

Abstract
The present study was a random-effects model meta-analysis of 26 studies published between 1990 and 2010 (k = 32; n = 39,777) that (a) examined the association between acculturation and cigarette smoking in Hispanic women and (b) evaluated age, national origin, and measure and dimensionality (unidimensional vs. bidimensional) of acculturation as moderating variables. Results indicate a strong positive relationship and suggest larger effects of acculturation on cigarette smoking in women of Mexican descent as compared with women originating from other Latin American countries for current and lifetime smoking, as well as smoking overall. The effect of acculturation on cigarette smoking was larger in adults as compared with adolescents for current smoking and smoking overall. Few differences in effect size by measure or dimensionality of acculturation emerged. Results are discussed with regard to implications for future research and the measurement of acculturation.
Keywords: Acculturation, Hispanic, Smoking, Meta-Analysis
Every year in the United States, approximately 184,015 women die from diseases related to cigarette smoking (CDC, 2013c). Smoking is the leading preventable cause of death in the United States and is responsible for 80% of lung cancer deaths and 90% of deaths related to chronic obstructive pulmonary disease (COPD) in women (CDC, 2013b). National data indicate that 16.5% of U.S. women smoke, but that Hispanic women report much lower rates of smoking (8.6% in 2011; CDC, 2013a). However, smoking prevalence among Hispanic women varies greatly by national origin. Women from Central or South America are least likely to report smoking, and women from Puerto Rico report higher rates of smoking than those of non-Hispanic Whites (American Lung Association, 2010; Caraballo, Yee, Gfroerer, & Mizra, 2008; CDC, 2013a).
One issue of particular importance when examining cigarette smoking in Hispanics is acculturation. 1 Acculturation generally refers to the process of adaptation and (a) involves the values, practices, and cultural identity associated with both an individual’s heritage culture and the receiving culture (e.g., United States), and (b) relates to the degree to which the heritage culture is maintained and the extent to which the receiving culture is adopted (Cabassa, 2003; Sam & Berry, 2010; Schwartz, Unger, Zamboanga, & Szapocznik, 2010). Acculturation has been linked to both perceived discrimination and stress, with factors such as family conflict and lack of shared family values and cohesion increasing the risk for smoking (Lorenzo-Blanco & Cortina, 2013; Torres, Driscoll & Voell, 2012). Indeed, research indicates a significant positive relationship between acculturation and smoking in the Hispanic population overall (Abriado-Lanza, Chao, & Florez, 2005; Kimbro, 2009). A recent study concluded that, although foreign-born Hispanic women report low rates of smoking, U.S. born Hispanic women report much higher rates of smoking – which suggests that the levels of smoking-related morbidity and mortality among Hispanic women as a group will only increase (Lariscy, Hummer, Rath, Villanti, Hayward, & Vallone, 2013). A clear understanding of the relationship between acculturation and smoking in Hispanic women, particularly the factors which serve to mediate and moderate it, is important if we are to develop acculturation-based interventions that prevent or reduce smoking in Hispanic women.
Despite the general trend toward a positive relation between acculturation and smoking, a small number of studies have also produced null results (e.g., Balcazar, Castro, & Krull, 1995; Samet, Howard, Coultas, & Skipper, 1992), and other research has found that age and national origin may moderate the relationship between smoking and acculturation in Hispanic women (Kaplan, Nápoles-Springer, Stewart, & Pérez-Stable, 2001; Perez-Stable et al., 2001; Wilkinson et al., 2005). Taken together with results from the 2008 National Health Interview Survey (American Lung Association, 2010)—which indicate that among Hispanics, U.S.-born Mexicans reported smoking at a rate second only to all Cubans regardless of nativity—these findings collectively suggest that the relationship between acculturation and cigarette smoking in Hispanics may be complex and multifaceted. Indeed, this relationship could reflect the influence of not only demographic factors, but also variations in factors that are related to migration and individual and social resources (Castro, 2013).
To add to this complexity, research also suggests that (a) smoking in Hispanic women may be related to certain cultural domains of acculturation (e.g., cultural practices such as language use; cultural values) but not others, and (b) that differences may exist in how individual domains affect patterns of use. For example, Kaplan et al. (2001) found that although linguistic acculturation (preference for English), less-traditional family values, and less-traditional beliefs about women’s roles in the family were positively related to smoking experimentation, only linguistic acculturation was related to regular smoking. These findings are particularly important given inconsistencies in the way acculturation has been measured in the extant literature (Thomson & Hoffman-Goetz, 2009). For example, many studies have used a single proxy variable (e.g., language spoken at home) to measure acculturation, while others have used composite measures or validated scales (e.g., Acculturation Rating Scale for Mexican Americans [ARSMA]; Cuellar et al., 1980). With the exception of language, which falls under the heading of cultural practices, the most commonly used proxy variables (e.g., nativity, length of time in the United States) in the literature related to smoking are demographic markers. Although some demographic markers (e.g., nativity) may be related to adoption of cultural practices, the validity of other proxies – such as years spent in the United States – is likely dependent upon the community in which one has settled (Schwartz, Pantin, Sullivan, Prado, & Szapocznik, 2006). Thus, in the case of studies that utilize composite measures and operationalize acculturation as the sum of multiple proxy variables, 2 there is no guarantee that the set of proxy variables is more valid than a single proxy would have been (especially if the proxies in the composite are unrelated to each other or work in opposing directions). In addition, the use of multiple measures does not ensure that multiple cultural domains are assessed. Lastly, even among those studies that utilize validated scales, such scales may lack consistency, as variations exist with regard to the content and assessment of multiple cultural domains (Wallace, Pomery, Latimer, Martinez, & Salovey, 2010).
In addition to differences in the type of measure used and cultural domains assessed, acculturation research also varies with regard to how acculturation is conceptualized. Some studies both conceptualize and measure (e.g., using proxies such as language and immigrant generation) acculturation unidimensionally, where greater acquisition of U.S. culture implies loss of Hispanic culture. Other studies conceptualize acculturation as consisting of separate dimensions for Hispanic and U.S. acculturation, and utilize bidimensional scales (e.g., Acculturation Rating Scale for Mexican Americans-II; Cuellar, Arnold, & Maldonado, 1995) to index these dimensions (see Schwartz et al., 2010 for a comprehensive overview of acculturation) 3.
Although it is clear that a relationship exists between acculturation and smoking in Hispanic women, more research is needed to better understand the strength of this relationship and the factors that may moderate it. Meta-analysis may be a useful way to synthesize existing research where different conceptual models and measurement approaches have been used (e.g., Barger & Gallo, 2008; Kasirye et al., 2005). Accordingly, the primary purpose of the present meta-analysis was to synthesize the current literature and to quantify the association between acculturation and cigarette smoking in Hispanic women. In addition, secondary aims included (a) assessing the impact of potential moderating variables such as age and country of origin, and (b) examining whether acculturation is more closely related to certain patterns of smoking. Finally, given the inconsistencies in the measurement of acculturation, we examined the extent to which findings in the current literature are moderated by the measure (and conceptualization) of acculturation used. The PICOTS table is provided in Appendix A.
Method
Literature Search
We conducted a comprehensive search of the literature examining acculturation and smoking between January, 1990 and Decemer, 2010 in March of 2011. To ensure an exhaustive search of relevant studies, a three-step process was used. Studies were initially identified via a computerized search of electronic databases, including EBSCOhost, PsycINFO, PubMed, and Web of Science, using the following key words in various combinations: acculturation, Hispanic, Latino, Latina, Mexican, Cuban, Puerto Rican, Central American, South American, women, and smoking (see Appendix B for the PubMed search strategy). Next, using the same date range and key word combinations, the electronic databases, Dissertations & Theses (ProQuest), and WorldCat Dissertations and Theses were searched in an effort to include both published and unpublished studies and to reduce publication bias. Finally, the reference lists of studies obtained from the computerized searches were examined to locate additional relevant studies, as were the reference lists from Chun, Organista and Marín’s (2003) edited book on acculturation.
All empirical studies examining the relationship between acculturation and smoking in the U.S. Hispanic population spanning the years between 1990 through 2010 were initially considered. The following criteria were used for inclusion in the meta-analysis: (a) statistical analyses evaluating the association between smoking and acculturation in women were provided; and (b) statistical information was provided in a form from which an effect size could be extracted, and studies were evaluated for inclusion by the primary author, with a subset of 50 articles re-evaluated two weeks after initial coding (k = 0.88, 95% CI [0.71, 1]; Lipsey & Wilson, 2001). In an effort to include all relevant studies, we attempted to contact the authors of studies for which the statistical information necessary for inclusion was not available.
