

Abstract
Background
In populations where mental health resources are scarce or unavailable, or where stigma prevents help-seeking, the Internet may be a way to identify and reach at-risk persons using self-report validated screening tools as well as to characterize individuals seeking health information online.
Aims
We examined the feasibility of delivering an Internet-based Chinese-language depression and suicide screener and described its users.
Method
An Internet-based depression and suicide screener was created and advertised primarily through Google AdWords. Participants completed a suicide and depression screening measure and received individualized feedback, which, if necessary, included the suggestion to seek additional mental health resources.
Results
In 7 months, 11,631 individuals visited the site; 4,709 provided valid information. Nearly half reported a current major depressive episode (MDE) and 18.3% a recent suicide attempt; however, over 75% reported never having sought help, including 77.7% of those with MDEs and 75.9% of those reporting a suicide attempt. As participants found the site by searching for depression information online, results may not generalize to the entire Chinese-speaking population.
Conclusion
Online screening can feasibly identify and reach many at-risk Chinese-speaking persons. It may provide resources to those with limited access to services or to those reluctant to seek such services.
Keywords: Online screening, cross-national, mental health services
A third of the world’s suicides occur in China (Hawton & van Heerigen, 2009; Phillips et al., 2002), although recent trends suggest that this might be decreasing over the past decade (Wang, Chan, & Yip, 2013). Depressive symptoms are a major risk factor for suicide attempts in the Chinese population (Phillips et al., 2002; World Health Organization [WHO], 2001). Although deaths from suicide are preventable with early identification and intervention, the timely identification of at-risk individuals is limited by a lack of mental health resources and stigma related to mental health.
In China, residents of rural areas, where resources are limited, have the highest suicide risk (Phillips et al., 2002). This situation is similar to the rest of the developing world: Over 75% of people worldwide with mental health problems are in resource-poor settings. In such settings, most do not receive care, largely due to poor infrastructure and few mental health resources, and this problem is unlikely to be solved by increasing the current or future supply of mental health professionals (Saxena, Thornicroft, Knapp, & Whiteford, 2007; WHO, 2004). Unfortunately, traditional delivery models are resource-intensive and may be prohibitively expensive to the majority of communities in rural areas and in the developing world overall.
Even when resources are present, there may be limited awareness of mental health problems (Bruffaerts et al., 2011). Mental health problems also carry significant social stigma in the Chinese culture, and are often associated with isolation, secrecy, and poor treatment adherence (Lee, Lee, Chiu, & Kleinman, 2005). This stigma can also lead to the internalization of stereotypes and low self-esteem, further exacerbating symptoms (Fung, Tsang, & Chan, 2010).
The Internet is a medium through which individuals can privately access resources that may not be supported by the local system, without consuming limited local resources (Muñoz, 2010). China has the largest number of Internet users in the world (Data Centre of China Internet, 2007; Internet World Stats, 2013), and Chinese is the second most common language online (Internet World Stats, 2013). Most Internet users are young persons, the target population identified by the WHO as at a heightened risk for suicide (WHO, 2001). The Internet and other social media can have a powerful influence on suicide behaviors of a population, either increasing (i.e., through pro-suicide information) or decreasing (i.e., through suicide prevention materials) suicide rates (Luxton, June, & Fairall, 2012).
The Internet can also be leveraged to deliver suicide and depression screening to the hundreds of millions of Chinese-literate individuals residing outside of China’s geographical borders, to help address the high rates of suicide in the immigrant populations (Bhugra, Desai, & Baldwin, 1999; Sue, Cheng, Ka, Saad, & Chu, 2012). Even outside of Asia, in the relatively affluent Western countries, Asian immigrant women attempt suicide more often than their Western counterparts (Bhugra et al., 1999). Suicide risk factors among Chinese individuals remain constant regardless of their country of residence (Lester, 1997). There is a steady flow of Chinese immigrating to other countries for work or study, and trends are reaching historic highs (Osnos, 2011). If these trends persist, Chinese-language resources will become increasingly necessary worldwide. The Internet offers a culturally appropriate medium that stays consistent regardless of country of residence. This can be important for Chinese immigrants, the majority of whom were born in China (Lai & Arguelles, 2003) and may lack fluency in host languages. Therefore, the ability to present materials in Chinese across geopolitical borders may be able to address a large and important need for suicide problems in this population.
Demonstration of the ability to assess the needs of suffering individuals through the Internet is a necessary first step to inform widespread dissemination and global uptake of online health resources. The utility of developing and delivering Chinese-language resources online depends on the ability to reach this population. Thus, the purpose of this investigation was to understand the feasibility of and interest in a Chinese-language web-based depression and suicide screener. We also discuss the prevalence of depression and suicide gathered by our online screener in relation to the national prevalence rates in China.
