basement membrane like structure with laminin positive in the liver metastatic tumor. Immunostain, × 20
Figure 6.
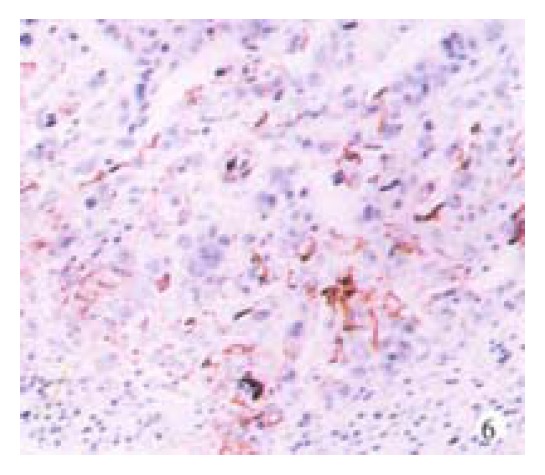
The same case of Figure 1. CD44v6 was also expressed in the liver metastatic cancer cells. Immunostain, × 20
Detection of cell-functional differentiations
Enzyme histochemistry[4]: alkaline phosphatase (AKP) was detected by Gomori’s method, and L-aminopeptidase (LAP) by Nachal’s method. Mucin histochemistry was done by the HID/ABpH2.5/PAS method[5]; endocrine histochemistry was performed by ABC immunostaining with antibodies to hormones produced by APUD cells. The results were evaluated using the standards given in references[6,7].
Detection of tumor associated markers[8-13]
The sections from all cases were stained by ABC histochemistry using antibodies to ER and CD44v6 respectively. The ploidy of DNA patterns of the cases with liver or ovary metastasis was examined by flow cytometry (FCM). p53 and laminin expressions in the gastric carcinomas with liver or ovary metastasis were also detected immunohistochemically.
Statistics
χ2 test was employed in this study to analyze the results of histochemistry and survival data.
RESULTS
The carcinomas were divided into five types: 82 cases classified as AFDT (22.7%); 54 MSFDT (15%); 180 AMPFDT (49.9%); 32 NFDT (8.9%) and 13 SFDT (3.6%). Table 2 and Table 3 illustrate the relationship between the cell function classification and the patients’ age and sex. The relationship between the cell-function classification and histological types, growth patterns, clinicopathological stages, ER expression, CD44v6 expression, ability forming laminin-positive basement membraneous structure, lymph node metastasis, liver and ovary metastases, and postoperative 5-year survival rates are shown in Table 4, Table 5, Table 6, Table 7, Table 8, Table 9, Table 10, Table 11, Table 12, Table 13 and Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8, Figure 9, Figure 10, Figure 11, Figure 12.
Table 2.
Relationship between cell function classification and age of patients with gastric carcinoma
| Type | n |
Age |
||
| < 45 yrs (%) | 45-65 yrs (%) | > 65 yrs (%) | ||
| AFDT | 82 | 6 (7.3) | 59 (72.0) | 17 (20.7) |
| MSFDT | 54 | 2 (3.7) | 43 (79.6) | 9 (14.7) |
| AMPFDT | 180 | 31 (17.2)a | 118 (65.5) | 31 (17.2) |
| SFDT | 13 | 1 (7.7) | 9 (69.2) | 3 (23.1) |
| NFDT | 32 | 6 (18.8) | 17 (53.1) | 9 (28.1) |
| Total | 361 | 46 (12.7) | 246 (68.1) | 69 (19.1) |
P < 0.05 (χ2 = 4.5575), vs AFDT of the patients below 45 years old.
Table 3.
Relationship between cell-function classification and sex of patients with gastric carcinoma
| Type | n |
Female (%) |
Male (%) |
||
| n | % | n | % | ||
| AFDT | 82 | 16 | (19.5) | 66 | (80.5) |
| MSFDT | 54 | 15 | (27.8) | 39 | (72.2) |
| AMPFDT | 180 | 62 | (34.4)a | 118 | (65.6) |
| SFDT | 13 | 3 | (23.1) | 10 | (76.9) |
| NFDT | 32 | 7 | (21.9) | 25 | (78.1) |
| Total | 361 | 103 | (28.5) | 258 | (71.5) |
P < 0.05 (χ2 = 6.0079), vs AFDT of female patients.
Table 4.