Data Extraction and Coding
A comprehensive coding sheet was designed for data extraction and coding. Coded data included variables such as sample size, age, SES, ethnicity, acculturation measure, psychometric properties of acculturation measure, type of smoking outcome, psychometric properties of the smoking measure, type of statistical analysis used, and test statistic reported. Studies separating their sample by groupings of interest (e.g., national origin) were coded so that each reported sample was entered as independent. This allowed us to avoid violating the assumption of statistical independence and to allow for moderator comparison (Lipsey & Wilson, 2001). All studies were coded according to the first author, and coding reliability was evaluated through the re-coding of a sub-sample of 13 studies six weeks after they were initially coding (k = 0.89, 95% CI [0.80, 0.99]; Lipsey & Wilson, 2001).
Statistical Analysis
The present meta-analysis utilized a random effects model to calculate weighted mean effect sizes. Such a method considers both within-study and between-study variability. Considering both sources of variability is essential given the wide array of acculturation measures utilized in current research, as well as the heterogeneity inherent in many Hispanic samples. The natural log of the odds ratio (lnOR) was used as the common effect size for analysis, with odds ratios (OR) s reported and all other forms of study level effect sizes (e.g., d, r) converted to odds ratios (Borenstein, Hedges, Higgins, & Rothstein, 2009; Lipsey & Wilson, 2001). Odds ratios are widely accepted as an effect size index for dichotomous outcomes (i.e., where most smoking studies index smoking as a yes/no variable), and 2x2 tables are expressed as cell frequencies as indicated by a, b, c, d or proportions of each group in each status as indicated by Pa, Pb, Pc, Pd, with OR = ad/bc = Pa(1-Pc)/Pc(1-Pa) (Lipsey & Wilson, 2001). Fleiss and Berlin (2009) note that odds ratios are “recommended as the measure of choice for measuring effect or association when the studies contributing to the research synthesis are summarized by fourfold tables” (p. 250).
A 95% confidence interval was created for each odds ratio, and effect sizes from each study were weighted by their inverse variance weight (i.e., the reciprocal of the standard error squared). Such a strategy increases representativeness by attributing more weight to studies with larger sample sizes under the assumption that the effect sizes yielded from such studies will be more precise and will better represent the true effect (Borenstein et al., 2009; Lipsey & Wilson, 2001). Heterogeneity of variance was evaluated both visually using forest plots and statistically using the Q statistic, which is distributed as a chi-square, with degrees of freedom equaling k – 1, and Q – df equaling the excess variance. Statistical significance is interpreted using an associated p-value, with a significant Q value indicating heterogeneity across studies (Bruce, Pope, & Stanistreet, 2008).
Publication bias was assessed using a variety of methods. The presence of bias was assessed visually using funnel plots to inspect the distribution of effect sizes (Borenstein et al., 2009) and statistically using Egger’s regression intercept, which tests the funnel plots for asymmetry. Egger’s regression intercept tests the null hypothesis that the Y intercept = 0 by regressing the standard normal deviate against precision (the inverse of the standard error); larger deviations from zero indicate greater asymmetry (Egger, Smith, Schneider, & Minder, 1997). The robustness of the effect of publication bias was assessed through the computation of Orwin’s fail safe Ns, which provide the additional studies necessary to reduce the mean effect size to nonsignificance (Borenstein et al., 2009; Sutton, 2009). Finally, Duval and Tweedie’s trim and fill procedure was used to assess the impact of publication bias and to identify an estimate of an unbiased mean effect (Borenstein et al., 2009; Sutton, 2009).
Standard conventions were used as guidelines for the interpretation of mean effect sizes, with ORs of 1.5 interpreted as small in magnitude, 2.5 as medium, and 4.3 as large (Cohen, 1988; Rossi, 2013). However, published effect sizes commonly seen in acculturation research and research related to smoking outcomes were also considered. Rossi (2013) examined thirteen meta-analyses related to health behavior change interventions and found a small mean effect size of d = 0.207 [95% CI = 0.175, 0.239], or the equivalent of OR = 1.5. Based on these findings, he recommends that Cohen’s (1988) conventions be adjusted downward to ORs of 1.31, 1.44, and 1.57, for small, medium, and large effect sizes.
To assess the significance of age, national origin, and acculturation measure as moderating variables, effect size magnitudes and confidence intervals were compared using an analog to the analysis of variance (ANOVA), which tests how much variance a categorical variable explains in terms of differences between effect sizes. The Q statistic (an index of heterogeneity) is divided into within pooled group variance (QW; sampling error) and between group variance (QB) statistics, with a p value indicating that the variability between effect sizes is significantly greater than sampling error alone and can therefore be attributed to the moderating effect of the categorical variable examined. One comparison of interest – acculturation reported as dichotomous “low” vs. “high” categories (e.g., English vs. Spanish speakers) vs. the addition of a “middle” category (e.g., English vs. English and Spanish vs. Spanish speakers) – violated the assumption of statistical independence due to multiple comparisons per dataset. As a result, inferences were made through a manual examination of effect sizes and confidence intervals (Borenstein, 2009; Lipsey & Wilson, 2001).
Results
Study Inclusion
A total of 314 studies on smoking and acculturation in Hispanic women were selected for initial review. A manual examination of titles and abstracts resulted in the exclusion of 195 studies, with the remaining 119 designated for full text review. We were unable to retrieve 13 of these 119 studies (12 of which were dissertations) despite using several retrieval methods: electronic databases, interlibrary loan, a hard copy search of local libraries, and attempts to contact the authors. The remaining 106 studies were obtained for thorough inspection. Based on inclusion/exclusion criteria, 80 studies were excluded, with 26 studies remaining for analysis (see Figure 1). One study (Peterson et al., 1998), which utilized data from the Arizona Perinatal Acculturation Project, was eliminated from the analysis because another study included in the review [Balcazar et al. (1996)] reported results using the same dataset.
Figure 1.
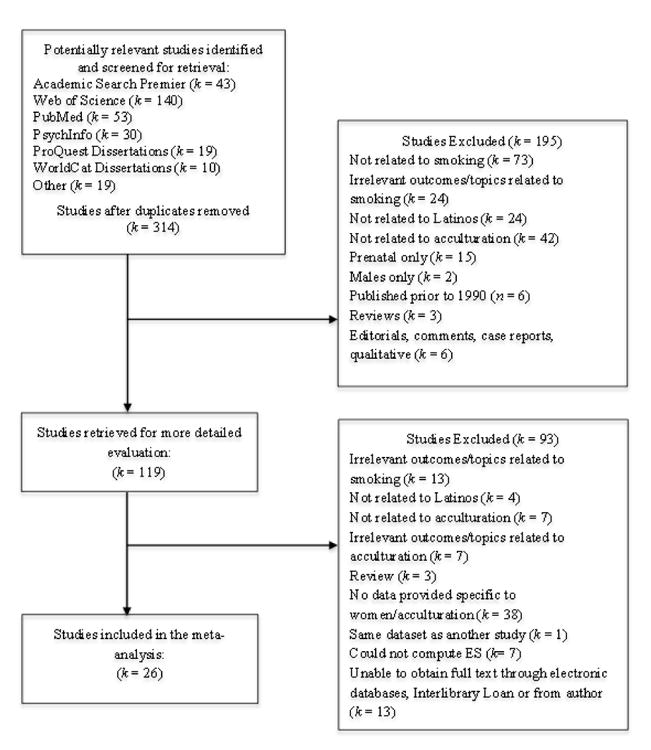
Flow chart of paper selection and exclusion process.
Study Characteristics
The 26 studies included in the meta-analysis indexed acculturation in a variety of ways, including proxy variables such as language, nativity, length of time in the United States, and self-identification as either Mexican or Mexican American. Six studies utilized composite variables and eight used validated scales, including the Short Acculturation Scale for Hispanics (Marin et al., 1987), the General Acculturation Index (Balcazar et al., 1995), the Acculturation Rating Scale for Mexican Americans (Cuellar et al., 1980), and the Acculturation Rating Scale for Mexican Americans-II (Cuellar, Arnold, & Maldonado, 1995). All but two studies conceptualized and measured acculturation as unidimensional, with ten studies assessing acculturation using a proxy variable.4 Smoking outcomes were primarily measured using self-report of lifetime smoking and/or current smoking within a specified time frame ranging from a week to a year (a number of studies employed an inclusion criterion of having smoked at least 100 cigarettes in one’s lifetime). Many of the studies reported results for multiple outcomes (i.e., current smoking and lifetime/ever having smoked), and in these cases, the mean of the effect size was taken to represent the effect of acculturation in the overall analysis (see Table 1).
