

Abstract
Gallstone ileus of the sigmoid colon is an important, though extremely rare, cause of large bowel obstruction. The gallstone often enters the large bowel through a fistula formation between the gallbladder and colon, and impacts at a point of narrowing, causing large bowel obstruction. We describe the case of an 80-year-old woman who presented with features of bowel obstruction. Multiplanar abdominal CT demonstrated a cholecystocolonic fistula in exquisite detail. The scan also showed obstruction of the colon due to a large gallstone impacted just proximal to a stricture in the sigmoid. Owing to inflammatory adhesions and a stricture from extensive diverticular disease, the gallstone could not be retrieved. This frail and elderly woman was treated with a loop colostomy to relieve bowel obstruction. The patient made an uneventful recovery.
Background
Gallstone ileus is a rare cause of mechanical bowel obstruction and, in the majority of cases, it causes small bowel obstruction. Sigmoid gallstone ileus is even rarer. This condition mostly affects elderly patients, and is associated with high morbidity and mortality due to associated comorbidity and late presentation. One predisposing factor is recurrent bouts of inflammation of the gallbladder. It commonly occurs due to the passage of a solitary large stone through a biliary-enteric fistula into the colon. The literature has previously suggested that diagnosis is often delayed, as symptoms may be intermittent and traditional investigations might fail to identify the cause of the obstruction. We report an unusual and rare case of gallstone ileus of the sigmoid colon and review the available literature and discuss advantages of multiplanar CT in making an accurate diagnosis.1–3
Case presentation
An 80-year-old woman was admitted under the surgeons, with a 5-day history of nausea, vomiting and absolute constipation. Clinical examination revealed a tense distended abdomen with high-pitched bowel sounds.
The patient's medical history included two episodes of cholecystitis within the past year, due to gallstones, the largest of which measured 30 mm. Comorbidities, including severe vascular disease, requiring angioplasties and a left femoropopliteal polytetrafluoroethylene graft, precluded the patient from undergoing a cholecystectomy. After the first episode of cholecystitis, the patient underwent an endoscopic retrograde cholangiopancreatography with a sphincterotomy and balloon trawl, which cleared the common bile duct of multiple stones and debris.
Investigations
Biochemical and haematological investigations on admission revealed a white cell count of 10.1×109/L and a C reactive protein of 144 mg/L. Liver function tests were unremarkable.
Initial plain abdominal radiograph (figure 1) showed gaseous distension of the large bowel up to the sigmoid region and pneumobilia. No gas was visible in the rectum. The small bowel was not dilated.
Figure 1.
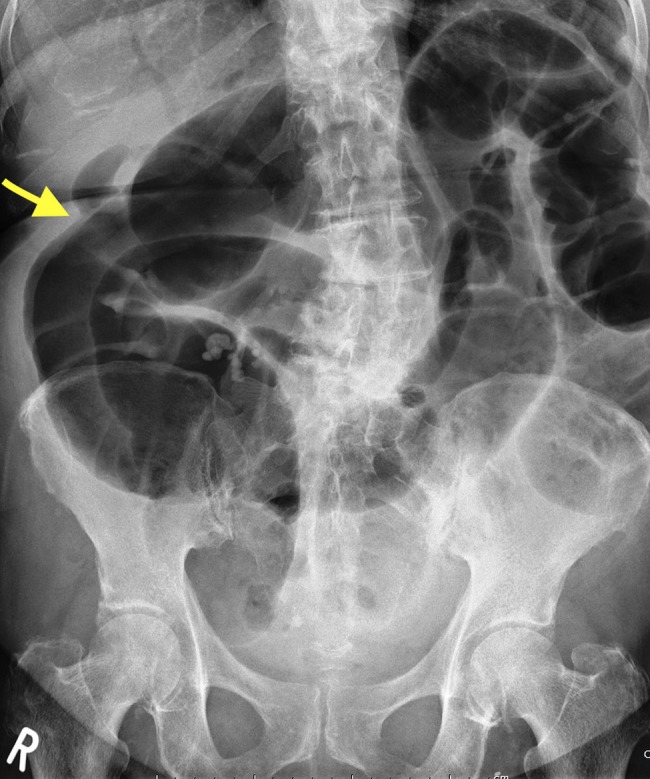
Pneumobilia—gas seen outlining the common bile duct, common hepatic duct and proximal aspects of the right and left hepatic ducts. Dilated loops of large bowel are also seen. The arrow showing the fistula between gallbladder and large bowel.