Relationship between cell-function and WHO’s histological classifications of gastric carcinoma
| Types | n | AFDT (%) | MSFDT (%) | AMPFDT (%) | SFDT (%) | NFDT (%) |
| Papillary adenocarcinoma | 37 | 29 (78.4)a | 2 (5.4) | 6 (16.2) | 0 | 0 |
| Tubular adenocarcinoma | ||||||
| Well-diff. ade. | 20 | 17 (85.0) | 0 | 2 (10.0) | 0 | 1 (5.0) |
| Mode. diff. ade. | 59 | 20 (33.9) | 5 (8.5) | 27 (45.8) | 1 (1.7) | 6 (10.2) |
| Poor. diff. ade. | 126 | 15 (11.9) | 14 (11.1) | 79 (62.7) | 2 (1.6) | 16 (12.7) |
| Undiff. car. | 30 | 1 (3.3) | 7 (23.3) | 13 (43.3) | 0 | 9 (30.0) |
| SRC | 41 | 0 | 5 (12.2) | 6 (87.8)b | 0 | 0 |
| Mucous ade. | 38 | 0 | 21 (55.3) | 17 (44.7) | 0 | 0 |
| Carcinoid | 9 | 0 | 0 | 0 | 9 (100.0) | 0 |
| Squamous car. | 1 | 0 | 0 | 0 | 1 (100.0) | 0 |
| Total | 361 | 82 (22.7) | 54 (15.0) | 180 (49.9) | 13 (3.6) | 32 (8.9) |
P < 0.01 (χ2 = 28.6784), vs others of the papillary adenocarcinomas;
P < 0.01 (χ2 = 46.8780), vs others of signetring cell carcinomas. ade: Adenocarcinoma; diff.: Differentiated; mode.: Moderately; undiff.: Undifferentiated; SRC: Signet ring cell carcinoma
Table 5.
Relationship between cell-function and Lauren£§s classifications of gastric carcinoma
| Types | n (%) | AFDT (%) | MSFDT (%) | AMPFDT (%) | SFDT (%) | NFDT (%) |
| Intestinal | 124 (36.4) | 69 (84.1)a | 11 (20.4) | 33 (18.3) | 11 (84.6)b | 0 |
| Diffuse | 237 (63.6) | 13 (15.9) | 43 (79.6) | 147 (81.7) | 2 (15.4) | 32 (100.0) |
| Total | 361 | 82 | 54 | 180 | 13 | 32 |
P < 0.01 (χ2 = 102.6339), vs AMPFDT;
P < 0.01 (χ2 = 15.11320), vs AMPFDT.
Table 6.
Relationship between cell-function classification and histological growth patterns of gastric carcinomas
| Patterns | n (%) | AFDT (%) | MSFDT (%) | AMPFDT (%) | SFDT (%) | NFDT (%) |
| Mass | 19 (6.1) | 12 (19.4) | 0 | 0 | 7 (53.8) | 0 |
| Nest | 84 (27.0) | 37 (59.7) | 12 (22.2) | 23 (14.8) | 6 (46.2) | 6 (22.2) |
| Diffuse | 208 (66.9) | 13 (21.0)a | 42 (77.8) | 132 (85.2) | 0 | 21 (77.8) |
| Total | 311 | 62 (19.9) | 54 (17.4) | 155 (49.8) | 13 (4.2) | 27 (8.7) |
P < 0.01 (Exact test: χ2 = 12.2793), vs MSFDT, AMPFDT and NFDT.
Table 7.
Relationship between cell-function classification and clinicopathological stages of gastric carcinomas
| Stages | n (%) | AFDT (%) | MSFDT (%) | AMPFDT (%) | SFDT (%) | NFDT (%) |
| EGC | 50 (13.9) | 20 (24.4) | 0 | 25 (13.9) | 0 | 5 (15.6) |
| AGC | ||||||
| Subserosa | 42 (11.6) | 8 (9.8) | 1 (1.9) | 28 (25.6) | 1 (7.7) | 4 (12.5) |
| Through serosa | 269 (74.5) | 54 (65.9) | 53 (98.1)a | 127 (70.6) | 12 (92.3) | 23 (71.9) |
| Total | 361 | 82 | 54 | 180 | 13 | 32 |
P < 0.01 (χ2 = 10.1203, 8.9078 and 6.7487 respectively), vs AFDT, AMPFDT and NFDT.
Table 8.
Relationship between cell-function classification and ER expression of gastric carcinomas
| ER expression | AFDT | MSFDT | AMPFDT | SFDT | NFDT | Total |
| Positive/examined | 7/82 | 12/54 | 129/180 | 0/13 | 7/32 | 155/361 |
| Positive rate (%) | 8.5 | 22.2 | 71.7a | 21.9 | 42.9 |
P < 0.01 (χ2 = 45.6418), vs others.
Table 9.
Relationship between cell-function classification and CD44v6 expression in gastric carcinoma tissues
| CD44v6 | n | AFDT (%) | MSFDT (%) | AMPFDT (%) | SFDT (%) | NFDT (%) |
| - | 241 | 44 | 32 | 132 | 9 | 24 |
| + (%) | 120 (33.2) | 38 (46.3)a | 22 (40.7)b | 48 (26.7) | 4 (30.8) | 8 (25.0) |
| Total | 361 | 82 | 54 | 180 | 13 | 32 |
P < 0.01 (χ2 = 9.8900), vs AMPFDT;
P < 0.05 (χ2 = 3.9245), vs AMPFDT.
Table 10.