Table 1. Characteristics of Studies Included in the Meta-Analysis.
| Study | Sample Size and Ethnicity | Age Group | SES | Participant Source | Acculturation Measure | Smoking Measure |
|---|---|---|---|---|---|---|
| Abraido-Lanza et al. (2005) | 1787 Hispanic | Adults | Low acculturated income M = 15-16KHigh acculturated income M = 19K | 1991 National Health Interview Survey | Nativity and length of time in the U.S. dichotomized into high and low | Current smokers have smoked 100 cigarettes in their lifetime and either smoke every day or some days |
| Balcazar et al. (1995) | 571 Hispanic, 91% Mexican | Adult | N/A | Companeros de la Salud study | GAI (1.0-2.39 was considered low acculturation, and 2.4-5.0 higher acculturation) | Self report of ever having smoked |
| Balcazar et al. (1996) | 141 Mexican | Adoles. and Adults | Low income | Arizona Perinatal Acculturation Project | 5 item scale: (1) language participant speaks better, (2) language participant writes better, (3) country where childhood was spent, (4) current circle of friends, & (5) pride in having a Latino/Hispanic background | Self report of smoking in the last 12 months |
| Barger & Gallo (2008) | 5118 Mexican | Adults | Estimates included male participants | 2000 & 2002 National Health Interview Survey | Self identification as either Mexican or Mexican American, nativity, interview language | Self report of current smoking |
| Cantero et al. (1999) | 573 Hispanic | Adults | Low income | Public housing projects in Los Angeles | 11 items from ARSMA | Self report of current and ever smoking |
| Coonrod et al. (1999) | 76 Mexican | Adults | Low income | Maricopa Medical Center in Phoenix, AZ | GAI (1.0-3 was considered low acculturation, and 3.1-5.0 higher acculturation), nativity, length of time in the U.S. (0-5 = low, >5 = high) | Self report of ever smoking (smoking more than 5 packs/lifetime) and current smoking (within 7 days) |
| Corral & Landrine (2008) | 3700 Mexican | Adults | Estimates included male participants | 2001 California Health Interview Survey | Nativity and language spoken at home | Self report of current smoking |
| Dusenbery & Epstein (1994) | 1627 Hispanic | Adoles. | N/A | 47 public and Catholic middle schools in NYC with 25% or more Hispanic/Latino students | 5-point scale of language spoken at home categorized into English, bilingual and Spanish | 11-point scale of smoking frequency ranging from never smoked to a pack +/day, dichotomized. Current smokers were those who smoke at least once/month |
| Gordon & Iribarren (2008) | 610 Mexican or Central Amer. | Adults | N/A | Kaiser Permanente of Northern California Adult Member Health Survey | Members were asked if they preferred to discuss their health in English or Spanish, and participants were classified into English, Spanish, and Bilingual | Self report of current smoking |
| Gossage (1998) | 89 Hispanic | Adults | Low income | 7 counties in New Mexico, 2nd wave of the Substance Abuse Epidemiology Unit (SAEU) study | 23 item composite of spoken and written language, generation, ethnic identity of parents and self, ethnicity of friends, nativity, country raised in, and language of TV and music | Self report current smoking in the last 30 day and 90 days and lifetime |
| Kaplan et al. (2001) | 1411 Hispanic | Adoles and adults | Income 92.2% < 15K | Family planning clinics in LA | Nativity, ARSMA, four item familialism measure, and 5 item beliefs about women’s roles scale adapted from the NLSY | Self report, categorized into never smokers, triers, and regular smokers |
| Kasirye et al. (2005) | 1062 Mexican | Adults | N/A | Study for Hispanic Acculturation Reproduction and the Environment recruited from OBGYN offices at San Joaquin General Hospital | ARSMA II | Self report of lifetime cigarette use |
| Khoury et al. (1996) | 210 Hispanic | Adoles | N/A | Dade County Public School District 9th graders | Nativity | Self report of lifetime and current smoking (past 12 month and past 30 day use) |
| Maher et al. (2005) | 723 Hispanic | Adults | N/A | 2000-2002 Oregon Behavioral Risk Factor Surveillance System | Survey Language | Current smokers, have smoked 100 cigarettes in their lifetime, and either smoke every day or some days |
| Marks et al. (1990) | 1575 Mexican415 Cuban677 Puerto Rican | Adults | N/A | Hispanic Health and Nutrition Examination Survey | ARSMA | Self report of current smoking |
| Otero-Sabogal et al. (1995) | 830 Hispanic | Adults | Estimates included male participants | San Francisco and Alameda Counties | SASH | Self report of current and lifetime smoking |
| Parker et al. (2010) | 2029 Mexican | Adults | Estimates included male participants | HMPG medical center, Minneapolis, MN | Primary language | Yes, quit, passive, or not asked from electronic medical records; answers categorized into current, former, or never |
| Perez-Stable (2001) | 4709 Hispanic – one third Mexican | Adults | Income 66.8% < 25K | Puerto Ricans from NY, Cubans from Miami, Mexicans from various cities in TX and San Diego, CA, and Central Americans from SF | SASH and nativity | Self report of smoking behavior – current, former, never |
| Samet et al. (1992) | 629 Hispanic | Adults | N/A | Semi Rural City near Albuquerque, NM | Composite of 4 level scale of ability to read, write, understand and speak Spanish and English and a 5 level scale of language use in family and work settings | Self report of current and lifetime smoking |
| Sarnoff et al. (2001) | 1423 Mexican | Adoles. | 2/3 Medicaid or other public payer | 1994-1995 CA PRAMS | Nativity | Self report of smoking 3 months prior to pregnancy |
| Smith & McGraw (1991) | 224 Puerto Rican | Adoles. | N/A | Boston, Cambridge & Chelsea, MA and Hartford, CT | 3 item language composite of language spoken most often, language spoken in the home, and interview language | Self report of smoking in the previous month |
| Smith & McGraw (1993) | 1085 Puerto Rican | Adults | N/A | Boston, Cambridge & Chelsea, MA and Hartford, CT | 3 item language composite of language spoken most often, language spoken in the home, and interview language | Self report of smoking in the previous month |
| Sundquist & Winkleby (1999) | 761 Mexican | Adults | 24.4% English-speaking below poverty line45.8% Spanish-speaking below poverty line | 1988-1994 National Health and Nutrition Examination Survey | Primary language and nativity | Self report of current smoking and serum cotinine levels for verification purposes |
| Tonin (2006) | 1691 Hispanic | Adoles. | N/A | Existing dataset collected by state agencies in a western state | Language spoken at home | Last 30 day cigarette use, scale of 0-6 (0 = no use and 6 = every day) |
| Trinidad et al. (2006) | 5697 Hispanic | Adults | N/A | California Tobacco Surveys 1996, 1999, 2002 | Primary language | Current smokers have smoked 100 cigarettes in their lifetime and either smoke every day or some days |
| Wilkinson et al. (2005) | 3638 Mexican | Adult | N/A | Houston, TX | Interview language and nativity | Self report of current and lifetime use with current smokers having smoked at least 100 cigarettes in their lifetime |
Note. Studies may contain additional measures of acculturation; however, only those from which an effect size could be obtained were included.
Participant Characteristics
All included studies were conducted in the United States, with the majority (15 total) conducted in the West and Southwest. Six studies sampled participants nationally or in select cities throughout the U.S., and the remaining studies were conducted in the Northeast, Southeast, and Midwest. Sample sizes ranged from n = 57 (Dusenbery & Epstein, 1994) to n = 5,697 (Trinidad et al., 2006), for a total of 39,777 independent participants. Three studies included adolescent girls in middle school and high school, and three studies included adolescents and young women ranging from 14-24 years. One study examined older women, with an age range of 46-92, and a mean age of 71 years (Cantero et al., 1999). The remaining 19 articles included adult participants. Seven of these 19 articles reported mean ages ranging from 25.2 to 44.4 years. Most of the included studies were performed with low-income participants, with three studies reporting all participants as low income and an additional eight studies reporting the majority of participants as low income. Across the studies, English-speaking participants had higher levels of education and income than their Spanish-speaking counterparts, who were more likely to be older and unemployed (see Table 1).
Acculturation, Current and Lifetime Smoking, and Cigarette Smoking Overall
Data from the 26 included studies (k = 32 comparisons) allowed for analyses examining current smoking and lifetime smoking. In addition, both lifetime and time-limited smoking outcomes were combined to derive an overall effect of acculturation on smoking. The mean effect size was computed and utilized for studies reporting both current and lifetime outcomes.
Of the 26 studies, two reported results for separate independent samples (Otero-Sabogal et al., 1995; Trinidad et al., 2006), and two others reported results separately by nationality (Khoury, Warheit, Zimmerman, Vega, & Gil, 1996; Marks et al., 1990), thus increasing the number of comparisons to 32.
Table 2 provides both study level and combined effect sizes for all of the outcomes that we examined. Of the 26 included studies, 24 examined current smoking (k = 30). Tests for heterogeneity were significant (Q [29] = 120.385, p < .001, I2 = 75.911), and a random effects model yielded a mean effect of OR = 1.778, 95% CI [1.554, 2.035]. This mean effect size would be interpreted as small according to Cohen’s guidelines (1988), but according to Rossi’s (2013) recommendations for effect size metrics in the context of health related behaviors, our mean effect size may be interpreted as large. Similar results were found for lifetime smoking, with the 12 (k = 14) included studies significant for heterogeneity, (Q [13] = 37.652, p < .001, I2 = 65.474), and characterized by a mean effect of OR = 2.026, 95% CI [1.598, 2.567]. Finally, the overall analysis of all 26 studies resulted in a significant Q statistic of (Q [31] = 152.171, p < .001, I2 = 79.628), and a mean effect of OR = 1.805, 95% CI [1.572, 2.072]. Appendix C presents the results of tests for publication bias.
