

Abstract
Background
We evaluated the prevalence of sarcopenia, presarcopenia, and severe sarcopenia in healthy Korean elderly women.
Methods
We measured the muscle mass and muscle function of 196 ambulatory women over the age of 65 years who visited the University Hospital Menopause Clinic. Appendicular skeletal muscle mass was measured by dual energy X-ray absorptiometry to measure skeletal muscle mass index (SMI). Assessment of hand grip strength (HGS) of the dominant hand was performed to measure the muscle strength, and 4-m straight on-way path was used to measure gait speed for physical performance. The values used to define the presarcopenia, sarcopenia, and severe sarcopenia were based on the cutoff values proposed by the Asian Working Group for Sarcopenia (AWGS).
Results
The mean age of women was 71.2 years, and the mean SMI in 196 women was 5.94 kg/m2. The average HGS was 20.3 kg, and the mean gait speed was 1.08 m/sec. In 41 out of the 196 women (20.9%), the SMI was reduced to less than 5.4 kg/m2. Fifty-nine women (30.1%) had HGS of less than 18 kg, and gait speed was less than 0.8 m/sec in 12 women (6.1%). Twenty-six women (13.3%) were classified into the presarcopenia stage, and 15 women (7.6%) were classified into the sarcopenia stage. There was no case of severe sarcopenia.
Conclusions
One out of five relatively healthy women aged more than 65 years showed a decrease in muscle mass, and 7.6% of women showed a decrease in muscle mass and strength. The sarcopenia stage was also intensified with aging.
Keywords: Prevalence, Sarcopenia, Skeletal muscle
INTRODUCTION
The prevalence and measurable impact of sarcopenia depends crucially on how sarcopenia is defined. A proper definition is the necessary base for clinical diagnosis and development of tailored treatment.
The most commonly used definition of sarcopenia is the one proposed by the European Working Group on Sarcopenia in Older People (EWGSOP).[1] The EWGSOP definition included measurements of muscle mass, muscle strength, and physical performance for the diagnosis of sarcopenia. However, the cutoff points of the EWGSOP sarcopenia criteria were based on the white population. The EWGSOP-suggested definition of sarcopenia should be evaluated for its clinical implications in other populations, including the Asian population.
The sarcopenia experts and researchers from some Asian countries including South Korea organized the Asian Working Group for Sarcopenia (AWGS). This group proposed a diagnostic algorithm based on the currently available evidence in Asia. Although recommended approaches for measurements of muscle mass, muscle strength, and physical performance by AWGS are similar to the EWGSOP definition, the cutoff values proposed by AWGS are different from those proposed by EWGSOP considering the difference in ethnicities, body size, lifestyles, and cultural background.[2]
In this study, we evaluated the prevalence of presarcopenia, sarcopenia, and severe sarcopenia in healthy Korean elderly women. The cutoff values used to define were based on the values proposed by AWGS.
METHDOS
1. Materials
From December 2011 to June 2014, we measured the muscle mass and muscle function (muscle strength and physical performance) of 196 ambulatory women over the age of 65 years who visited the University Hospital Menopause Clinic. This study was approved by the Institutional Review Board of Chung-Ang University Hospital. All subjects provided their informed consent.
2. Methods
1) Muscle mass
The AWGS recommended using height-adjusted appendicular skeletal muscle mass (skeletal muscle mass index, SMI), and suggested cutoff values of 5.4 kg/m2 for women by using dual energy X-ray absorptiometry (DXA). Appendicular skeletal muscle mass was measured by DXA (Lunar Prodigy Advance, GE Lunar, Medison, WI, USA). Appendicular skeletal muscle mass was calculated as the sum of the lean soft tissue mass in both arms and legs.