Method
An Internet-based study was conducted worldwide in Chinese. Consent was obtained over the Internet, as approved by the Institutional Review Board of the University of California, San Francisco.
Participants
Any Chinese-literate individual 18 years of age or older was able to take part in this study. During the 7 months of recruitment, 11,631 persons visited the website, and 6,013 provided minimum data to determine eligibility (382 were ineligible; mean age = 15.49 years, SD = 1.60, women: 65.8%). Of those eligible, nearly 90% (N = 4,980) provided enough data to screen for the presence or absence of major depression. Of these, 5.4% reported that their answers may not be accurate, and were excluded from analyses. The final sample for our study therefore comprised 4,709 individuals. Participants were 30.2 years old (SD = 9.63) on average, and 61.8% were women. Just over half (52.1%) reported being from mainland China; others were from Malaysia (14.5%), the US (13.3%), Hong Kong (3.4%), Australia (3.0%), Canada (2.3%), and other countries (11.4%).
Those who consented to provide additional information in the Demographics 2 questionnaire (N = 531) were mostly well educated, with 15.0 years (SD = 3.33) of education on average, and living in urban areas (91.9%). A sizable proportion reported being currently unemployed (40.3%); 7% reported being divorced. An overwhelming majority (89.3%) reported that they did not know of mental health resources where they lived.
Measures
The Demographics 1 questionnaire assessed participants’ age, gender, race, and country of residence.
The Demographics 2 questionnaire was administered only to participants consenting to take part in a follow-up study. This questionnaire asked about participants’ country of birth, number of people in the household, participants’ education, employment, marital status, income, and subjective social status, as assessed by the “social ladder” (Adler, Epel, Castallazzo, & Ickovics, 2000), where individuals rate their position in society relative to others. The questionnaire also asked about participants’ experience with treatment and their knowledge of the availability of mental health resources in their community.
The MDE Screener (Muñoz, 1998) is an 18-item measure designed to screen for the presence of current and past major depressive episodes (MDEs). It assesses the presence of nine symptoms of depression according to the Diagnostic and Statistical Manual, 4th ed. (DSM-IV; American Psychiatric Association, 1994) over a period of 2 weeks or more; it also assesses whether Criterion C (significant impairment in functioning) is met within the same time span. All participants were screened for current MDEs by reporting their symptoms over the past 2 weeks. Participants who consented to participate in the follow-up study were asked about symptoms occurring in any 2-week period during their lifetime, excluding the past 2 weeks (to identify a past MDE). The screener has good agreement with the PRIME-MD (Muñoz, McQuaid, Gonzalez, Dimas, & Rosales, 1999; Spitzer et al., 1994) and with clinician-administered diagnostic interviews (Vasquez, Muñoz, Blanco, & López, 2008). Suicide was assessed using the item on this measure that assesses suicide ideation and behavior, using the question: “In the past two weeks … have you attempted suicide?”
Procedure
Participants were recruited primarily via a worldwide Google AdWords campaign; some may also have found our website via organic search results, word of mouth, etc. For the Google AdWords recruitment, entering keyword terms in Chinese in the Google search engine such as those focused on depression, for example, “depression,” (i.e., “抑 漿症”) or “I am feeling sad” or “I am down” (i.e., “感瘷 心情低篃或悲伤”) on suicide, including “suicide” (i.e., “縖杀”) or “want to commit suicide” (i.e., “想縖杀”), and nonspecific related terms, such as “no hope” (i.e., “没有希望”) or “excessive pressure” (i.e., “压力瀹大”), triggered one of several ads for a “Free Online Depression Screener” (i.e., “免狇抑漿 症筛检樒卷”). Those clicking on the ad were taken to the landing page of the research website.
The landing page informed participants that the screener is part of a research study and offered information about the limits to confidentiality. All participants provided their age to determine eligibility; participants were also asked to provide their race, gender, and country of residence. Participants then completed the current MDE Screener. To identify invalid data, the MDE Screener was followed by the honesty question, which asked whether the participants’ responses are accurate or whether participants are simply testing the site; participants were assured that answering this question would not influence feedback or their ability to participate further. Only 271 participants reported that their answers were not accurate; their data were excluded from these analyses. Participants were then offered personalized feedback on their responses, containing a brief explanation of the individuals’ symptom level. Participants indicating a high symptom level (5+ symptoms) or meeting Criterion C (i.e., disability or impairment in functioning) were prompted to consult with a mental health professional, if available. Participants who reported any degree of suicidality (i.e., from thinking about death to making a suicide attempt) were offered additional feedback expressing concern and urging them to seek help by consulting with their provider or going to a hospital. To offer participants immediate safety resources, all pages contained a link to the Chinese page of Befrienders.org (http://www.befrienders.org/int/chinese/index.asp?PageURL=index.php), an international online database of suicide helplines available by telephone or email, and to a dedicated Chinese-language crisis support website (http://www.crisis.org.cn/).