Table 2. National Origin, Study Level Effect Sizes, and Combined Mean Effect Sizes.
| Study | National Origin | OR [95% CI] | ||
|---|---|---|---|---|
|
| ||||
| Current | Lifetime | Overall | ||
| Abraido-Lanza et al. (2005) | Unspecified Hispanic | 1.938 [1.419, 2.646] | -- | 1.938 [1.419, 2.646] |
| Balcazar et al. (1995) | Unspecified Hispanic | -- | 1.039 [0.588, 1.836] | 1.039 [0.588, 1.836] |
| Balcazar et al. (1996) | Mexican | 4.292 [1.352, 13.626] | -- | 4.292 [1.352, 13.626] |
| Barger & Gallo (2008) | Unspecified Hispanic | 1.792 [1.188, 2.704] | -- | 1.792 [1.188, 2.704] |
| Cantero et al. (1999) | Unspecified Hispanic | 1.944 [1.099, 3.442] | 1.696 [1.108, 2.596] | 1.816 [1.098, 3.005] |
| Coonrod et al. (1999) | Mexican | 3.894 [0.845, 17.945] | 4.127 [1.150, 14.814] | 4.009 [0.980, 16.395] |
| Corral & Landrine (2008) | Mexican | 3.109 [2.145, 4.506] | -- | 3.109 [2.145, 4.506] |
| Dusenbery & Epstein (1994) | Unspecified Hispanic | 2.350 [0.828, 6.672] | 1.130 [0.508, 2.512] | 1.630 [0.643, 4.127] |
| Gordon & Iribarren (2008) | Unspecified Hispanic | 1.251 [0.333, 4.699] | -- | 1.251 [0.333, 4.699] |
| Gossage (1998) | Unspecified Hispanic | 1.234 [0.398, 3.828] | 2.675 [0.891, 8.029] | 1.597 [0.520, 4.901] |
| Kaplan et al. (2001) | Unspecified Hispanic | 3.426 [2.132, 5.506] | 2.085 [1.587, 2.740] | 2.180 [1.627, 2.923] |
| Kasirye et al. (2005) | Mexican | -- | 5.485 [3.608, 8.340] | 5.485 [3.608, 8.340] |
| Khoury et al. (1996)a | Cuban | 1.477 [0.359, 6.069] | 1.411 [0.557, 3.572] | 1.443 [0.437, 4.773] |
| Khoury et al. (1996)b | Unspecified Hispanic | 1.483 [0.426, 5.155] | 1.587 [0.775, 3.249] | 1.517 [0.506, 4.549] |
| Maher et al. (2005) | Unspecified Hispanic | 7.700 [3.597, 16.485] | -- | 7.700 [3.597, 16.485] |
| Marks et al. (1990)a | Cuban | 0.964 [0.679, 1.369] | -- | 0.964 [0.679, 1.369] |
| Marks et al. (1990)b | Mexican | 1.388 [1.159, 1.662] | -- | 1.388 [1.159, 1.662] |
| Marks et al. (1990)c | Puerto Rican | 1.870 [1.416, 2.469] | -- | 1.870 [1.416, 2.469] |
| Otero-Sabogal et al. (1995)a | Unspecified Hispanic | 2.282 [1.326, 3.927] | 2.398 [1.590, 3.617] | 2.339 [1.445, 3.786] |
| Otero-Sabogal et al. (1995)b | Unspecified Hispanic | 2.843 [1.665, 4.854] | 1.940 [1.270, 2.964] | 2.348 [1.449, 3.805] |
| Parker et al. (2010) | Mexican | 2.064 [1.274, 3.345] | 2.555 [1.961, 3.328] | 2.296 [1.556, 3.389] |
| Perez-Stable (2001) | Unspecified Hispanic | 1.291 [1.019, 1.637] | -- | 1.291 [1.019, 1.637] |
| Samet et al. (1992) | Unspecified Hispanic | 0.698 [0.161, 3.020] | 0.548 [0.127, 2.365] | 0.618 [0.143, 2.672] |
| Sarnoff et al. (2001) | Mexican | 3.391 [2.367, 4.857] | -- | 3.391 [2.367, 4.857] |
| Smith & McGraw (1991) | Puerto Rican | 1.313 [0.846, 2.036] | -- | 1.313 [0.846, 2.036] |
| Smith & McGraw (1993) | Puerto Rican | 1.158 [0.989, 1.357] | -- | 1.158 [0.989, 1.357] |
| Sundquist & Winkleby (1999) | Mexican | 1.239 [0.879, 1.746] | -- | 1.239 [0.879, 1.746] |
| Tonin (2006) | Unspecified Hispanic | 1.126 [0.947, 1.339] | -- | 1.126 [0.947, 1.339] |
| Trinidad et al. (2006)a | Unspecified Hispanic | 1.677 [1.385, 2.032] | -- | 1.677 [1.385, 2.032] |
| Trinidad et al. (2006)b | Unspecified Hispanic | 1.691 [1.393, 2.052] | -- | 1.691 [1.393, 2.052] |
| Trinidad et al. (2006)c | Unspecified Hispanic | 1.555 [1.362, 1.776] | -- | 1.555 [1.362, 1.776] |
| Wilkinson et al. (2005) | Mexican | 2.001 [1.215, 3.294] | 1.882 [1.240, 2.855] | 1.940 [1.225, 3.072] |
| Combined Mean | 1.778 [1.554, 2.035] | 2.026 [1.598, 2.567] | 1.805 [1.572, 2.072] | |
Note. Four studies reported results of more than one independent sample, each of which were coded separately.
The Impact of Moderating Variables
The significance of moderating variables was assessed using the meta-analytic analog ANOVA approach for all examined outcomes. Comparisons were performed examining (1) the difference in the effect of acculturation on smoking in adolescents as compared with adults, (2) the differences among Mexicans, Cubans, Puerto Ricans, and unspecified Hispanic groups5, and (3) the type of acculturation measure used in the study. Significant age-group (adolescent versus adult) differences in the effect of acculturation emerged for both current smoking (QB [26] = 11.975, p < .01) and smoking overall (QB [28]= 14.473, p < .001), but not for lifetime smoking and indicated a larger effect of acculturation on cigarette smoking in adults (see Table 3).
Table 3. Comparisons of Acculturation on Smoking Outcomes by Age.
| Age Group | k | OR [95% CI] | Q (df) | QB (df) |
|---|---|---|---|---|
| Overall Smoking | ||||
| Adults | 25 | 1.771 [1.532, 2.049] | 112.588 (24)** | |
| Adolescents | 4 | 1.153 [.976, 1.362] | 0.977 (3) | 14.473 (28)** |
|
| ||||
| Current Smoking | ||||
| Adults | 23 | 1.686 [1.480, 1.921] | 74.767 (22)** | |
| Adolescents | 4 | 1.158 [.979, 1.370] | 2.130 (3) | 11.975 (26)* |
|
| ||||
| Lifetime Smoking | ||||
| Adults | 10 | 2.177 [1.597, 2.966] | 32.705 (9)** | |
| Adolescents | 3 | 1.375 [.866, 2.184] | 0.388 (2) | 2.614 (12) |
p < .01,
p < .001
Comparisons for both overall and current smoking by national origin indicated that mean effect sizes for Cuban women were significantly lower than those for Mexican and unspecified Hispanic women. Further, effect sizes for Mexican women were also significantly higher than Puerto Rican women in the overall smoking comparison and significantly higher than unspecified Hispanic women in lifetime smoking. No other significant nationality differences were found (see Table 4).