Relationship between cell-function classification and metastases of gastric carcinomas
| Types | n (%) | AFDT (%) | MSFDT (%) | AMPFDT (%) | SFDT (%) | NFDT (%) |
| No mets | 111 (30.7) | 28 (34.1) | 13 (24.1) | 51 (28.3) | 6 (46.2) | 13 (40.6) |
| LN mets | 224 (62.0) | 45 (54.9) | 38 (70.4) | 116 (64.4) | 6 (46.2) | 19 (59.4) |
| Liver mets | 12 (3.3) | 9 (11.0)a | 1 (1.9) | 1 ( 0.6) | 1 (7.7) | 0 |
| Ovary mets | 14 (3.9) | 0 | 2 (3.7) | 12 (6.7) | 0 | 0 |
| Total | 361 | 82 (22.7) | 54 (15.0) | 180 (49.9) | 13 (3.6) | 32 (8.9) |
P < 0.05 (Exact test: χ2 = 5.4385), vs AMPFDT. Mets: Metastasis; LN: Lymph node.
Table 11.
Relationship among cell-function classification, metastasis and sex of patients with gastric carcinoma
| Types |
Liver metastasis |
Ovary metastasis | |
| Male (%) | Female (%) | ||
| AFDT | 9/66 (13.6)a | 0/16 | 0/16 |
| MSFDT | 0/39 | 1/15 (6.7) | 2/15 (13.3) |
| AMPFDT | 1/118 (0.8) | 0/62 | 12/62 (19.4)b |
| SFDT | 1/10 (10.0) | 0/3 | 0/3 |
| NFDT | 0/25 | 0/7 | 0/7 |
| Total | 11/258 (4.3) | 1/103 (1.0) | 14/103 (13.6) |
P < 0.01 (Exact test χ2 = 8.9527), vs AMPFDT of the male with liver metastasis;
P < 0.05 (Exact test χ2 = 4.2992), vs AFDT, SFDT and NFDT of the female with ovary metastasis.
Table 12.
Comparison of cell-function differentiation classification and molecular biological features of gastric carcinoma with liver or ovary metastases
| Comparison |
GC with liver mets. |
GC with ovary mets. |
| Positive/12 cases (%) | Positive/14 cases (%) | |
| Cell-function differentiation types | ||
| AFDT | 9 (75.0)a | 0 |
| MSFDT | 1 (8.3) | 2 (14.3) |
| AMPFDT | 1 (8.3) | 12 (85.7)b |
| SFDT | 1 (8.3) | 0 |
| NFDT | 0 | 0 |
| Comparison of molecular biological features | ||
| Estrogen-dependent ER (+) | 0 | 12 (85.7)c |
| LN (+) BM structure (+) | 12 (100.0) | 0 |
| Mutant p53 protein (+) | 10 (83.3)d | 3 (21.4) |
| DNA ploidy:Diploid | 3 (25.0) | 10 (71.4) |
| Tetraploid | 0 | 2 (14.3) |
| Aneuploid | 9 (75.0)e | 2 (14.3) |
| CD44v6 expression (+) | 10 (83.3)f | 0 |
LN: Laminin; BM: Basement membrane; Mets: Metastasis
P < 0.01 (Exact test χ2 = 12.9160), vs AFDT with ovary mets;
P < 0.01 (Exact test χ2 = 12.5357), vs AMPFDT with liver mets;
P < 0.01 (Exact test χ2 = 15.8087), vs GC with liver mets;
P < 0.01 (Exact test χ2 = 7.5833), vs GC with ovary mets;
P < 0.01 (Exact test χ2 = 6.0420), vs GC with ovary mets;
P < 0.05 (Exact test χ2 = 15.6010), vs GC with ovary mets.
Table 13.
Relationship between postoperative survival rates and cell function classification of gastric carcinomas
| Types | n | Cases survived over 5 years (%) | |
| AFDT | 82 | 48 | (58.5)a |
| MSFDT | 49 | 14 | (28.6) |
| AMPFDT | 174 | 43 | (24.7) |
| SFDT | 5 | 3 | (60.0) |
| NFDT | 32 | 9 | (28.1) |
| Total | 342 | 117 (34.2) | |
P < 0.01 (χ2 = 11.0478, 28.7138 and 10.3250), vs MSFDT, AMPFDT and NFDT, respectively.
Figure 7.
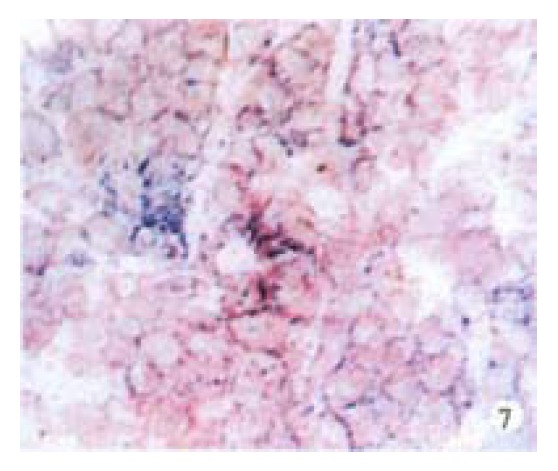
Primary gastric carcinoma of AMPFDT with ovary metastasis. LAP was moderately positive and distributed in the membrane and cytoplasm of cancer cells. Frozen section, × 40
Figure 8.