Participants were then offered an opportunity to participate in a monthly follow-up rescreening study, for the next 12 months. Those consenting (N = 531) were asked to complete the Demographics 2 questionnaire, as well as the Lifetime portion of the MDE Screener, which assessed for a 2-week period of depressive symptoms at any point in their lifetime, excluding the past 2 weeks. As with the current MDE Screener, personalized feedback was provided on participants’ responses. Participants were then sent follow-up emails monthly for the next 12 months, inviting them to return to the site and re-screen their mood; the follow-up data are not discussed in this paper. The design of the site is illustrated graphically in Figure 1.
Figure 1.
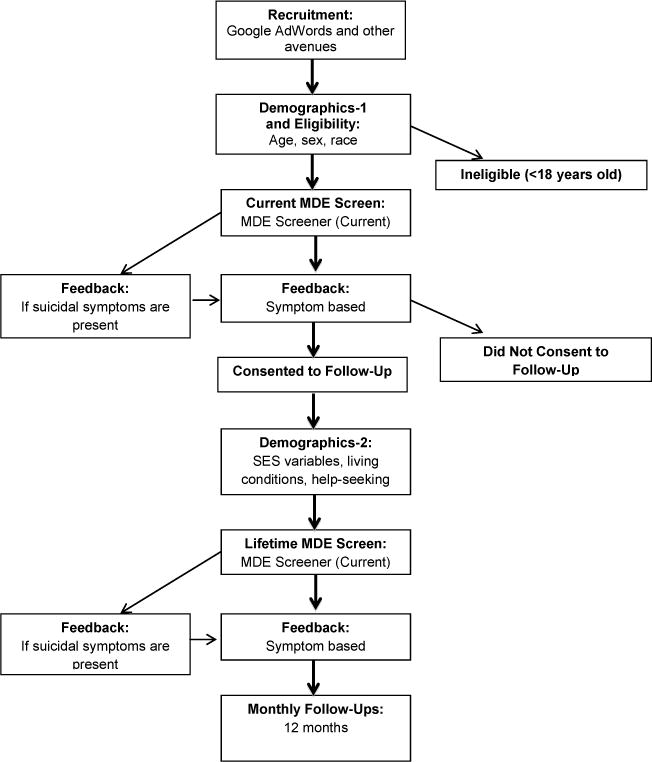
Design of the Mood Screener website.
Results
Depression
Of the 4,709 individuals who provided enough data to assess for a current MDE, 49.0% screened positive for a current MDE (of these, 47.2% were women). Demographic characteristics of those with and without MDEs are provided in Table 1.
Table 1.
Characteristics of 4,709 individuals (≥18 years) with and without current major depressive episode (MDE) and suicide attempts, suicidal ideation, disability, and lifetime rates of help-seeking behaviors for psychological problems
| MDE status | N | Demographics | Suicidality (%)d |
Disability (%)b |
Help-seeking behaviors (%)c |
|||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age (SD) years |
Female (%) |
Attempted suicidea |
Wanted to die |
Thought about suicide |
Never sought help |
Currently receiving medication |
Currently receiving therapy |
|||
| Current MDE | 2306 | 29.1 (8.89) | 59.5 | 24.7 | 57.7 | 63.2 | 100d | 77.7 | 16.0 | 12.9 |
| No current MDE | 2403 | 31.4 (10.17) | 63.9 | 12.1 | 28.7 | 32.8 | 27.6 | 84.8 | 1.0 | 0.6 |
Notes.
As measured by “suicide attempt or try.”
Disability was assessed using the question: “Did these problems interfere with your life or activities a lot?”
Collected as part of Demographics 2; current MDE group, N = 319, no current MDE group, N = 177.
Part of the MDE criteria.
Rates of suicide attempts as well as disability and lifetime rates of help-seeking behaviors for psychological problems are presented in Table 1. On the basis of the information from those who consented to a monthly re-screening study and provided additional information about help-seeking behaviors in the Demographics 2 questionnaire (n = 496), we found that MDE status did not distinguish help-seeking behaviors, with 77.7% of those with a current MDE and 84.8% of those without a current MDE reporting never seeking help, Fisher’s exact test, p = .061. However, those with a current MDE were more likely to be unemployed than those without a current MDE, Fisher’s exact test, p = .008. Not surprisingly, of those with a current MDE, 84.8% also endorsed a past MDE.