Table 4. Comparisons of Women of Mexican descent to Other Nationalities.
| National Origin | k | OR [95% CI] | Q (df) | QB (df) |
|---|---|---|---|---|
| Smoking Overall | ||||
| Mexican | 9 | 2.512 [1.724, 3.659] | 62.387 (8)*** | -- |
| Cuban | 2 | .996 [.711, 1.393] | 0.402 (1) | 12.925 (10)*** |
| Unspecified Hispanic | 18 | 1.697 [1.464, 1.966] | 50.842 (18)*** | 3.622 (26) |
| Puerto Rican | 3 | 1.407 [1.011, 1.959] | 8.612 (2)* | 5.141 (11)* |
|
| ||||
| Current Smoking | ||||
| Mexican | 8 | 2.179 [1.544, 3.075] | 36.445 (7)*** | -- |
| Cuban | 2 | .988 [.704, 1.389] | 0.329 (1) | 10.250 (9)*** |
| Unspecified Hispanic | 17 | 1.810 [1.529, 2.142] | 56.169 (16)*** | 0.901 (24) |
| Puerto Rican | 3 | 1.407 [1.011, 1.959] | 8.612 (2)* | 3.223 (10) |
|
| ||||
| Lifetime Smoking | ||||
| Mexican | 4 | 3.062 [1.862, 5.036] | 14.167 (3)** | -- |
| Cuban | 1 | 1.411 [.557, 3.572] | -- | -- |
| Unspecified Hispanic | 9 | 1.768 [1.435, 2.179] | 11.149 (8) | 3.983 (12)* |
p < .05,
p < .01,
p < .001
Finally, analyses were performed to explore differences resulting from the measure of acculturation utilized. Comparisons included the use of proxy variables as compared with a composite or scale; linguistic acculturation (both proxy language variables and language-based composites and scales were included) as compared with nativity (the only other proxy variable utilized in enough studies for comparison); unidimensional as compared with bidimensional acculturation measures; and the categorization of acculturation as dichotomous (e.g., English vs. Spanish speaking) as compared with three categories (e.g., English, Spanish and English, Spanish speaking). Although the vast majority of comparisons were nonsignificant, including the use of a proxy variable as compared to the use of a composite or scale, the effect of nativity specifically as a proxy variable emerged as significantly higher compared to the use of a composite or scale for current smoking (QB [20] = 3.906, p = .048), but not for lifetime smoking or for smoking overall. In addition, while not statistically analyzed due to dependent samples, manual examination of mean effect sizes and confidence intervals suggest that for current smoking, a noteworthy difference may exist between the mean effect of OR = 2.034, 95% CI [1.734, 2.386] for the dichotomized “high” vs. “low” acculturation variable versus both the “high” vs. “middle” category (OR = 1.256, 95% CI [0.830, 1.899]) and the “middle” vs. “low” category (OR = 1.417, 95% CI [0.981, 2.046]). For overall smoking, the mean effect sizes of “high” vs. “middle” and the “middle” vs. “low” categories appeared to be lower than the mean effect sizes for the high/low comparisons. However, the CIs for these comparisons overlapped, suggesting that these differences may not be reliable (see Table 5). No significant differences emerged between studies using unidimensional versus bidimensional acculturation measures.
Table 5. Summary of Smoking Findings by Categorization of Acculturation Measure.
| Measure | Overall Smoking | Current Smoking | Lifetime Smoking | |||
|---|---|---|---|---|---|---|
|
| ||||||
| k | OR [95% CI] | k | OR [95% CI] | k | OR [95% CI] | |
| High vs. Low | 27 | 2.113 [1.767, 2.527] | 25 | 2.034 [1.734, 2.386] | 13 | 2.350 [1.771, 3.119] |
| High vs. Middle | 7 | 1.497 [.997, 2.249] | 6 | 1.256 [.830, 1.899] | 5 | 1.798 [1.216, 2.658] |
| Middle vs. Low | 8 | 1.535 [0.978, 2.411] | 6 | 1.417 [.981, 2.046] | 6 | 1.627 [.859, 3.081] |
| Total | 32 | 1.805 [1.572, 2.072] | 30 | 1.778 [1.554, 2.035] | 14 | 2.026 [1.598, 2.567] |
Note. A number of included studies reported results for multiple outcomes and used multiple acculturation measures. Thus, statistical analysis was not performed due to violation of the assumption of independence.
Discussion
The present meta-analysis was guided by four objectives. The primary objective of this study was to quantitatively synthesize the extant literature examining acculturation and cigarette smoking in Hispanic women. Secondary aims included (a) assessing the potential moderating influence of demographic variables such as age and national origin, (b) to examine whether acculturation is more closely related to different patterns of smoking, and (c) to investigate whether differences in effect sizes would emerge based on the method used to measure acculturation.
Given the overall near-consensus in the field, it was not surprising that, across studies, acculturation is positively related to smoking behaviors in Hispanic women. More importantly, our moderator analyses indicated significant differences in the effect of acculturation on smoking along variables such as age, ethnicity, and how acculturation was measured. Specifically, the mean effects of acculturation on overall and current smoking were significantly higher in adults than in adolescents. These findings may suggest that, for adolescents, familial factors such as parent/child acculturation discrepancies may be a more important factor than adolescent acculturation alone with regard to current and overall smoking (Martinez, 2006; Unger, Ritt-Olson, Wagner, Soto, & Baezconde-Garbanati, 2009). Such familial acculturation discrepancies would not be expected to influence smoking behaviors among adults. That said, no age group differences emerged for lifetime smoking behaviors. This pattern of findings suggests that although familial processes such as parental warmth and perceived parental monitoring (Mogro-Wilson, 2008; Pokhrel, Unger, Wagner, Ritt-Olson, & Sussman, 2008) may serve to offset the development of smoking habits in teens, they may not impact smoking experimentation.
Large differences emerged in mean effects when comparing women by nationality. The effect of acculturation on smoking in Cubans was null and significantly lower than both Mexican women and the unspecified Hispanic category for overall and current smoking outcomes. Conversely, mean effects of acculturation on overall smoking were significantly higher for Mexicans as compared to Cubans and Puerto Ricans, and mean effects on lifetime smoking were significantly higher for Mexicans than for unspecified Hispanics. In general, it has been suggested that increases in smoking in Hispanic women as a result of acculturation may be due to the discouragement of smoking among women in Latin American countries and the acceptability of such behaviors in the United States (Bethel & Schenker, 2005; Wilkinson et al., 2005). Although this pattern is plausible for the majority of ethnic subgroups examined here, our results suggest that acculturation has no effect on smoking in Cubans. Studies indicate that Puerto Ricans and Cubans report the highest rates of smoking among Hispanic women in the United States, with Cubans more likely to be heavy smokers (American Lung Association, 2010; Office on Women’s Health, 2001; Perez-Stable et al., 2001). In addition, unlike many Latin American countries, cultural norms in Cuba do not strongly discourage smoking for women, resulting in higher smoking rates (22.3% in 2001; Varona, Chang, Garcia, & Bonet, 2011). Perhaps acculturation has little or no effect on behaviors when the cultural norms of that behavior are similar in both the country of origin and the United States. These findings illustrate the heterogeneity within the Hispanic population and highlight the importance of examining individual national groups rather than large, pan-ethnic categories, as this practice can mask a great deal of heterogeneity. However, the results and conclusions regarding Cubans must be interpreted with great caution, given that only two of the included studies (one with adolescents and one with adults) identified participants as Cuban. More research is warranted to better understand the effects of acculturation on smoking behaviors among Cuban American women.
Our examination of Puerto Rican women suggests that acculturation is positively associated with cigarette smoking. However, the overall effect (OR = 1.407) is quite small, even according to Rossi’s (2013) more generous guidelines. Results comparing Puerto Ricans to other ethnic subgroups suggest that the effect of acculturation on smoking overall in Puerto Ricans is lower compared to the corresponding effect among Mexicans. It is important to note that only 8.7% of island Puerto Rican women, compared to 24.2% of mainland Puerto Rican women, report smoking (American Lung Association, 2010; Centers for Disease Control and Prevention, 2005; Perez-Stable et al., 2001). Although acculturation (which would be assumed to be higher among Puerto Ricans on the U.S. mainland than among those living in Puerto Rico) would be a logical explanation for these differences in smoking prevalence, these results do not support the significant differences in reported rates. Consequently, more research on acculturation and smoking among Puerto Rican women is needed.
As compared with other ethnic subgroups, the research base for Mexican-descent women is large, and results can be interpreted with a reasonable degree of confidence. Our results indicate that Mexican women had significantly higher acculturation-overall smoking mean effects compared to Puerto Rican and Cuban women and a higher mean effect than unspecified Hispanics for lifetime smoking. The overall trend found for Mexican women is that acculturation increases the likelihood of smoking. Significant differences between Mexicans and at least one other ethnic subgroup emerged in all of the analyses. Although large effects of acculturation emerged for all smoking behaviors, the mean effect of acculturation on lifetime smoking was higher than the effect on current smoking, suggesting the possibility that, in Mexican women, acculturation may exert its strongest effect on experimentation. More in-depth studies of acculturation and experimental smoking among Mexican-descent women are needed to further explore the present findings.
When measure of acculturation was examined as a moderator, the only significant difference was a higher mean effect of nativity as compared to a composite or scale in current smoking. No other differences emerged among proxies or scales, or between unidimensional and bidimensional acculturation measures. However, these results must be interpreted with extreme caution, as 24 of the 26 studies used a unidimensional acculturation measure, with only two conceptualizing acculturation as bidimensional. While preliminary in nature, these findings suggest that, although a wide variety of acculturation measures have been used, in many cases the smoking behaviors that are associated with acculturation may be adequately captured regardless of the type or dimensionality of acculturation measure. This conclusion is in direct conflict with the current recommendations in the field, which urge researchers to avoid proxy variables and other unidimensional measures and to utilize bidimensional or multidimensional scales. More research in this area is clearly warranted (see Schwartz et al., 2010). It is possible that smoking behaviors become more likely with increasing engagement in U.S. cultural behaviors and that these increases in engagement are captured equivalently by proxy measures, unidimensional scales, and multidimensional scales. It is not yet known whether similar findings would emerge for use of other substances. Inclusion of more studies using a bidimensional approach to acculturation in future meta-analytic work is also needed.