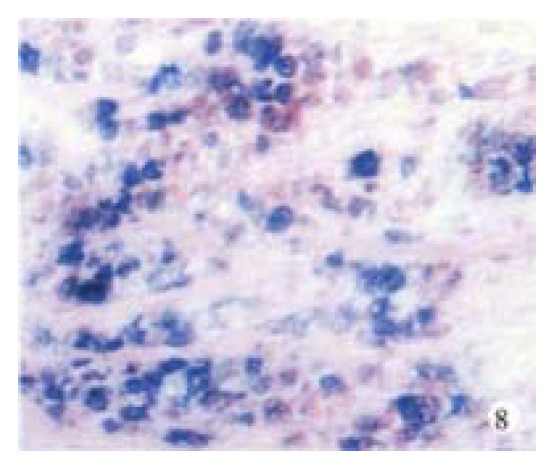
The same case of Figure 7. Sialomucin and neutral mucin were positive in the primary cancer cells. Mucin histochemistry, × 20
Figure 9.
The same case of Figure 7. Most of primary cancer cells expressed ER, which was distributed in the nuclei and cytoplasm. Immunostain, × 20
Figure 10.
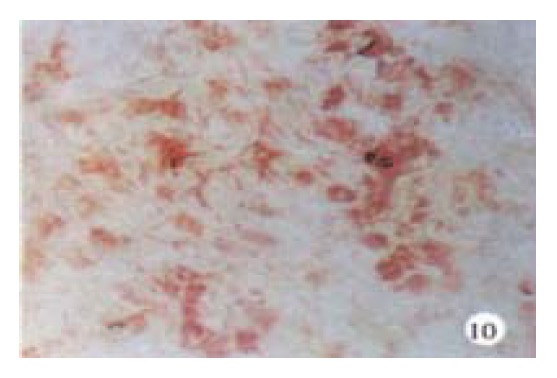
The same case of Figure 7. LAP was moderately positive in the ovary metastatic cancer cells. Frozen section, × 20
Figure 11.
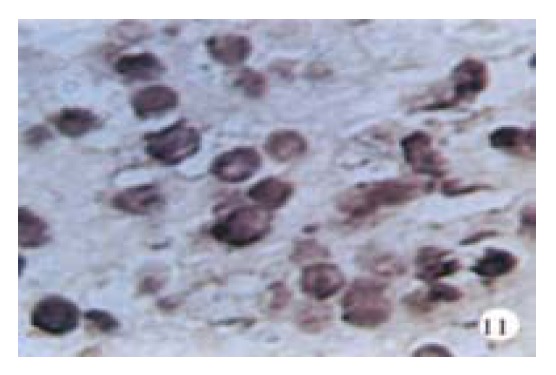
The same case of Figure 7. Sulfomucin was positive in the ovary metastatic cancer cells. Mucin histochemistry, × 40
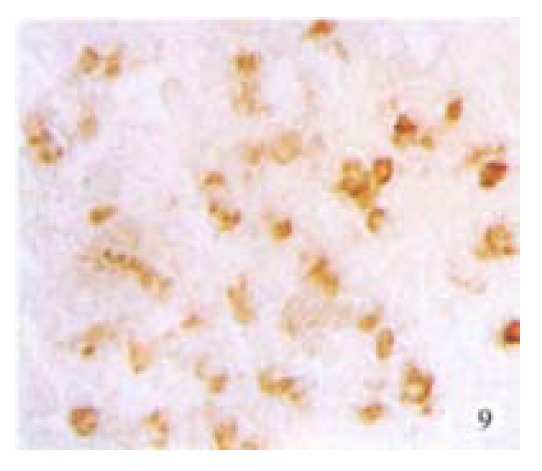
Figure 12.