Suicide
Of those providing valid MDE data, virtually all participants (n = 4,690) answered the suicide item. Of these, 18.3% reported having attempted suicide in the past 2 weeks, with women being more likely to report an attempt than men, 20.3% vs. 15.0%, respectively, Fisher’s exact test, p = .000005. Those who reported a recent suicide attempt were younger on average than those reporting no recent suicide attempt, 28.0 (SD = 8.99) years old vs. 30.7 (SD = 9.68) years old, F(1, 4688) = 56.18, p < .001. Interestingly, only two thirds (66.2%) of suicide attempters screened positive for a current MDE.
Demographic characteristics and help-seeking behaviors of those with and without recent suicide attempt are provided in Table 2. Of the respondents who consented to a follow-up study and provided additional information about help-seeking and suicide information (n = 494) in Demographics 2, there was no significant difference between those with and without a suicide attempt in reporting ever seeking help, Fisher’s exact test, p = .18. A majority of those reporting a suicide attempt in the past 2 weeks (86.2%) reported that there were either no mental health resources available where they lived (35.3%) or they were unsure whether such resources existed (50.9%). Those who were unemployed were more likely to have made a suicide attempt compared with those in employment, 29.0% vs. 19.7%, respectively, Fisher’s exact test, p = .018.
Table 2.
Demographic characteristics of 4,690 individuals (≥ 18 years) reporting whether they did or did not make a suicide attempt in the past 2 weeks and with current major depressive episode (MDE), disability, and lifetime rates of help-seeking behaviors for psychological problems
| Suicide statusa | N | Demographics | MDE (%) | Disability (%) | Help-seeking behaviors (%)b | |||
|---|---|---|---|---|---|---|---|---|
| Age (SD) years | Female (%) | Never sought help | Current medication | Current therapy | ||||
| Suicide attempt | 856 | 28.0 (8.99) | 68.6 | 66.2 | 75.3 | 75.9 | 22.4 | 19.1 |
| No suicide attempt | 3834 | 30.7 (9.68) | 60.2 | 45.1 | 60.5 | 81.7 | 12.4 | 8.5 |
Notes.
As measured by “suicide attempt or try.”
Collected as part of Demographics 2; suicide attempt group, N = 116, no suicide attempt group, N = 378.
Discussion
This study reveals that online screening has the ability to identify and reach many Chinese-speaking persons at risk for suicide and depression. We were able to quickly recruit a sizable number of Chinese-literate Internet users, who were split almost equally between China and other countries, which demonstrates that such resources can reach the intended audience. Our sample also consisted of predominantly younger people, the target population of many suicide prevention programs (WHO, 2001).
Our participants endorsed an alarmingly high rate of suicide attempts (18.3%). The rate in the identical English-language screener was only 7.8% (Leykin, Muñoz, & Contreras, 2012). Worldwide, women are more likely to attempt suicide than men, which was also true in our sample; however, China is one of only a few countries in the world where the rate of suicide completion is higher in women than it is in men (He & Lester, 1997; Lester, 1997; Phillips, et al., 2002). Although we focused only on suicide attempts, the high reported rate suggests a troubling rate of completions as well.
Only 66.2% of those who reported a suicide attempt also met criteria for an MDE. Although 90% of persons who commit suicide in high-income countries meet criteria for a mental disorder at the time of death (Hawton & van Heerigen, 2009), only 63% did so in a nationally representative sample in China (Yang et al., 2005), and our results suggest a similar pattern for suicide attempters. Other studies focusing on subsamples have found that only 45% (Li, Phillips, Zhang, Xu, & Yang, 2008) to 48% of younger Chinese suicide completers had a mental disorder (Zhang, Xiao, & Zhou, 2010). We also found an overall lower base rate of MDEs in our sample (49.0%) compared with the 66% reported in an English-language version of the screener (Leykin et al., 2012).
As this was a naturalistic web-based study, it is possible that our sample may comprise a self-selected group of young individuals who were motivated enough to seek information about depression online, perhaps because of the presence of more severe depression symptoms. They may be more likely to seek information due to the lack of stigma associated with seeking help. If so, a simple web-based tool such as the one described here may be able to reach a higher-risk subgroup of the target population in an acute time of need.
Although there are various explanations for the low rate of MDEs in Chinese suicide completions and attempts, depressive symptoms nonetheless remain linearly associated with the risk of suicide (Phillips et al., 2007) and are therefore important to assess. Subthreshold symptoms may play a significant role in suicide attempts. In our study, of those who did not meet criteria for an MDE, nearly a third (32.8%) reported wanting to die. Over a quarter of our sample endorsed significant disability associated with depressive symptoms even though they did not meet criteria for an MDE. Future studies examining web-based screening of suicide may look at continuous measures of depressive symptoms to identify subthreshold significance or impact of symptoms on functioning rather than a dichotomous measure.