Finally, although no formal comparisons were performed due to statistically dependent effect sizes, in an effort to better understand the significance of timing - one area of interest was whether changes in smoking behavior occurred at different degrees of acculturation. Most of the included studies reported results comparing assumedly higher degrees of acculturation (e.g., English language, U.S. born) to lower degrees (e.g., Spanish language, foreign born); however, a sufficient number of studies utilized measures that allowed for a “middle” category, such as English vs. bilingual vs. Spanish or 1st generation vs. 2nd generation vs. 3rd generation. The mean effect sizes and confidence intervals were visually inspected for differences among these comparisons, and results suggest that, although subtle, the inclusion of intermediate stages may allow for a more nuanced effect. As expected, dichotomized “high” vs. “low” measures produced higher mean effects than those measuring participants at “low” vs. “middle” and “middle” vs. “high” stages. No differences between the mean effects of participants at “low” vs. “middle” and “middle” vs. “high” stages were noted, suggesting that timing may not influence the relationship between acculturation and smoking behaviors in Hispanic women.
Limitations and Future Directions
As with any meta-analysis, this study has important limitations. First, the number of studies included in the subgroup analyses was small, with wide confidence intervals and low power, which greatly limits our ability to generalize the results found here to the population at large. Additionally, missing data and publication bias is one common area of concern in a meta-analysis, and this study is no exception. A concerted effort was made to locate all studies relevant to the analyses, both published and unpublished; however, a large number of studies were excluded due to the lack of data needed for inclusion, and it is probable that potentially relevant studies may have been missed.
Second, the included studies varied in terms of reporting and methodological quality. Inconsistencies in the data reported created challenges, as studies varied in their definitions of outcome (e.g., current or lifetime smoking) and how these outcomes were measured (e.g., self-report or biological measures of cotinine). With regard to acculturation, although one of the study’s aims was to gain a better understanding of moderating effects of measurement variations, this lack of consistency in acculturation measurement served as an inherent limitation. Although our analyses concluded that, in general, proxy measures and scales adequately capture similar information overall, we are still left with the question of comparing “apples” and “oranges.” Are Hispanics who speak English acculturated to the same degree as those who are born in the United States? Does the answer to this question depend on the specific context (e.g., ethnic enclave) in which the person resides? Comparing results across measurement approaches was further complicated by the use of composite variables and scales, some validated and formal, but many of which were developed specifically for individual studies and used quasi-continuous variables to categorize acculturation. Future studies should be cognizant of these inconsistencies when determining how acculturation should be measured. Moreover, more research is needed to better understand and identify the differences in aspects of acculturation that these commonly utilized measures capture, as well as the mediating mechanisms through which acculturation affects smoking in Hispanic women.
Another area to which the “apples” to “oranges” challenge applies is the common aggregation of Hispanics into a homogenous ethnic/racial category. The general conclusion of this study was similar to previous research in the area – that is, a positive effect exists when examining smoking behaviors. However, these conclusions are likely weighted heavily by a large percentage of participants from Mexico – a country in which smoking norms for women are much more restrictive than in the United States; thus, as women acculturate to U.S. norms, their smoking behaviors increase. The problem is that we cannot assume that all Hispanics are the same or that all Latin American countries are strict in smoking norms for women since this simply is not the case. As a result of the large percentage of Hispanics in the United States being of Mexican descent, it is likely that results pertaining to individuals from other countries are obscured. To better clarify the behavioral effects which occur as a result of acculturation in different Hispanic ethnic subgroups, future researchers should oversample Hispanic groups that are less well represented in the general U.S. population.
Finally, previous research has indicated that differences exist in the behavioral outcomes of acculturation when comparing adolescents to adults, and the same is true when comparing older to younger adults (Markides et al., 1988; Markides et al., 1990; Perez-Stable, 2001). In order to better understand the mechanisms through which these behavioral changes occur as Hispanics acculturate, it is important that future research examine Hispanic women at various stages of life with the a priori assumption that differences exist.
Despite limitations, the findings of this meta-analysis add to our understanding of the relationship between acculturation and cigarette smoking in Hispanic women by quantifying the effect of acculturation across studies and identifying significant moderating factors. These results not only confirm the general consensus in the field, but also suggest that within the context of health related behaviors, the effect of acculturation on smoking may be relatively large (Rossi, 2013). In addition, the significant differences that emerged by national origin highlight the importance of the recognition that Hispanics are a large and heterogeneous group. As such, studies should examine ethnic subgroups independently. Further, while future research is necessary, our virtual lack of significant differences when comparing measures of acculturation suggest that the commonly used measures in the field may be capturing the components of acculturation related to cigarette smoking. However, a better understanding of the timing or stage at which changes resulting from acculturation occur is especially important. If a sensitive period of acculturation (Cheung, Chudek, & Heine, 2011) vis-à-vis changes in behaviors such as smoking can be identified, clinicians and public health officials may be better equipped and able to target education and prevention efforts to those at higher risk. It is our hope that this study will serve as a reminder of the complexities related to acculturation in Hispanics and the importance of examining context in future research. A better understanding of the differences in experiences and outcomes related to acculturation within the Hispanic population will better inform the development of targeted interventions aimed at smoking prevention and the prevention of other health-compromising behaviors.
Acknowledgments
We wish to express our gratitude to Dr. Kathryn Quina, Dr. Margaret Rogers, and Dr. Diane Martins for your contributions to this project from inception to completion. We also wish to thank Delia Sosa and Erica Ironside for their assistance with manuscript preparation.
Declaration of Interest: This research was supported in part by the National Center for Research Resources of the National Institutes of Health under Award Number G20RR030883. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Appendix A: PICOTS Table
| Key Question |
KQ1. What is the relationship between acculturation and cigarette smoking in Hispanic women?
|
| Populations | Hispanic Women |
| Intervention | Acculturation. Measures of acculturation may include proxy variables (e.g., nativity, length of time in the U.S., language), unidimensional scales (e.g., Acculturation Rating Scale for Mexican Americans [ARSMA]), or bidimensional scales (e.g., Acculturation Rating Scale for Mexican Americans-II [ARSMA-II]). |
| Comparator | Other Hispanic women |
| Outcomes | Cigarette smoking (current – 30 day, 90 days, 1 year; lifetime) |
| Timing | Short and long term outcomes |
| Study design | All study designs will be considered. Studies must be quantitative and provide data from which an effect size can be calculated. |
Appendix B: PubMed Search Strategy
((((“acculturation”[MeSH Terms] OR “acculturation”[All Fields]) AND (“health”[MeSH Terms] OR “health"[All Fields])) AND ((“acculturation” [MeSH Terms] OR “acculturation” [All Fields]) AND (“smoking” [MeSH Terms] OR “smoking” [All Fields]))) AND ((“acculturation” [MeSH Terms] OR “acculturation” [All Fields]) AND (“hispanic americans” [MeSH Terms] OR (“hispanic” [All Fields] AND “americans” [All Fields]) OR vhispanic americans” [All Fields] OR “hispanic” [All Fields]))) AND ((((“mexican” [All Fields] OR “puerto rican"[All Fields]) OR “cuban” [All Fields]) OR “central american” [All Fields]) OR “south american” [All Fields]) AND ((“1990/01/01” [PDAT] : “3000/12/31”[PDAT]) AND “female”[MeSH Terms])
Appendix C: Test of Publication Bias
Table C1. Tests for Publication Bias.
| Outcome | Orwin’s N | Egger’s Regression Intercept | Duval and Tweedie’s Trim and Fill | |
|---|---|---|---|---|
| # of Imputed | Adjusted Mean Effect | |||
| Overall Smoking | 269 | b = 1.52, SE = 0.605, t(28) = 2.514, p = 0.018, 95% CI [0.28, 2.759] | 2 | OR = 1.873, 95% CI [1.625, 2.159] |
| Current Smoking | 239 | b = 1.52, SE = 0.680, t(30) = 2.248, p = 0.032, 95% CI [0.14, 2.919] | 0 | OR = 1.778, 95% CI [1.554, 2.035] |
| Lifetime Smoking | 211 | b = -1.20, SE = 1.013, t(12) = 1.186, p = 0.256, 95% CI [-3.407, 1.005] | 3 | OR = 2.302, 95% CI [1.803, 2.938] |
Note. Orwin’s fail-safe N criterion of OR = 1.05.
Figure C1.

Funnel plot with both observed and imputed (dark) studies for Overall Smoking
Figure C2.