2) Muscle strength
The AWGS recommended using the lower 20th percentile of handgrip strength in the study population as the cutoff value for low muscle strength. Low handgrip strength was defined as <18 kg for women by AWGS. Assessment of hand grip strength (HGS) of the dominant hand was performed according to the standardised testing procedure of the American Society of Hand Therapists with the Jamar hand-held dynamometer (Sammons Preston Inc., Bolingbrook, IL, USA), which has been established as a reliable measure in community-dwelling older adults.[3] The individuals were seated with their shoulders adducted, their elbows flexed at 90°, and their forearms in neutral position. The mean of the three trials was recorded in kg.[4]
3) Physical performance
The AWGS suggested using ≤0.8 m/sec as the cutoff for low physical performance with 6 m gait speed for measurement of physical performance. In this study, 4-m straight on-way path was used for measurement of gait speed. Participants were asked to walk 4 m at their usual pace. Participants completed one practice and then two timed trials. Raw scores were recorded as the time in seconds required to walk four meters on each of the two trials, with the better trial used for scoring.[5]
4) Definition of presarcopenia, sarcopenia, and severe sarcopenia
The 'presarcopenia' stage was characterized by low muscle mass without impact on muscle strength or physical performance. The 'sarcopenia' stage was characterized by low muscle mass, plus low muscle strength or low physical performance. 'Severe sarcopenia' was defined when all three criteria of the definition were met (low muscle mass, low muscle strength, and low physical performance) as suggested by EWGSOP.[1]
5) Statistical analysis
Data are expressed as the mean±standard deviation (SD) and as a percentage. Differences between groups were tested using a Student t-test or the Mann-Whitney test, and the χ2-test was used to test the difference in the distribution of categorical variables. A P-value <0.05 was considered statistically significant in all analyses. Data were analyzed using SPSS for Windows (version 12.0; SPSS Inc., Chicago, IL, USA).
RESULTS
The mean age of women was 71.2 years, and the mean SMI in 196 women was 5.94 kg/m2. The mean HGS was 20.3 kg, and the mean gait speed was 1.08 m/sec (Table 1). In 41 out of the 196 women (20.9%), the SMI was reduced to less than 5.4 kg/m2. Fifty-nine women (30.1%) had HGS of less than 18 kg, and gait speed was less than 0.8 m/sec in 12 women (6.1%).
Table 1. Clinical characteristics.
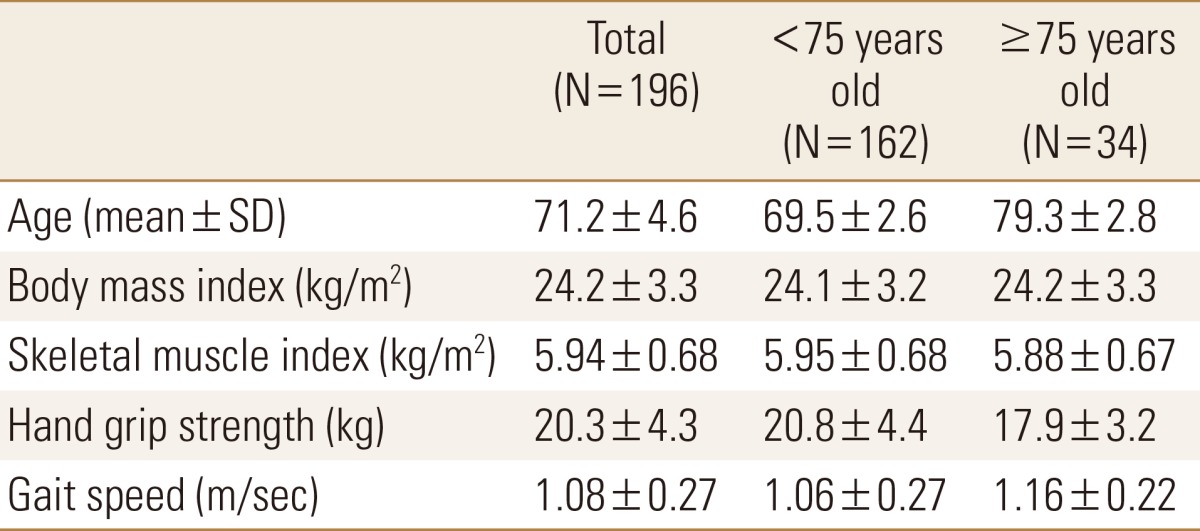
SD, standard deviation.