Over 75% of those who reported either a current MDE or suicide attempt reported never seeking treatment. Although alarming, this is regrettably consistent with other studies on help-seeking behaviors among the Chinese. Studies from the World Mental Health Survey found that only one third of persons in Taiwan with MDD sought help despite having twice the number of lost workdays compared with the US sample (Liao et al., 2012). Studies from mainland China show that 87.1% of those with mood disorders and moderate to severe disability never sought help and of those who did, only 6.7% ever saw a mental health professional (Phillips et al., 2009). A cross-cultural comparison revealed that among suicidal people in low- and middle-income countries who never received care, the most frequently cited reason for failure to seek treatment was low perceived need, followed by attitudinal barriers (e.g., wanting to handle the problem on their own) and structural barriers (e.g., limited financial resources, transportation, and availability of mental health resources) (Bruffaerts et al., 2011). Our study suggests that Chinese speakers are willing to seek mental health resources over the internet, which may help overcome these structural and attitudinal barriers (Erdman, Greist, Gustafason, Taves, & Klein, 1987; Levine, Ancil, & Roberts, 1989).
The finding that the vast majority – 90% of our participants – were not aware of other mental health resources is extremely troubling, and helps explain the willingness of these individuals to seek resources on the Internet. Indeed, given that our participants, by virtue of having access to the Internet, are likely more educated and affluent than the majority of Chinese speakers, the low rate of awareness of mental health resources in this population is as surprising as it is alarming, and likely points to even lower awareness and perhaps access to such resources of the rest of the population (e.g., Bruffaerts et al., 2011). This finding draws attention to the urgent need to develop and publicize mental health resources for Chinese speakers, and to do so in a variety of media, including the Internet, where individuals are already seeking such services.
A large majority of individuals who used our mood and suicide screener were unemployed. Other studies have also found a link between suicide risk and unemployment (Chen et al., 2013; Zisook et al., 2007). In Chinese populations, dysfunction, such as the inability to continue working, may be a more sensitive indicator of depression rather than distress, as distress may not be sufficient for determining depression, particularly considering issues of translation, cultural adaptation, and online delivery; detailed assessment of functioning might provide additional information about mood symptoms (Phillips, 2009). Studies from China show that nearly 40% of those with mood disorders also report moderate to severe disability from the mood disorder (Phillips et al., 2009).
Limitations
Our study used ads delivered via the Google search engine to recruit participants. Although Google remains the world’s largest search engine, it has relatively limited penetration in China (Levy, 2011) as compared with Baidu, China’s dominant search engine (Bonfils, 2013). Although over half of our sample (52.1%) nonetheless came from mainland China, our results may generalize only to individuals choosing to use an alternative search engine in preference to Baidu.
This was a naturalistic (nonrandomized) study, which may have resulted in a self-selection bias, thus, our findings are not meant to generalize to the entire population of Chinese individuals. However, our results should be representative of individuals seeking depression information over the Internet, and our data suggest that Chinese-speaking individuals are interested in online mental health resources. It is possible that the 2-week criterion for symptom assessment might have been overlooked, which may have contributed to the high rate of suicide attempts in the past 2 weeks; however, even if the numbers are accurate for a longer temporal duration, they remain highly concerning.
Conclusion
Suicide is a preventable cause of death. Our results indicate that the Internet is a feasible tool for accessing Chinese-literate populations who endorse high rates of suicide and depression, and is a good way to gather reliable data from these individuals. Our results appear consistent with a larger body of literature on the high rate of attempts and low rate of MDEs in the larger Chinese populations, as well as its role in suicide completion and attempts.
Suicide rates are known to fluctuate in response to social change (Sartorius, 1995) and ongoing drastic social change may play a unique role in the suicide and depression rate among Chinese individuals (Phillips, Liu, & Zhang, 1999). The most recent prevalence data do appear to suggest a decrease in the Chinese suicide rate over time (Wang et al., 2013). Nearly half of our sample was from mainland China and there is evidence that considerable social change is occurring in this country: the country’s average income has grown faster than anywhere else in the world (Hu, Hu, & Chang, 2003); concurrently, there has also been a sizable increase in income inequality (Sen, 2006), and more and more Chinese are emigrating to other countries (Osnos, 2012). One unique advantage of Internet-based resources is their plasticity and flexibility. The Internet can be used to deliver mental health resources despite the regional diversity of mainland China (e.g., providing self-help videos in various Chinese dialects); it can also be used to reach the immigrant Chinese-literate populations who reside in countries outside of China.