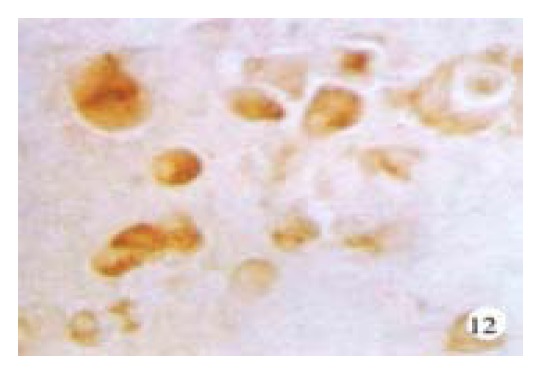
The same case of Figure 7. Most of the ovary metastatic cancer cells expressed ER. Immunostain, × 40
DISCUSSION
In the light of differentiation degree, malignant tumors from epithelial cells of gastrointestinal tract may retain more or less the functional differentiation potential of their ancestors, which has effects on their biological behavior. Previous studies revealed the relationship between the morphological differentiation and the pathobiological behavior of gastric cancer[14-22], but so far there have been very few studies on the phenotypes of functional differentiation of gastric cancer cells[23-25]. We have studied simple morphological and the functional differentiation indicators of gastric carcinoma to infer its biological behavior during last fifteen years, and found that there was a correlation between the functional differentiation of gastric carcinoma cells and their biological behavior[26-32]. In this study, we investigated more cases and compared the degree of functional differentiation and morphological differentiation features of gastric carcinomas, and found no definite correlation between them. Although most well-differentiated papillary and tubular adenocarcinomas possessed absorptive functions, all signet ring cell cancers were classified as AMPFDT and carcinoid tumors as SFDT, the direction of functional differentiation of most moderately and poorly differentiated adenocarcinomas were undetermined. Most so-called undifferentiated cancers determined histologically displayed some functional differentiation, and were mostly MSFDT or AMPFDT gastric carcinomas; truly undifferentiated cancers made up only 8.3% in our study. Interestingly, 55.3% of mucinous adenocarcinomas classified by histology had mucin-secreting function (MSFDT) but the other 44.7% had absorptive and mucin-producing function (AMPFDT). Furthermore, Tumors of MSFDT were significantly different from those of AMPFDT in patient age, the serosa involvement, estrogen dependence and the CD44v6 expression. The results indicated that the cancer cells of mucinous adenocarcinoma possessed obvious heterogenicity in cell function differentiation and biological behavior, which should be paid special attention to predict the invasive and metastatic features.
The results also indicated that stomach cancers with different functional characteristics often possessed different pathobiological behavior. For example, the MSFDT tumors, constantly growing invasively, were mostly accompanied by the serosa involvement, and were not obviously dependent on estrogen. NFDT independent of estrogen invades weakly, of which about 60% metastasized to lymph node. Among different functionally differentiated gastric carcinomas, AFDT and AMPFDT had specific clinicopathologically biological features as follows. Gastric carcinomas of ATDT were most common in the middle aged and senile (92.7%), only 7.3% were found in the young; with men (80.5%) surpassing women (19.5%), and intestinal type gastric carcinoma (84.1%) exceeding diffuse ones; and exhibited mainly “mass” or “nest” styles of growth. The invasion of this type of tumor was often beneath the serosa, which resisted local infiltration as a barrier. AFDT, whose growth was not very much dependent on estrogen, expressed metastasis-associated cell adhesion molecule CD44v6 at a higher rate than AMPFDT, and its postoperative 5-year survival rate was 58.5% revealed its best prognosis. Liver metastasis was frequently observed in patients with AFDT tumor whose biological behavior was as follows: ① mutant p53 protein positively expressed at a rate of 83.3%; ② among 75.0% of cases, DNA showed aneuploid; ③ 83.3% of this type presented positive expression of CD44v6; and ④ the thread-like basement membraneous structure containing LN was often formed. Special attention should be paid clinically to the characteristics of AFDT stomach cancer mentioned above. AMPFDT gastric carcinoma often occurried in the young aged below 45 years (17.2%) with more female patients (34.3%) than in other types, and histologically, 81.7% were diffusing invasive type and 71.7% were estrogen-dependent type, and there were more ovary metastases (19.4%) than in the other types. The 5-year survival rate of 24.7% embodied the worst prognosis. AMPFDT gastric carcinoma that grew in women with ovary metastasis had the following biological behavior: 85.7% of cases had high ER expression; mutant P53 protein displayed low expression at a rate of 21.4%; no expression of metastasis-associated adhesion molecule CD44v6; and diploid DNA occurred in 71.4% of tumors. Although the molecular mechanism of liver and ovary metastases was not clear, we should pay much more attention to the cell-function differentiation and biological behavior of gastric carcinomas mentioned above in order to help with the early diagnosis and treatment of the micrometastasis in the liver and ovary.
Much attention has been paid to the mechanism of cancer invasion and metastasis[33-42], especially to the mechanism of the liver and ovary metastases from gastric carcinomas. Several hypotheses have been proposed but cannot explain the specific organic affinity satisfactorily[43-50]. Our study found that the gastric carcinomas with liver metastasis possessed different cellular biological behaviors from those with ovary metastasis (Table 10, Table 11, Table 12). It is thus possible to consider a new explanation of the mechanisms of the organic affinity of liver and ovary metastases: the fact that the gastric carcinoma with liver metastasis displayed absorptive function differentiation and expressed LN positive basement membrane-like structure suggested that these cancer cells may have increased the number of exposed laminin receptors. When the cells with exposed laminin receptors (LR) encounter the basement membrane of capillaries, the cancer cells can combine with the basement membrane by the specific affinity between LN and LR, making it possible for the cancer cells to invade the blood vessels. Therefore, we can hypothesize that the presence of exposed LR on the surface of cancer cells is an important precondition for the metastasis through the blood vessels. Most gastric cancers with ovary metastasis displayed disordered functional differentiation in the directions of absorption and mucin-production, and all these cancers expressed estrogen receptors (ER). This finding suggests that the specific organic affinity between the ovary and the specific type of gastric carcinomas may be related to an estrogen-estrogen receptor (E-ER) link.