A subsequent contrast-enhanced CT scan of the abdomen demonstrated dilated loops of large bowel and a 30×24 mm non-calcified gallstone (figure 2) within the mid-sigmoid colon, which had similar appearances to a gallstone seen within the gallbladder on a previous CT from 4 years prior (figure 3). On the latest scan, the sigmoid colon was affected by extensive diverticulosis, which resulted in narrowing of lumen. Inflammatory changes were seen at the site of large bowel stricture. However, there was no abscess or collection. The small bowel was of normal calibre. Multiplanar CT reconstructions also demonstrated a cholecystocolonic fistula between the gallbladder and hepatic flexure (figures 4 and 5) along with a considerable amount of pneumobilia.
Figure 2.
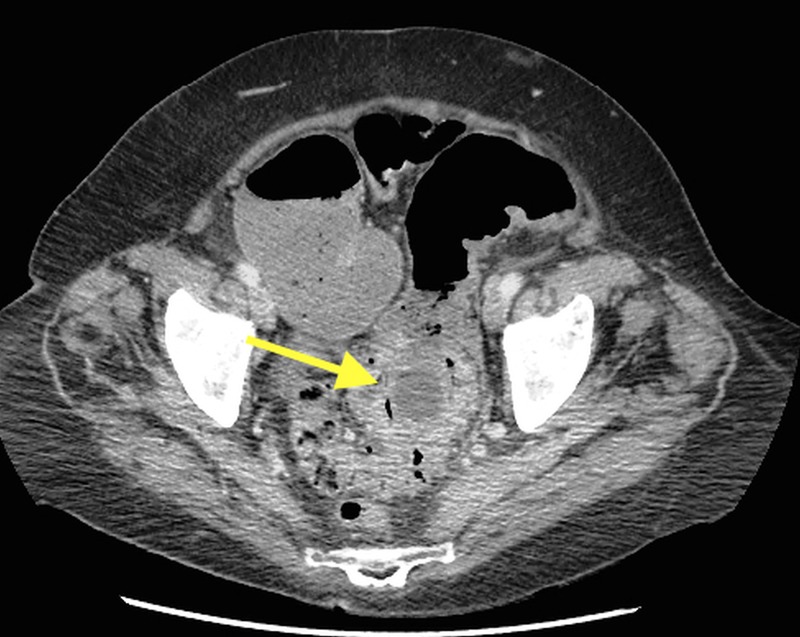
Non-calcified gallstone, measuring 30 mm, within sigmoid colon, affected by diverticular disease in 2014.
Figure 3.
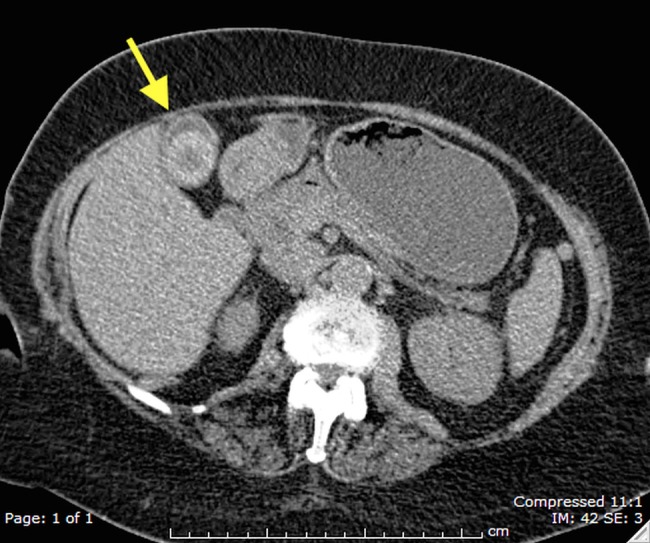
Multiple non-calcified gallstones, the largest of which measures 30 mm, in a normal gallbladder in 2010.
Figure 4.