Funnel plot with both observed and imputed (dark) studies for Current Smoking
Figure C3.

Funnel plot with both observed and imputed (dark) studies for Lifetime Smoking
Footnotes
Acculturation can encompass changes in the following cultural domains: practices (language use, choice of friends), values (beliefs about the importance of an individual and of the larger social group), and identifications (sense of self as a member of a group within the host society). Acculturation can also be conceptualized unidimensionally or bidimensionally. The bulk of smoking research has conceptualized as a unidimensional process, which assumes that as an individual identifies with the host society and acquires the cultural practices and values of the receiving culture, one automatically discards her or his heritage practices, values, and identifications.
e.g., Smith & McGraw (1993) used a three item language-based composite variable. Participant language preference, language spoken in the household, and interview language were each assessed using the scale of 0 = Spanish only; 1 = English and Spanish; and 2 = English only, with the sum used as an index of acculturation.
The term multidimensional is commonly used to describe acculturation scales (e.g., Abbreviated Multidimensional Acculturation Scale; Zea, Asner-Self, Birman, & Buki, 2003). However, while the term multidimensional suggests reference to the conceptualization of acculturation (i.e., unidimensional vs. bidimensional), multidimensional refers rather to the assessment of multiple cultural domains (i.e., practices, values, and identifications).
A limited number of studies (e.g., Perez-Stable, 2001) assessed acculturation using multiple proxy measures, with independent results reported for each.
Unspecified Hispanics represent samples that were not disaggregated by the researchers for analysis.
References
References marked with an asterisk were included in the meta-analysis
- Abraído-Lanza A, Chao M, Flórez K. Do healthy behaviors decline with greater acculturation?: Implications for the Latino mortality paradox. Social Science & Medicine. 2005;61(6):1243–1255. doi: 10.1016/j.socscimed.2005.01.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Lung Association. Hispanics. 2010 Retrieved from http://www.lungusa.org/stop-smoking/about-smoking/facts-figures/hispanics-and-tobacco-use.html.
- Balcazar H, Castro FG, Krull JL. Cancer risk reduction in Mexican American women: the role of acculturation, education, and health risk factors. Health Education and Behavior. 1995;22(1):61–84. doi: 10.1177/109019819502200107. [DOI] [PubMed] [Google Scholar]
- Balcazar H, Peterson G, Cobas J. Acculturation and health-related risk behaviors among Mexican-American pregnant youth. American Journal of Health Behavior. 1996;20(6):425–433. [Google Scholar]
- Barger SD, Gallo LC. Ability of ethnic self-identification to partition modifiable health risk among U.S. residents of Mexican ancestry. American Journal of Public Health. 2008;98(11):1971–1978. doi: 10.2105/AJPH.2007.122754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bethel JW, Schenker MB. Acculturation and smoking patterns among Hispanics: A review. American Journal of Preventive Medicine. 2005;29(2):142–148. doi: 10.1016/j.amepre.2005.04.014. [DOI] [PubMed] [Google Scholar]
- Borenstein M. Effect sizes for continuous data. In: Cooper H, Hedges LV, Valentine JC, editors. The handbook of research synthesis and meta-analysis. 2nd. New York: Russell Sage Foundation; 2009. pp. 221–253. [Google Scholar]
- Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to meta-analysis. New York: Wiley; 2009. [Google Scholar]
- Bruce N, Pope D, Stanistreet D. Systematic reviews and meta-analysis in quantitative methods for health research: A practical interactive guide to epidemiology and statistics. Chichester, UK: John Wiley & Sons; 2008. [Google Scholar]
- Cabassa LJ. Measuring acculturation: Where we are and where we need to go. Hispanic Journal of Behavioral Sciences. 2003;25(2):127–146. [Google Scholar]
- Cantero PJ, Richardson JL, Baezconde-Garbanati L, Marks G. The association between acculturation and health practices among middle-aged and elderly Latina. Ethnicity and Disease. 1999;9(2):166–180. [PubMed] [Google Scholar]
- Caraballo RS, Yee SL, Gfroerer J, Mirza SA. Adult tobacco use among racial and ethnic groups living in the United States, 2002-2005. Preventing Chronic Disease. 2008;5(3):1–9. [PMC free article] [PubMed] [Google Scholar]
- Castro FG. Emerging Hispanic health paradoxes. American Journal of Public Health. 2013;103:1541. doi: 10.2105/AJPH.2013.301529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Cigarette Smoking in the United States: Current cigarette smoking among U.S. adults aged 18 years and older. 2013a Retrieved from http://www.cdc.gov/tobacco/campaign/tips/resources/data/cigarette-smoking-in-united-states.html#hispanics.
- Centers for Disease Control and Prevention. Health Effects of Cigarette Smoking. 2013b Retrieved from http://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/index.htm.
- Centers for Disease Control and Prevention. Tobacco-Related Mortality. 2013c Retrieved from http://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/tobacco_related_mortality/
- Cheung BY, Chudek M, Heine SJ. Evidence for a sensitive period for acculturation: Younger immigrants report acculturating at a faster rate. Psychological Science. 2011;22:147–152. doi: 10.1177/0956797610394661. [DOI] [PubMed] [Google Scholar]
- Chun KM, Balls Organista P, Marín G. Acculturation: Advances in theory, measurement and applied research. Washington, DC: American Psychological Association; 2003. [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd. Hillsdale, NJ: Lawrence Earlbaum Associates; 1988. [Google Scholar]
- Coonrod D, Balcazar H, Brady J, Garcia S, Van Tine M. Smoking, acculturation and family cohesion in Mexican-American women. Ethnic Disparities. 1999;9(3):434–440. [PubMed] [Google Scholar]
- Corral I, Landrine H. Acculturation and ethnic-minority health behavior: A test of the operant model. Health Psychology. 2008;27(6):737–745. doi: 10.1037/0278-6133.27.6.737. [DOI] [PubMed] [Google Scholar]
- Cuellar I, Harris LC, Jasso R. An acculturation scale for Mexican American normal and clinical populations. Hispanic Journal of Behavioral Sciences. 1980;2:199–217. [Google Scholar]
- Cuellar I, Arnold B, Maldonado R. Acculturation Rating Scale for Mexican Americans-II: A revision of the original ARSMA scale. Hispanic Journal of Behavioral Sciences. 1995;17(3):275–304. [Google Scholar]
- Dusenbery L, Epstein JA, Botvin GJ, Diaz T. The relationship between language spoken and smoking among Hispanic-Latino youth in New York City. Public Health Reports. 1994;109(3):421. [PMC free article] [PubMed] [Google Scholar]
- Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple graphical test. BMJ. 1997;315(7109):629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleiss JL, Berlin JA. Effect sizes for dichotomous data. In: Cooper H, Hedges LV, Valentine JC, editors. The handbook of research synthesis and meta-analysis. 2nd. New York, NY: Russell Sage Foundation; 2009. pp. 237–253. [Google Scholar]
- Gordon NP, Iribarren C. Health-related characteristics and preferred methods of receiving health education according to dominant language among Latinos aged 25 to 64 in a large Northern California health plan. BMC Public Health. 2008;8:305–313. doi: 10.1186/1471-2458-8-305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gossage JP. Doctoral dissertation. An examination of the relationship of acculturation to high-risk behaviors among Hispanic women of childbearing age in New Mexico. Available from PsychInfo. (UMI no. 9826620) [Google Scholar]
- Kaplan CP, Nápoles-Springer A, Stewart SL, Pérez-Stable EJ. Smoking acquisition among adolescents and young Latinas The role of socioenvironmental and personal factors. Addictive Behaviors. 2001;26(4):531–550. doi: 10.1016/s0306-4603(00)00143-x. [DOI] [PubMed] [Google Scholar]
- Kasirye OC, Walsh JA, Romano PS, Beckett LA, Garcia JA, Elvine-Kreis B, Schenker MB. Acculturation and its association with health-risk behaviors in a rural Latina population. Ethnicity and Disease. 2005;15(4):733–739. [PubMed] [Google Scholar]
- Khoury EL, Warheit GJ, Zimmerman RS, Vega WA, Gil AG. Gender and ethnic differences in the prevalence of alcohol, cigarette, and illicit drug use over time in a cohort of young Hispanic adolescents in south Florida. Women & Health. 1996;24(1):21–40. doi: 10.1300/J013v24n01_02. [DOI] [PubMed] [Google Scholar]
- Kimbro RT. Acculturation in context: Gender, age at migration, neighborhood ethnicity, and health behaviors. Social Science Quarterly. 2009;90(5):1145–1166. [Google Scholar]
- Larisey JT, Hummer RA, Rath JM, Villanti AC, Hayward MD, Vallone DM. Race/ethnicity, nativity, and tobacco use among U.S. young adults: Results from a nationally representative survey. Nicotine & Tobacco Research. 2013;15(8):1417–1426. doi: 10.1093/ntr/nts344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lipsey MW, Wilson DB. Practical Meta-Analysis. Thousand Oaks, CA: Sage; 2001. [Google Scholar]
- Lorenzo-Blanco EI, Corina LM. Latino/a depression and smoking: an analysis through a lens of culture, gender, and ethnicity. American Journal of Community Pyschology. 2013;51(3-4):332–346. doi: 10.1007/s10464-012-9553-3. [DOI] [PubMed] [Google Scholar]
- Maher JE, Boysun MJ, Rohde K, Stark MJ, Pizacani BA, Dilley J, Pickle KE. Are Latinos really less likely to be smokers? Lessons from Oregon. Nicotine & Tobacco Research. 2005;7(2):283–287. doi: 10.1080/14622200500056259. [DOI] [PubMed] [Google Scholar]
- Marin G, Sabogal F, Marin B, Otero-Sabogal R, Perez-Stable EJ. Development of a short acculturation scale for Hispanics. Hispanic Journal of Behavioral Sciences. 1987;9(2):183–205. [Google Scholar]
- Markides KS, Krause N, Mendes de Leon CF. Acculturation and alcohol consumption among Mexican Americans: A three-generation study. American Journal of Public Health. 1988;78(9):1178–1181. doi: 10.2105/ajph.78.9.1178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markides KS, Ray LA, Stroup-Benham CA, Trevino F. Acculturation and alcohol consumption in the Mexican American population of the Southwestern United States: Findings from HHANES 1982-84. American Journal of Public Health. 1990;80(Supplement):42–46. doi: 10.2105/ajph.80.suppl.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marks G, Garcia M, Solis J. Health risk behaviors of Hispanics in the United States: Findings from HHANES, 1982-84. American Journal of Public Health. 1990;80(Supplement):20–26. doi: 10.2105/ajph.80.suppl.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martinez CR. Effects of differential family acculturation on Latino adolescent substance use. Family Relations. 2006;55(3):306–317. [Google Scholar]
- Mogro-Wilson C. The influence of parental warmth and control on Latino adolescent alcohol use. Hispanic Journal of Behavioral Science. 2008;30(1):89–105. [Google Scholar]
- Office on Women’s Health. Surgeon General's Report on Women and Smoking: Hispanic Women and Smoking. 2001 Retrieved from http://www.womenshealth.gov/archive/owh/pub/factsheets/smoking_hispanic.cfm.