In addition, our study found that gastric carcinomas exhibiting “mass” or “nest” growth pattern, all expressed thread-like structure containing LN. The reason for this phenomenon is probably that LR is polarized on the basal side of the cancer cells which grow in masses or nests, so these cancer cells can arrange in a row along basement membranes containing LN. On the contrary, the laminin receptors were absent or disordered on those cancer cells which grow diffusely, so that they cannot form a regular structure[51-53].
In summary, the findings of the study indicate that there was some correlation between the cell-function differentiation and invasion and metastasis of gastric carcinomas. A further study is necessary to make clear the genotypes of different functional phenotypes of gastric carcinomas and find out new molecular biological markers for the early diagnosis and treatment of the metastasis. Additionally, the remarkable difference between liver and ovary metastasis of gastric carcinoma in cell-function differentiation, P53 gene mutation, ploidy of DNA, CD44v6 expression and laminin expression indicates their different pathways of gene regulation.
Footnotes
Supported by the National Natural Science Foundation of China, No.39270300, No.39370772 and Training Program for Trans-Century Talents by the State Education Commission of China.
Edited by Ma JY
References
- 1.Li L, Lu F, Zhang S. [Analyses of variation trend and short-term detection of Chinese malignant tumor mortality during twenty years] Zhonghua Zhongliu Zazhi. 1997;19:3–9. [PubMed] [Google Scholar]
- 2.Li L, Zhang S, Lu F. [Research on characteristics of mortality spectrum and type composition of malignant tumors in China] Zhonghua Zhongliu Zazhi. 1997;19:323–328. [PubMed] [Google Scholar]
- 3.National Pathological Association of Stomach Cancer Research. Pathological study on the postmortems of 360 gastric carcinomas. Zhonghua Binglixue Zazhi. 1983;12:124–128. [Google Scholar]
- 4.Takeuchi T editor. New Enzyme Histochemistry. Tokyo: Asakura Publishing House; 1980. p. 228. [Google Scholar]
- 5.Jass JR. Sulphomucin, precancerous lesion of the human stomach. Histopathology. 1980;4:291–296. doi: 10.1111/j.1365-2559.1980.tb02921.x. [DOI] [PubMed] [Google Scholar]
- 6.Xin Y, Zhang YC, Zhang PF, Wang MX. Comparative study of cyclic nucleotide phosphodiesterases and marker enzymes of small intestinal absorptive cell in gastric cancer tissue. Zhongguo Yike Daxue Xuebao. 1991;20:333–337. [Google Scholar]
- 7.Xin Y, Wu DY, Zhang SM, Wang YP, Xu L, Zhao FK, Zhang YC. Relationship between the expression of glucagon and liver me-tastasis of gastric carcinoma. Zhongguo Yike Daxue Xuebao. 1998;27(Suppl):1–5. [Google Scholar]
- 8.Xin Y, Zhao FK, Li HZ, Zhang YC. Relationship between the expression of ER and pathobiological behavior of gastric carcinomas. Zhongguo Yike Daxue Xuebao. 1991;20:231–233. [Google Scholar]
- 9.Xin Y, Zhao F, Wu D, Wang Y, Xu L, Curran B, Leader M, Henry K. DNA ploidy, expression of p53 protein and metastatic behaviour of gastric carcinoma. Chin Med Sci J. 1996;11:147–151. [PubMed] [Google Scholar]
- 10.Xin Y, Grace A, Leader M, Kay E. CD44 splice variant 6(CD44v6) in gastric carcinomas. Lab Invest. 1999;79:495. [Google Scholar]
- 11.Xin Y, Zhao FK, Zhang SM, Wu DY, Wang YP, Xu L. Relationship between CD44v6 expression and prognosis in gastric carci-noma patients. Shijie Huaren Xiaohua Zazhi. 1999;7:210–214. [Google Scholar]
- 12.Xin Y, Zhao FK, Wu DY, Zhang PF, Zhang YC, Wang YH. Immu-nohistochemical study on the content and distribution of laminin in stomach cancer tissues. Zhongguo Yike Daxue Xuebao. 1993;22:179–181. [Google Scholar]
- 13.Xin Y, Zhao FK, Wu DY, Wang YP, Xu L, Zhang YC. Relationship between the mutation of p53 gene and infiltration,metastasis and prognosis of gastric carcinoma. Chin J Cancer Res. 1996;8:263–266. [Google Scholar]
- 14.Zhang YC, Zhang PF, Zhang WF. Study of the morphological and biological features of 60 cases of stomach cancers. Zhonghua Binglixue Zazhi. 1964;8:234–237. [Google Scholar]