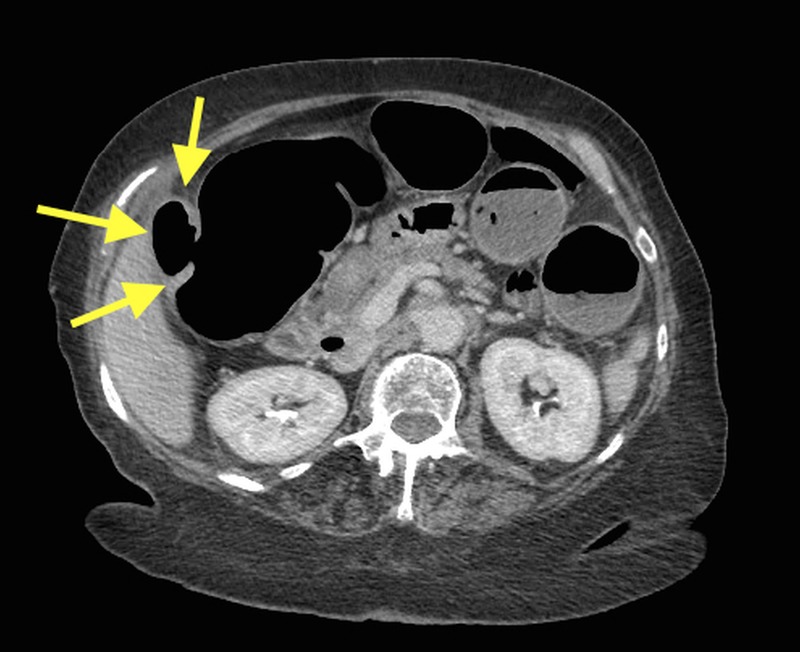
Axial slice showing cholecystocolonic fistula between gallbladder and hepatic flexure.
Figure 5.

Coronal slice showing cholecystocolonic fistula between gallbladder and hepatic flexure. Dilated loops of large bowel indicating large bowel obstruction. Pneumobilia is also visible.
Treatment
A flexible sigmoidoscopy was performed, but the scope was unable to pass beyond a tight stricture within the distal sigmoid colon. Subsequently, the patient underwent a laparotomy and a loop colostomy was formed to relieve the obstruction. Owing to other comorbidities including pelvic adhesions from extensive diverticular disease, the patient could undertake neither an enterolithotomy nor a sigmoidectomy.
Outcome and follow-up
The patient made an uneventful recovery and was discharged after a short hospital stay postsurgery. It has been over 5 months after her operation, and at the time of writing this report, she is alive and without any complications.
Discussion
Gallstone ileus is an unusual complication of cholelithiasis, occurring in <0.5% of patients. It is responsible for approximately 2–5% of all cases of mechanical intestinal obstruction. In patients over 60 years of age, it accounts for a quarter of all cases of bowel obstruction.1 2 Therefore, it is important to consider gallstone ileus in the differential diagnosis when managing an elderly patient with symptoms of intestinal obstruction. Females are 5–15 times more likely to be affected.3 4
Enterobiliary fistulae are an unusual complication associated with gallstones.5 Reported incidence of biliary fistula is around 0.1–0.5% in autopsy series and 1.5–5% in cholecystectomies. Nearly 75% of these fistulas are cholecystoduodenal, and only 10–20% are cholecystocolonic fistulae.6 A fistula can also occur secondary to Crohn's disease, peptic ulcer disease, abdominal trauma, and malignancies of the gallbladder and bowel.5 7
Gallstone ileus of the colon is an extremely rare cause of large bowel obstruction, where a calculus usually migrates via a cholecystocolonic fistula, and accounts for only 2–8% of gallstone ileus.8 9 Obstruction of bowel usually occurs in elderly women in whom there is often a pre-existing narrowing of the gut,10 11 such as diverticular stricture, shown on CT in our case. CT scan also demonstrated a cholecystocolonic fistula in exquisite detail, making a confident preoperative diagnosis of gallstone ileus of the sigmoid colon.
Rigler et al12 described the classic triad of pneumobilia, ectopic gallstone and bowel obstruction on plain radiographs; the same features are now observed on CT scan of the abdomen.13
Management of gallstone ileus of the colon depends on a number of factors, such as general fitness of the patient and comorbidities. Ideal treatment of choice is relief of bowel obstruction, cholecystectomy and repair of the fistula. In very frail patients, such as in our case, a loop colostomy is often performed to relieve symptoms. Colonoscopic extraction of gallstone has also been reported in a small number of cases.3 9 However, extraction may not be successful for stones larger than 2.5 cm or if bowel lumen is narrowed. In the case we have presented, the calculus was 3 cm in size and, due to stricture formation, colonoscopic extraction was not feasible. As this condition occurs in the elderly and presentation is often late, each case needs a careful management plan to take into consideration current clinical status and existing comorbidities.