The target group was divided into two groups based on age 75 years and older or less than 75 years. There were a total of 162 women in the 65- to 74-year-old age group, and there were a total of 34 women in the 75 years and older age group. A reduction in SMI to less than 5.4 kg/m2 was observed in 33 women (20.4%) of the less than 75 years age group and in 8 women (23.5%) of the 75 years and older age group. Thirty-eight women (23.5%) in the less than 75 years age group and 21 women (61.8%) in the 75 years and older age group had low HGS, and 12 women (7.4%) in the less than 75 years age group and none of the women in the 75 years and older age group had low physical performance (Table 2).
Table 2. Prevalence of abnormal muscle mass and muscle function.

a)Significantly different from that in the other group.
SMI, skeletal muscle mass index; HGS, hand grip strength; GS, gate speed.
Twenty-six women (13.3%) were classified into the presarcopenia stage, which is defined as decreased muscle mass only without lower muscle strength and lower physical performance.
Sarcopenia was defined as decreased muscle mass with one of the two parameters (lower muscle strength or lower physical performance), and 15 women (7.6%) were classified into the sarcopenia stage. There was no case of severe sarcopenia, which is defined as decreased skeletal muscle mass with both parameters (lower muscle strength and lower physical performance).
According to the age groups, in the less than 75 years age group, 24 women (14.8%) had presarcopenia, 9 women (5.6%) had sarcopenia, and none of the women had severe sarcopenia. In the 75 years and older age group, 2 women (5.9%) had presarcopenia, 6 women (17.6%) had sarcopenia, and none of the women had severe sarcopenia. This finding indicated that, with an increase in age, the prevalence of sarcopenia was significantly increased compared to that of presarcopenia (P=0.032).
DISCUSSION
The term 'sarcopenia' was first used in 1995 by Rosenberg and Roubenoff [6];he made this word by combining two Greek words, Sarx (flesh) and penia (loss).
Sarcopenia initially referred to only lowered skeletal muscle mass, but itevolved as a clinical terminology combined with the concept of not only quantity of skeletal muscle mass but also quality and physical performance, then the term becomes more specific and keeps changing.
In general, sarcopenia, which appears to be related with aging, includes loss of quantity and quality of skeletal muscle.[7]
In 2010, EWGSOP suggested a clinical definition and consensus diagnostic criteria for age-related sarcopenia. The EWGSOP also suggested a conceptual staging as 'presarcopenia', 'sarcopenia', and 'severe sarcopenia' according to the status of muscle mass, muscle strength, and physical performance. However, this diagnostic strategy has been based on white population, and body size and physical performance among Asian people might differ from Caucasians, and the definitions of muscle-related parameters should be redefined within each ethnic group.
Then, the Asian Working Group for sarcopenia published a consensus report about the diagnosis of sarcopenia and strategy for sarcopenia screening and assessment. This study used the diagnostic cutoff value suggested by the AWGS.
The strength of this study is that it is the first trial performed in Korea to measure muscle function including muscle strength and physical performance as well as muscle mass and then to analyze the data based on the criteria suggested by the AWGS.
One out of five relatively healthy postmenopausal women aged more than 65 years assessed according to the cutoff value suggested by the AWGS showed decreased muscle mass (presarcopenia), and 7.6% of women had decreased muscle mass and muscle strength (sarcopenia).
The prevalence of sarcopenia was significantly increased compared to that of presarcopenia in the 75 years and older age group than in the less than 75 years age group. This indicated that the sarcopenia stage was aggravated by aging, but no case of severe sarcopenia was found.