- 15.Lauren P. The two histological main types of gastric carcinoma: diffuse and socalled intestinal-type carcinoma. Acta Path. 1965;64:31–37. doi: 10.1111/apm.1965.64.1.31. [DOI] [PubMed] [Google Scholar]
- 16.Ming SJ. Gastric carcinoma. Cancer. 1977;33:2475–2481. doi: 10.1002/1097-0142(197706)39:6<2475::aid-cncr2820390626>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 17.Japanese Research Society for gastric Cancer. The general rules for the gastric cancer study in surgery and pathology. Part II. Histological classification of gastric cancer. Jpn J Surg. 1981;48:2084–2087. [Google Scholar]
- 18.Watanabe H, Jass JR, Sobin LH. In collaboration with pathologists in 8 countries. Histological typing of esophageal and gastric tumors, 2nd edition. WHO International Histological Classification of Tumours. Berlin: Springer-Verlag; 1994. pp. 40–52. [Google Scholar]
- 19.UICC . TNM classification of malignant tumors. 4th edition. Hermaneck P, Sobin IH, eds. Berlin; Springer-Verlag, 1987 [Google Scholar]
- 20.Martin IG, Dixon MF, Sue-Ling H, Axon AT, Johnston D. Goseki histological grading of gastric cancer is an important predictor of outcome. Gut. 1994;35:758–763. doi: 10.1136/gut.35.6.758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Carneiro F. Classification of gastric carcinomas. Curr Diag Pathol. 1997;4:51–59. [Google Scholar]
- 22.Zhang YC, Zhang PF, Wei YH. Metastatic carcinoma of the cervix uteri from the gastrointestinal tract. Gynecol Oncol. 1983;15:287–290. doi: 10.1016/0090-8258(83)90084-7. [DOI] [PubMed] [Google Scholar]
- 23.Zhang QX, Dou YL, Shi XY, Ding Y. Expression of somatostatin mRNA in various differentiated types of gastric carcinoma. World J Gastroenterol. 1998;4:48–51. doi: 10.3748/wjg.v4.i1.48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yu JY, Wang LP, Meng YH, Hu M, Wang JL, Bordi C. Classification of gastric neuroendocrine tumors and its clinicopathologic significance. World J Gastroenterol. 1998;4:158–161. doi: 10.3748/wjg.v4.i2.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yi YF, Cheng BK. Expression of sialylated mucin-associated car-bohydrate structures in human gastric carcinoma. World J Gastroenterol. 1998;4:233. [Google Scholar]
- 26.Xin Y, Zhao FK, Wu DY, Wang YP. Comparative study of functional and histological differentiation of 104 gastric carcinomas. Zhongguo Yike Daxue Xuebao. 1993;22:259–261. [Google Scholar]
- 27.Xin Y, Zhao F, Gong W, Wang Y, Zhang Y, Yan R. A new functional classification of stomach cancer and its pathobiological and clinical significance. Chin Med Sci J. 1994;9:119–124. [PubMed] [Google Scholar]
- 28.Xin Y, Zhao FK, Wu DY, Wang YP, Zhang YC. Recommendation of a new functional classification of gastric cancer. Zhonghua Binglixue Zazhi. 1995;24:320–321. [Google Scholar]
- 29.Xin Y, Zhao FK, Wang YP, Zhang YC. Comparative study of the biological behavior of signet ring cell carcinoma and mucinous adenocarcinoma of the stomach. Zhongguo Yike Daxue Xuebao. 1996;25:441–445. [Google Scholar]
- 30.Zhao FK, Xin Y, Zhang SM. Relationship between Collagen I and Laminin and the pathobiological behavior of gastric carcinomas. Zhongguo Yike Daxue Xuebao. 1998;27(Suppl):6–8. [Google Scholar]
- 31.Xin Y, Zhao FK, Wang YP, Wu DY. Study of the biological characteristics of the metastatic tumor cells in the liver from the cancers of gastrointestinal tract. Zhongguo Yike Daxue Xuebao. 1994;23:443–445. [Google Scholar]
- 32.Xin Y, Zhao FK, Wang YP, Wu DY. Study of biological characteristics of the metastatic tumour cells in the ovary and uterus cervix from the cancers of gastrointestinal tract. Zhongguo Yike Daxue Xuebao. 1995;24:1–4. [Google Scholar]
- 33.Albelda SM. Role of integrins and other cell adhesion molecules in tumor progression and metastasis. Lab Invest. 1993;68:4–17. [PubMed] [Google Scholar]
- 34.Matsui S, Shiozaki H, Inoue M, Tamura S, Doki Y, Kadowaki T, Iwazawa T, Shimaya K, Nagafuchi A, Tsukita S. Immunohistochemical evaluation of alpha-catenin expression in human gastric cancer. Virchows Arch. 1994;424:375–381. doi: 10.1007/BF00190559. [DOI] [PubMed] [Google Scholar]