Our website was programmed to provide individualized feedback to users’ responses; however, the alarmingly high rates of suicide attempts endorsed by our sample reveal a need for the development of further resources, such as digital interventions that can teach coping skills, problem-solving, emotion regulation, or other strategies aimed at managing distress and dysfunction. These might be delivered over the Internet or over mobile phones and could be specifically designed for populations in areas of limited resources (Howitt et al., 2012) and be available free of charge (Muñoz, 2010). Recent innovations in this line of research demonstrate that online cognitive-behavioral-based self-help can effectively reduce the frequency and intensity of suicidal thoughts and is cost effective (Spijker, Majo, Smit, van Straten, & Kerkhof, 2012; Spijker, van Straten, & Kerkhof, 2010) and this appears to be a burgeoning area in suicide prevention (Mishara & Kerkhof, 2013). As Chinese-literate populations migrate to other countries, the Internet provides a powerful medium through which Chinese-language resources can be made available regardless of the place of residence (Lester, 1997). Currently, Chinese-language mental health resources on the Internet are sparse and these results could inform the development of an intervention geared specifically at this population. Online screening, treatment, and prevention efforts may have the potential to serve many currently untreated clinically depressed and suicidal individuals.
Biographies
Nancy Liu is currently a research specialist at the University of California, San Francisco, and Assistant Adjunct Professor at the University of San Francisco. Her clinical research expertise is in underserved populations, with a focus on suicide and depression. A former Fulbright Fellow and Fogarty Scholar, she has conducted research in China and Argentina.
Omar Contreras is a research associate and a web developer at the University of California, San Francisco, and the University of California at Berkeley. He has contributed, as the lead developer, to several multilingual Internet interventions and other Internet resources focused on depression.
Ricardo F. Muñoz is Distinguished Professor of Clinical Psychology at Palo Alto University and Professor of Psychology Emeritus, University of California, San Francisco. He is Founding Director of the Institute for International Internet Interventions for Health and does research in Spanish and English on depression prevention and smoking cessation.
Yan Leykin is an assistant professor in the Department of Psychiatry at the University of California, San Francisco. His research focuses on the development of Internet-based interventions for symptoms of depression and of other related resources for individuals with depression; he also studies decision making of depressed individuals.
References
- Adler NE, Epel E, Castallazzo G, Ickovics J. Relationship of subjective and objective social status with psychological and physiological functioning in preliminary data in healthy white women. Health Psychology. 2000;19:586–592. doi: 10.1037//0278-6133.19.6.586. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th. Washington, DC: Author; 1994. [Google Scholar]
- Bhugra D, Desai M, Baldwin DS. Attempted suicide in west London, I: rates across ethnic communities. Psychological Medicine. 1999;29:1125–1130. doi: 10.1017/s0033291799008910. [DOI] [PubMed] [Google Scholar]
- Bonfils M. Yandex just passed Bing to become 4th largest global search engine. Search Engine Watch. 2013 May; Retrieved from http://searchenginewatch.com/article/2242374/Yandex-Just-Passed-Bing-to-Become-4th-Largest-Global-Search-Engine.
- Bruffaerts R, Demyttenaere K, Hwang I, Chiu WT, Sampson N, Kessler RC, Nock M. Cross-cultural attitudes to help-seeking among individuals who are suicidal: New perspective for policy-makers. British Journal of Psychiatry. 2011;199:8–10. doi: 10.1192/bjp.bp.110.087817. [DOI] [PubMed] [Google Scholar]
- Chen L, Liu YH, Zheng QW, Xiang YT, Duan YP, Yang FD, Si TM. Suicide risk in major affective disorder: Results from a national survey in China. Journal of Affective Disorders. 2013 doi: 10.1016/j.jad.2013.10.046. [DOI] [PubMed] [Google Scholar]
- Data Centre of China Internet. 2007–2008 China Internet Survey Report. 2008 Jan 8; [in Chinese]. Retrieved from http://www.dcci.com.cn/list/research.shtml.