A variety of methods for measuring muscle mass, muscle strength, and physical performance have been suggested. The EWGSOP group recommends measuring muscle mass with computed tomography (CT), magnetic resonance imaging (MRI), and bioelectrical impedance analysis (BIA) in addition to DXA. With respect to measurement of muscle strength, knee flexion/extension and peak expiratory flow can also be a measure of muscle strength besides HGS. Short physical performance battery, the timed get-up-and-go test, and the stair climb power test are recommended for measuring physical performance in addition testing the gait speed. The AWGS recommends DXA or BIA for measurement of the muscle mass and proposed the cutoff value for each method. We have to keep in mind that the prevalence of presarcopenia and sarcopenia could be different when BIA tests are used because the measurement of muscle mass in this study was based on the standard of DXA. DXA measures body composition as bone mineral content, body fat mass, and lean body mass individually. The coefficient of variation could reach 0.9% for bone mineral content, 2% for fat mass, and 0.6% for the lean body mass, which represents the muscle mass, and it is possible to perform accurate measurement as the test is repeated.[8] Measurement of muscle mass by DXA showed good agreement with the result obtained using CT or MRI in the DXA verification research. Therefore, DXA is considered the standard method for measurement of muscle mass taking into account its cost-effectiveness.[9]
HGS, a measure of the maximum voluntary force of the hand, has been described as a simple method in assessing muscle function.[10] Grip strength is used not only to describe the status of the hand but also to characterise overall upper extremity strength.[11,12] The American Society of Hand Therapists (ASHT) has recommended that grip strength should be measured using the Jamar dynamometer with its handle in the second position.[3]
Many studies have reported that HGS begins to decline when women become more than 50 years old, and it declines even further after the age of 60 years.[13,14,15,16] This study also showed lower HGS in the 75 years and older age group than in the less than 75 years age group and the prevalence of low HGS was significantly increased in the older age group whose HGS was less than 18 kg, which was the cutoff value.
Among the available physical performance measures, gait speed is suitable to be implemented in the standard clinical evaluation of older persons because it is a quick, inexpensive, reliable measure of functional capacity, with high interrater and test-retest reliability.[17,18,19]
A recent systematic review proposed a gait speed of 0.8 m/sec as a predictor of poor clinical outcomes and 0.6 m/sec as a threshold to predict further functional decline in those older adults already impaired.[20] This value is consistent with our cutoff value suggested by the AWGS.
It is known that the distance walked during the gait speed test does not affect the recorded gait speed.[21,22,23] Hence, although the AWGS suggests a cutoff value of gait speed using the 6 m gait speed test, the result obtained with the 4 m gait speed test in this study is considered to be unaffected even we used the same cutoff value suggested by the AWGS.
The first limitation of this study is that it does not represent the whole Korean elderly women population since this study targeted relatively healthy women capable of walking independently among those aged more than 65 years.
Second, the number of women enrolled in this study is not enough to predict the change according to the age, so there are limitations in analyzing the difference between the two groups because the number of women aged 75 years or older was too small. Therefore, a large-scale population-based study is necessary in the future.
Third, for measuring the gait speed, this study measured the 4 m speed rather than 6-m speed recommended by the AWGS. However, it can be considered that this does not cause any difference in the results.
In conclusion, one out of five relatively healthy women aged more than 65 years showed a decrease in muscle mass in South Korea, and 7.6% of women showed a decrease in muscle mass and strength. The sarcopenia stage was also intensified with aging, but severe sarcopenia was not observed.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39:412–423. doi: 10.1093/ageing/afq034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chen LK, Liu LK, Woo J, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc. 2014;15:95–101. doi: 10.1016/j.jamda.2013.11.025. [DOI] [PubMed] [Google Scholar]
- 3.Bohannon RW, Schaubert KL. Test-retest reliability of grip-strength measures obtained over a 12-week interval from community-dwelling elders. J Hand Ther. 2005;18:426–427. quiz 8. doi: 10.1197/j.jht.2005.07.003. [DOI] [PubMed] [Google Scholar]
- 4.Fess EE. Grip strength. In: Casanova JS, editor. Clinical assessment recommendation. 2nd ed. Chicago, IL: American Society for Hand Therapists; 1992. pp. 41–45. [Google Scholar]
- 5.Kallen M, Slotkin J, Griffith J, et al. NIH toolbox: Technical manual. 2012. [cited by 2015 April 1]. Available from: http://www.nihtoolbox.org/HowDoI/TechnicalManual/Technical%20Manual%20sections/Toolbox%204-Meter%20Walk%20Gait%20Speed%20Test%20Technical%20Manual.pdf.