- 35.Su LK, Vogelstein B, Kinzler KW. Association of the APC tumor suppressor protein with catenins. Science. 1993;262:1734–1737. doi: 10.1126/science.8259519. [DOI] [PubMed] [Google Scholar]
- 36.Rubinfeld R, Robbins P, E1-Gamil M, Albert I, Porfiri E, Polakis P. Stabilization of β -catenin bu genetic defects in melanoma cell lines. Science. 1997;275:1790–1792. doi: 10.1126/science.275.5307.1790. [DOI] [PubMed] [Google Scholar]
- 37.Morin PJ, Sparks AB, Korinek V, Barker N, Clevers H, Vogelstein B, Kinzler KW. Activation of beta-catenin-Tcf signaling in colon cancer by mutations in beta-catenin or APC. Science. 1997;275:1787–1790. doi: 10.1126/science.275.5307.1787. [DOI] [PubMed] [Google Scholar]
- 38.Joseph-Silverstein J, Silverstein RL. Cell adhesion molecules: an overview. Cancer Invest. 1998;13:1225–1231. doi: 10.3109/07357909809050034. [DOI] [PubMed] [Google Scholar]
- 39.Postel EH. NM23-NDP kinase. Int J Biochem Cell Biol. 1998;30:1291–1295. doi: 10.1016/s1357-2725(98)00087-9. [DOI] [PubMed] [Google Scholar]
- 40.Ma D, Luyten GP, Luider TM, Jager MJ, Niederkorn JY. Association between NM23-H1 gene expression and metastasis of human uveal melanoma in an animal model. Invest Ophthalmol Vis Sci. 1996;37:2293–2301. [PubMed] [Google Scholar]
- 41.Sass PM. The involvement of selectins in cell adhesion, tumor progression, and metastasis. Cancer Invest. 1998;16:322–328. doi: 10.3109/07357909809084652. [DOI] [PubMed] [Google Scholar]
- 42.Liotta LA, Stetler-Stevenson WG. Tumor invasion and metastasis: an imbalance of positive and negative regulation. Cancer Res. 1991;51:5054s–5059s. [PubMed] [Google Scholar]
- 43.Liotta LA, Steeg PS, Stetler-Stevenson WG. Cancer metastasis and angiogenesis: an imbalance of positive and negative regulation. Cell. 1991;64:327–336. doi: 10.1016/0092-8674(91)90642-c. [DOI] [PubMed] [Google Scholar]
- 44.Stetler-Stevenson WG. Type IV collagenases in tumor invasion and metastasis. Cancer Metastasis Rev. 1990;9:289–303. doi: 10.1007/BF00049520. [DOI] [PubMed] [Google Scholar]
- 45.Hruban RH, Offerhaus GJ. Molecular diagnosis of cancer and micrometastases. Adv Anat Pathol. 1998;5:175–178. doi: 10.1097/00125480-199805000-00005. [DOI] [PubMed] [Google Scholar]
- 46.Morris VL, Schmidt EE, MacDonald IC, Groom AC, Chambers AF. Sequential steps in hematogenous metastasis of cancer cells studied by in vivo videomicroscopy. Invasion Metastasis. 1997;17:281–296. [PubMed] [Google Scholar]
- 47.Nicolson GL. Gene expression, cellular diversification and tumor progression to the metastatic phenotype. Bioessays. 1991;13:337–342. doi: 10.1002/bies.950130706. [DOI] [PubMed] [Google Scholar]
- 48.Liotta LA, Kleinerman J, Saidel GM. Quantitative relationships of intravascular tumor cells, tumor vessels, and pulmonary metastases following tumor implantation. Cancer Res. 1974;34:997–1004. [PubMed] [Google Scholar]
- 49.Meyer T, Hart IR. Mechanisms of tumour metastasis. Eur J Cancer. 1998;34:214–221. doi: 10.1016/s0959-8049(97)10129-0. [DOI] [PubMed] [Google Scholar]
- 50.Woodhouse EC, Chuaqui RF, Liotta LA. General mechanisms of metastasis. Cancer. 1997;80:1529–1537. doi: 10.1002/(sici)1097-0142(19971015)80:8+<1529::aid-cncr2>3.3.co;2-#. [DOI] [PubMed] [Google Scholar]
- 51.Liotta LA, Horan HP, Rao CN. Monoclonal antibodies to the human laminin receptor recognized structurally distinct sites. Exp Cell Res. 1985;156:117–121. doi: 10.1016/0014-4827(85)90266-6. [DOI] [PubMed] [Google Scholar]
- 52.de Manzoni G, Guglielmi A, Verlato G, Tomezzoli A, Pelosi G, Schiavon I, Cordiano C. Prognostic significance of 67-kDa laminin receptor expression in advanced gastric cancer. Oncology. 1998;55:456–460. doi: 10.1159/000011895. [DOI] [PubMed] [Google Scholar]
- 53.Li XL, Wang YP, Wu DY, Zhang SM, Xin Y. Expression of 67Kda laminin receptor in human gastric cancer and its significance. Zhongguo Aizheng Yanjiu Jinzhan. 2000;5:130–134. [Google Scholar]