- Erdman HP, Greist JH, Gustafson DH, Taves JE, Klein MH. Suicide risk prediction by computer interview: a prospective study. Journal of Clinical Psychiatry. 1987;48:464–467. [PubMed] [Google Scholar]
- Fung K, Tsang H, Chan F. Self-stigma, stages of change and psychosocial treatment adherence among Chinese people with schizophrenia: A path analysis. Social Psychiatry and Psychiatric Epidemiology. 2010;45:561–568. doi: 10.1007/s00127-009-0098-1. [DOI] [PubMed] [Google Scholar]
- Hawton K, van Heerigen K. Suicide. Lancet. 2009;373:1372–1381. doi: 10.1016/S0140-6736(09)60372-X. [DOI] [PubMed] [Google Scholar]
- He ZX, Lester D. The gender difference in Chinese suicide rates. Archives of Suicide Research. 1997;3:81–89. [Google Scholar]
- Howitt P, Darzi A, Yang GZ, Ashrafian H, Atun R, Bar-low J, Wilson E. Technologies for global health. Lancet. 2012;380:507–535. doi: 10.1016/S0140-6736(12)61127-1. [DOI] [PubMed] [Google Scholar]
- Hu A, Hu LL, Chang ZX. China’s economic growth and poverty reduction (1978–2002) 2003 Retrieved from http://www.imf.org/external/np/apd/seminars/2003/newdelhi/angang.pdf.
- Internet World Stats. Internet world users by language: Top 10 languages. 2013 Retrieved from http://www.internetworldstats.com/stats7.htm.
- Lai EYP, Arguelles D. The new face of Asian Pacific America: Numbers, diversity & change in the 21st century. San Francisco, CA: Asian American Studies Center Press; 2003. [Google Scholar]
- Lee S, Lee M, Chiu M, Kleinman A. Experience of social stigma by people with schizophrenia in Hong Kong. British Journal of Psychiatry. 2005;186:153–157. doi: 10.1192/bjp.186.2.153. [DOI] [PubMed] [Google Scholar]
- Lester D. Suicide in American: a nation of immigrants. Suicide and Life-Threatening Behavior. 1997;27:50–59. [PubMed] [Google Scholar]
- Levine S, Ancill RJ, Roberts AP. Assessment of suicide risk by computer-delivered self-rating questionnaire: Preliminary findings. Acta Psychiatrica Scandinavica. 1989;80:216–220. doi: 10.1111/j.1600-0447.1989.tb01330.x. [DOI] [PubMed] [Google Scholar]
- Levy S. Inside Google’s China misfortune. Fortune. 2011 Apr 15; Retrieved from http://tech.fortune.cnn.com/2011/04/15/googlesordeal-in-china/
- Leykin Y, Muñoz RF, Contreras O. Are consumers of internet health information “cyberchondriacs”? Characteristics of 24, 965 users of a depression screening site. Depression and Anxiety. 2012;29:71–77. doi: 10.1002/da.20848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li XY, Phillips MR, Zhang YP, Xu D, Yang GH. Risk factors for suicide in China’s youth: A case-control study. Psychological Medicine. 2008;38:397–406. doi: 10.1017/S0033291707001407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liao SC, Chen WJ, Lee MB, Lung FW, Lai TJ, Liu CY, Chen CC. Low prevalence of major depressive disorder in Taiwanese adults: possible explanations and implications. Psychological Medicine. 2012;42:1227–1237. doi: 10.1017/S0033291711002364. [DOI] [PubMed] [Google Scholar]
- Luxton DD, June JD, Fairall JM. Social media and suicide: A public health perspective. American Journal of Public Health. 2012;102:S195–S200. doi: 10.2105/AJPH.2011.300608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mishara B, Kerkhof A. Suicide prevention and new technologies. Basingstoke, UK: Palgrave Macmillan; 2013. [Google Scholar]
- Muñoz RF. The Major Depression Episode (MDE) screener. 1998 Retrieved from http://www.medschool.ucsf.edu/latino/manuals.aspxm.
- Muñoz RF. Using evidence-based internet interventions to reduce health disparities worldwide. Journal of Medical Internet Research. 2010;12:e60. doi: 10.2196/jmir.1463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muñoz RF, McQuaid JR, Gonzalez GM, Dimas J, Rosales VA. Depression screening in a women’s clinic: Using automated Spanish-and English-language voice recognition. Journal of Consulting and Clinical Psychology. 1999;67:502–510. doi: 10.1037//0022-006x.67.4.502. [DOI] [PubMed] [Google Scholar]
- Osnos E. The Chinese navy, Zambian copper and Libya. The New Yorker. 2011 Feb 28; Retrieved from http://www.newyorker.com/online/blogs/evanosnos/2011/02/china-zam-bia-libya.html.