Learning points.
It is important to consider gallstone ileus as a rare cause of large bowel obstruction in elderly women, especially those with a history of previous cholecystitis.
The use of multiplanar CT is invaluable in diagnosis of such a rare cause of large bowel obstruction. It can show the exact location of the fistula as well as the site of impaction.
This case also illustrates that, for the gallstone to impact in the large bowel, there is usually an underlying abnormality in the colon, such as diverticular stricture or malignancy, to cause gallstone ileus. Preoperative CT scan, as performed in our case, can unmask the underlying colonic pathology and will aid the surgeon in planning subsequent treatment/surgery.
Acknowledgments
The authors would like to express their thanks to radiology and surgical colleagues. They also thank Dr L Chandratreya, Mr C Wong and Mr A Dixon.
Footnotes
Twitter: Follow Tarryn Carlsson at @tazzalc
Contributors: TC was involved in design and interpretation of data, and drafting of the article. She was the radiology registrar involved in producing a final report for the patient’s CT on admission. SG was involved in reporting the patient’s CT on admission and supervised the final approval of the manuscript version to be published.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Lobo DN, Jobling JC, Balfour TW. Gallstone ileus: diagnostic pitfalls and therapeutic successes. J Clin Gastroenterol 2000;30:72–6. 10.1097/00004836-200001000-00014 [DOI] [PubMed] [Google Scholar]
- 2.Clavien PA, Richon J, Burgan S et al. Gallstone Ileus. Br J Surg 1990;77:737–42. 10.1002/bjs.1800770707 [DOI] [PubMed] [Google Scholar]
- 3.Osman N, Subar D, Loh MY et al. Gallstone ileus of the sigmoid colon: an unusual cause of large-bowel obstruction. HPB Surg 2010;2010:153740 10.1155/2010/153740 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Anseline P. Colonic gall-stone ileus. Postgrad Med J 1981;57:62–5. 10.1136/pgmj.57.663.62 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.LeBlanc KA, Barr LH, Rush BM. Spontaneous biliary enteric fistulas. South Med J 1983;76:1249–52. 10.1097/00007611-198310000-00013 [DOI] [PubMed] [Google Scholar]
- 6.Hernandez C, Heuman D, Vlahcevid ZR. Pathophysiology of disease associated with deficiency of bile acids. Principles and practice of gastroenterology and hepatology. New York. Elsevier Science Publishing, 1988:384–95. [Google Scholar]
- 7.Chandar VP, Hookman P. Choledocolonic fistula through a cystic duct remnant: a case report. Am J Gastroenterol 1980;74:179–81. [PubMed] [Google Scholar]
- 8.Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg 1994;60:441–6. [PubMed] [Google Scholar]
- 9.Roberts SR, Chang C, Chapman T et al. Colonoscopic removal of a gallstone obstructing the sigmoid colon. J Tenn Med Assoc 1990;83:18–19. [PubMed] [Google Scholar]
- 10.Papavramidis TS, Potsi S, Paramythiotis D et al. Gallstone obstructive ileus 3 years post-cholecystectomy to a patient with an old ileoileal anastomosis. J Korean Med Sci 2009;24:1216–19. 10.3346/jkms.2009.24.6.1216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Foster DR. Colonic gallstone ileus. Australas Radiol 1997;41:76–7. 10.1111/j.1440-1673.1997.tb00477.x [DOI] [PubMed] [Google Scholar]
- 12.Rigler LG, Borman CN, Noble JF. Gallstone obstruction: pathogenesis and roentgen manifestation. J Am Med Assoc 1941;117:1753–9. 10.1001/jama.1941.02820470001001 [DOI] [Google Scholar]
- 13.Key A, Dawkins A, DiSantis D. Rigler's Triad. Abdom Imaging 2015;40:229–30. 10.1007/s00261-014-0252-4 [DOI] [PubMed] [Google Scholar]