- Otero-Sabogal R, Sabogal F, Perez-Stable EJ, Hiatt RA. Dietary practices, alcohol consumption, and smoking behavior: Ethnic, sex, and acculturation differences. Journal of the National Cancer Institute Monographs. 1995;18:73–82. [PubMed] [Google Scholar]
- Parker ED, Solberg LI, Foldes SS, Walker PF. A surveillance source of tobacco use differences among immigrant populations. Nicotine & Tobacco Research. 2010;12(3):309–314. doi: 10.1093/ntr/ntp211. [DOI] [PubMed] [Google Scholar]
- Perez-Stable EJ, Ramirez A, Villareal R, Talavera GA, Trapido E, Suarez L, McAlister A. Cigarette smoking behavior among US Latino men and women from different countries of origin. American Journal of Public Health. 2001;91(9):1424–1430. doi: 10.2105/ajph.91.9.1424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson GW, Cobas JA, Balcazar H, Amling JW. Acculturation and risk behavior among pregnant Mexican American females: A structural equation model. Sociological Inquiry. 1998;68(4):536–556. [Google Scholar]
- Pokhrel P, Unger J, Wagner K, Ritt-Olson A, Sussman S. Effects of parental monitoring, parent-child communication, and parents’ expectation of the child’s acculturation on the substance use behaviors of urban, Hispanic adolescents. Journal of Ethnicity in Substance Abuse. 2008;7(2):200–213. doi: 10.1080/15332640802055665. [DOI] [PubMed] [Google Scholar]
- Rossi JS. Statistical power analysis. In: Schinka JA, Velicer WF, editors. The handbook of psychology: Volume 2, research methods in psychology. Hoboken, NJ: John Wiley & Sons; 2013. pp. 71–108. [Google Scholar]
- Sam DL, Berry JW. Acculturation: When individuals and groups of different cultural backgrounds meet. Perspectives on Psychological Science. 2010;5(4):472–481. doi: 10.1177/1745691610373075. [DOI] [PubMed] [Google Scholar]
- Samet JM, Howard CA, Coultas DB, Skipper BJ. Acculturation, education, and income as determinants of cigarette smoking in New Mexico Hispanics. Cancer Epidemiology Biomarkers and Prevention. 1992;1(3):235–240. [PubMed] [Google Scholar]
- Sarnoff R, Adams E, Shauffler H, Abrams B. Disparities in reported prenatal care advice from health care providers among women of Mexican origin in California. Journal of Immigrant Health. 2001;3(2):77–84. doi: 10.1023/A:1009561832643. [DOI] [PubMed] [Google Scholar]
- Schwartz SJ, Pantin H, Sullivan S, Prado G, Szapocznik J. Nativity and years in the receiving culture as markers of acculturation in ethnic enclaves. Journal of Cross-Cultural Psychology. 2006;37(3):345–353. doi: 10.1177/0022022106286928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz SJ, Unger JB, Zamboanga BL, Szapocznik J. Rethinking the concept of acculturation: Implications for theory and research. American Psychologist. 2010;65(4):237–251. doi: 10.1037/a0019330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith KW, McGraw SA, Carrillo JE. Factors affecting cigarette smoking and intention to smoke among Puerto Rican-American high school students. Hispanic Journal of Behavioral Sciences. 1991;13(4):401–411. [Google Scholar]
- Smith KW, McGraw SA. Smoking behavior of Puerto Rican women: Evidence from caretakers of adolescents in two urban areas. Hispanic Journal of Behavioral Sciences. 1993;15(1):140–149. [Google Scholar]
- Sutton AJ. Publication bias. In: Cooper H, Hedges LV, Valentine JC, editors. The handbook of research synthesis and meta-analysis. New York: Russell Sage Foundation; 2009. pp. 435–452. [Google Scholar]
- Sundquist J, Winkleby MA. Cardiovascular risk factors in Mexican American adults: A transcultural analysis of NHANES III, 1988-1994. American Journal of Public Health. 1999;89(5):723–730. doi: 10.2105/ajph.89.5.723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomson MD, Hoffman-Goetz L. Defining and measuring acculturation: A systematic review of public health studies with Hispanic populations in the United States. Social Science & Medicine. 2009;69:983–991. doi: 10.1016/j.socscimed.2009.05.011. [DOI] [PubMed] [Google Scholar]
- Tonin SL. Doctoral dissertation. 2006. The relationship among acculturation, gender, attitudes towards drugs, and substance use among Hispanic eighth graders. Available from PsychInfo. (UMI no. 3217478) [Google Scholar]
- Torres L, Driscoll MW, Voell M. Discrimination, acculturation, acculturative stress, and Latino psychological distress: a moderated meditational model. Cultural Diversity Ethnic Minority Psychology. 2012;18(1):17–25. doi: 10.1037/a0026710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trinidad DR, Gilpin EA, Messer K, White MM, Pierce JP. Trends in smoking among Hispanic women in California: Relationship to English language use. American Journal of Preventive Medicine. 2006;31(3):257–260. doi: 10.1016/j.amepre.2006.04.009. [DOI] [PubMed] [Google Scholar]
- Unger JB, Ritt-Olson A, Wagner KD, Soto DW, Baezconde-Garbanati L. Parent-child acculturation patterns and substance use among Hispanic adolescents: A longitudinal analysis. Journal of Primary Prevention. 2009;30(3-4):293–313. doi: 10.1007/s10935-009-0178-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varona P, Chang M, Garcia RG, Bonet M. Tobacco and alcohol use in Cuban women. MEDICC Review. 2011;13(4):38–44. doi: 10.37757/MR2011V13.N4.8. [DOI] [PubMed] [Google Scholar]
- Wallace PM, Pomery EA, Latimer AE, Martinez JL, Salovey P. A review of acculturation measures and their utility in studies promoting Latino health. Hispanic Journal of Behavioral Sciences. 2010;31(1):37–54. doi: 10.1177/0739986309352341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilkinson AV, Spitz MR, Strom SS, Prokhorov AV, Barcenas CH, Cao Y, Bondy LM. Effects of nativity, age at migration, and acculturation on smoking among adult Houston residents of Mexican descent. American Journal of Public Health. 2005;95(6):1043–1049. doi: 10.2105/AJPH.2004.055319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zea MC, Asner-Self KK, Birman D, Buki LP. The abbreviated multidimensional acculturation scale: Empirical validation with two Latino/Latina samples. Cultural Diversity and Ethnic Minority Psychology. 2003;9(2):107–126. doi: 10.1037/1099-9809.9.2.107. [DOI] [PubMed] [Google Scholar]