- 6.Rosenberg IH, Roubenoff R. Stalking sarcopenia. Ann Intern Med. 1995;123:727–728. doi: 10.7326/0003-4819-123-9-199511010-00014. [DOI] [PubMed] [Google Scholar]
- 7.Bijlsma AY, Meskers CG, Westendorp RG, et al. Chronology of age-related disease definitions: osteoporosis and sarcopenia. Ageing Res Rev. 2012;11:320–324. doi: 10.1016/j.arr.2012.01.001. [DOI] [PubMed] [Google Scholar]
- 8.Park SW. Sarcopenia of the old age. J Korean Endocr Soc. 2007;22:1–7. [Google Scholar]
- 9.Chen Z, Wang Z, Lohman T, et al. Dual-energy X-ray absorptiometry is a valid tool for assessing skeletal muscle mass in older women. J Nutr. 2007;137:2775–2780. doi: 10.1093/jn/137.12.2775. [DOI] [PubMed] [Google Scholar]
- 10.Bohannon RW. Dynamometer measurements of hand-grip strength predict multiple outcomes. Percept Mot Skills. 2001;93:323–328. doi: 10.2466/pms.2001.93.2.323. [DOI] [PubMed] [Google Scholar]
- 11.Bohannon RW. Adequacy of hand-grip dynamometry for characterizing upper limb strength after stroke. Isokinet Exerc Sci. 2004;12:263–265. [Google Scholar]
- 12.Bohannon RW, Peolsson A, Massy-Westropp N, et al. Reference values for adult grip strength measured with a Jamar dynamometer: a descriptive meta-analysis. Physiotherapy. 2006;92:11–15. [Google Scholar]
- 13.Luna-Heredia E, Martín-Peña G, Ruiz-Galiana J. Handgrip dynamometry in healthy adults. Clin Nutr. 2005;24:250–258. doi: 10.1016/j.clnu.2004.10.007. [DOI] [PubMed] [Google Scholar]
- 14.Günther CM, Bürger A, Rickert M, et al. Grip strength in healthy caucasian adults: reference values. J Hand Surg Am. 2008;33:558–565. doi: 10.1016/j.jhsa.2008.01.008. [DOI] [PubMed] [Google Scholar]
- 15.Budziareck MB, Pureza Duarte RR, Barbosa-Silva MC. Reference values and determinants for handgrip strength in healthy subjects. Clin Nutr. 2008;27:357–362. doi: 10.1016/j.clnu.2008.03.008. [DOI] [PubMed] [Google Scholar]
- 16.Vianna LC, Oliveira RB, Araújo CG. Age-related decline in handgrip strength differs according to gender. J Strength Cond Res. 2007;21:1310–1314. doi: 10.1519/R-23156.1. [DOI] [PubMed] [Google Scholar]
- 17.Guralnik JM, Ferrucci L, Pieper CF, et al. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci. 2000;55:M221–M231. doi: 10.1093/gerona/55.4.m221. [DOI] [PubMed] [Google Scholar]
- 18.Cesari M, Kritchevsky SB, Penninx BW, et al. Prognostic value of usual gait speed in well-functioning older people--results from the Health, Aging and Body Composition Study. J Am Geriatr Soc. 2005;53:1675–1680. doi: 10.1111/j.1532-5415.2005.53501.x. [DOI] [PubMed] [Google Scholar]
- 19.Studenski S, Perera S, Wallace D, et al. Physical performance measures in the clinical setting. J Am Geriatr Soc. 2003;51:314–322. doi: 10.1046/j.1532-5415.2003.51104.x. [DOI] [PubMed] [Google Scholar]
- 20.Abellan van Kan G, Rolland Y, Andrieu S, et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J Nutr Health Aging. 2009;13:881–889. doi: 10.1007/s12603-009-0246-z. [DOI] [PubMed] [Google Scholar]
- 21.Peel NM, Kuys SS, Klein K. Gait speed as a measure in geriatric assessment in clinical settings: a systematic review. J Gerontol A Biol Sci Med Sci. 2013;68:39–46. doi: 10.1093/gerona/gls174. [DOI] [PubMed] [Google Scholar]
- 22.Bohannon RW. Population representative gait speed and its determinants. J Geriatr Phys Ther. 2008;31:49–52. doi: 10.1519/00139143-200831020-00002. [DOI] [PubMed] [Google Scholar]
- 23.Ng SS, Ng PC, Lee CY, et al. Walkway lengths for measuring walking speed in stroke rehabilitation. J Rehabil Med. 2012;44:43–46. doi: 10.2340/16501977-0906. [DOI] [PubMed] [Google Scholar]