- Phillips MR. Is distress a symptom of mental disorders, a marker of impairment, both or neither? World Psychiatry. 2009;8:91–92. [PMC free article] [PubMed] [Google Scholar]
- Phillips MR, Liu H, Zhang Y. Suicide and social change in China. Culture, Medicine, & Psychiatry. 1999;23:25–50. doi: 10.1023/a:1005462530658. [DOI] [PubMed] [Google Scholar]
- Phillips MR, Shen Q, Liu X, Pritzker S, Streiner D, Conner K, Yang G. Assessing depressive symptoms in persons who die of suicide in mainland China. Journal of Affective Disorders. 2007;98:73–82. doi: 10.1016/j.jad.2006.07.020. [DOI] [PubMed] [Google Scholar]
- Phillips MR, Yang GH, Zhang YP, Wang LJ, Ji HY, Zhou M. Risk factors for suicide in China: A national case-control psychological autopsy study. Lancet. 2002;360:1728–1736. doi: 10.1016/S0140-6736(02)11681-3. [DOI] [PubMed] [Google Scholar]
- Phillips MR, Zhang JX, Shi QC, Song ZQ, Ding ZJ, Pang ST, Wang ZQ. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001–05: An epidemiological survey. Lancet. 2009;373:2041–2053. doi: 10.1016/S0140-6736(09)60660-7. [DOI] [PubMed] [Google Scholar]
- Sartorius N. Recent changes in suicide rates in selected Eastern European and other European countries. International Psychogeriatrics. 1995;7:301–308. doi: 10.1017/s1041610295002055. [DOI] [PubMed] [Google Scholar]
- Saxena S, Thornicroft G, Knapp M, Whiteford H. Resources for mental health: Scarcity, inequity, and inefficiency. Lancet. 2007;370:878–889. doi: 10.1016/S0140-6736(07)61239-2. [DOI] [PubMed] [Google Scholar]
- Sen A. Conceptualizing and measuring poverty. In: Grusky DB, Kanbur R, editors. Poverty and inequality. Stanford, CA: Stanford University Press; 2006. pp. 30–40. [Google Scholar]
- Spijker BAJ, Majo CM, Smit F, van Straten A, Kerkhof AJFM. Reducing suicidal ideation: Cost-effectiveness analysis of a randomized controlled trial of unguided web-based self-help. Journal of Medical Internet Research. 2010;14:e141. doi: 10.2196/jmir.1966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spijker BAJ, van Straten A, Kerkhof AJFM. The effectiveness of a web-based self-help intervention to reduce suicidal thoughts: A randomized controlled trial. Trials. 2010;11:25. doi: 10.1186/1745-6215-11-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spitzer RL, Williams JB, Kroenke K, Linzer M, deGruy FV, Hahn SR, Johnson JG. Utility of a new procedure for diagnosing mental disorders in primary care. The PRIME-MD 1000 study. Journal of the American Medical Association. 1994;272:1749–1756. [PubMed] [Google Scholar]
- Sue S, Cheng Y, Ka J, Saad CS, Chu JP. Asian American mental health: A call to action. American Psychologist. 2012;67:532–544. doi: 10.1037/a0028900. [DOI] [PubMed] [Google Scholar]
- Vázquez FL, Muñoz RF, Blanco V, López M. Validation of Muñoz’s mood screener in a nonclinical Spanish population. European Journal of Psychological Assessment. 2008;24:57–64. [Google Scholar]
- Wang CW, Chan CLW, Yip PSF. Suicide rates in China from 2002 to 2011: An update. Social Psychiatry and Psychiatric Epidemiology. 2013 doi: 10.1007/s00127-013-0789-5. Advance online publication. [DOI] [PubMed] [Google Scholar]
- World Health Organization. The World Health Report: Mental health: New understanding, new hope. Geneva, Switzerland: World Health Organization; 2001. [Google Scholar]
- World Health Organization. World Mental Health Survey Consortium. Prevalence, severity, and unmet need for treatment of mental health disorders in the World Health Organization World Mental Health surveys. Journal of the American Medical Association. 2004;291:2581–2590. doi: 10.1001/jama.291.21.2581. [DOI] [PubMed] [Google Scholar]
- Yang GH, Phillips MR, Zhou MG, Wang LJ, Zhang YP, Xu D. Understanding the unique characteristics of suicide in China: National psychological autopsy study. Biomedical and Environmental Sciences. 2005;18:379–389. [PubMed] [Google Scholar]
- Zhang J, Xiao S, Zhou L. Mental disorders and suicide among young rural Chinese: A case-control psychological autopsy study. American Journal of Psychiatry. 2010;167:773–781. doi: 10.1176/appi.ajp.2010.09101476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zisook S, Lesser I, Stewart JW, Wisniewski SR, Balasubramani GK, Fava M, Rush AJ. Effect of age at onset on the course of major depressive disorder. American Journal of Psychiatry. 2007;164:1539–1546. doi: 10.1176/appi.ajp.2007.06101757. [DOI] [PubMed] [Google Scholar]